
Abstract
Purpose
To analyze a large, single-institution database to further understanding of melanoma in-transit metastases (ITM) with regard to incidence, prognosis, and the role of lymphadenectomy.
Methods
A total of 11,614 patients with single primary cutaneous melanomas were treated at Melanoma Institute Australia between January 1994 and December 2009. Of these, 505 developed ITM. Clinicopathologic characteristics, sentinel node (SN) status, patterns of disease progression, and outcomes were analyzed.
Results
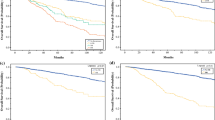
In the 505 patients with ITM, the median primary tumor thickness was 2.95 mm, and 39.4 % were ulcerated. The ITM rates for patients with primary melanomas <1 or ≥1 mm in size and in those who underwent sentinel node biopsy were 0.4, 7.8, and 7.2 %, respectively. The ITM rates for SN-positive and SN-negative patients were 21.6 and 4.7 %, respectively. The median time from primary diagnosis to the development of ITM was 17.9 months. After ITM diagnosis, the median survival time was 19.9 months, 5-year survival was 32.8 %, and 10-year survival was 27.5 %. After ITM diagnosis, primary tumor site (head/neck, trunk) and ulceration were predictors of poorer survival. Five-year survival from the time of ITM ranged from 47.9 % for nonulcerated limb primary lesions to only 13.6 % for ulcerated trunk primary lesions. Elective lymph node dissection in clinically node-negative patients with ITM did not significantly alter overall survival.
Conclusions
This large study demonstrates that the diagnosis of melanoma ITM carries serious adverse prognostic implications and will assist in improving the accuracy of staging and prognostic estimates as well as treatment in these patients.

Similar content being viewed by others


References
Coit D, Ferrone C. Recurrent regional metastases of melanoma. In: Balch C, Houghton AN, Sober AJ, Soong SJ, Atkins MA, Thompson JF, eds. Cutaneous melanoma. 5th ed. St Louis: Quality Medical Publishing; 2009. p. 487–98.
Gershenwald JE, Fidler IJ. Cancer. Targeting lymphatic metastasis. Science. 2002;296(5574):1811–2.
Zbytek B, Carlson JA, Granese J, Ross J, Mihm MC Jr, Slominski A. Current concepts of metastasis in melanoma. Expert Rev Dermatol. 2008;3:569–85.
McCarthy WH. Melanoma: margins for error—another view. ANZ J Surg. 2002;72:304–6.
Wilmott J, Haydu L, Bagot M, et al. Angiotropism is an independent predictor of microscopic satellites in primary cutaneous melanoma. Histopathology. 2012;61:889–98.
Heenan PJ, Ghaznawie M. The pathogenesis of local recurrence of melanoma at the primary excision site. Br J Plast Surg. 1999;52:209–13.
Balch CM, Gershenwald JE, Soong SJ, et al. Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol. 2009;27:6199–206.
Weide B, Faller C, Buttner P, et al. Prognostic factors of melanoma patients with satellite or in-transit metastasis at the time of stage III diagnosis. PLoS One. 2013;8:e63137.
Morton DL, Thompson JF, Cochran AJ, et al. Sentinel-node biopsy or nodal observation in melanoma. N Engl J Med. 2006;355:1307–17.
Morton DL, Thompson JF, Cochran AJ, et al. Final trial report of sentinel-node biopsy versus nodal observation in melanoma. N Engl J Med. 2014;370:599–609.
van Poll D, Thompson JF, Colman MH, et al. A sentinel node biopsy does not increase the incidence of in-transit metastasis in patients with primary cutaneous melanoma. Ann Surg Oncol. 2005;12:597–608.
Wolf IH, Richtig E, Kopera D, Kerl H. Locoregional cutaneous metastases of malignant melanoma and their management. Dermatol Surg. 2004;30(2 Pt 2):244–7.
Heenan PJ, English DR, Holman CD, Armstrong BK. The effects of surgical treatment on survival and local recurrence of cutaneous malignant melanoma. Cancer. 1992;69:421–6.
Suojarvi NJ, Jahkola TA, Virolainen S, Ilmonen SK, Hernberg MM. Outcome following local recurrence or in-transit metastases in cutaneous melanoma. Melanoma Res. 2012;22:447–53.
Kretschmer L, Beckmann I, Thoms KM, Mitteldorf C, Bertsch HP, Neumann C. Factors predicting the risk of in-transit recurrence after sentinel lymphonodectomy in patients with cutaneous malignant melanoma. Ann Surg Oncol. 2006;13:1105–12.
Pawlik TM, Ross MI, Johnson MM, et al. Predictors and natural history of in-transit melanoma after sentinel lymphadenectomy. Ann Surg Oncol. 2005;12:587–96.
Pawlik TM, Ross MI, Thompson JF, Eggermont AM, Gershenwald JE. The risk of in-transit melanoma metastasis depends on tumor biology and not the surgical approach to regional lymph nodes. J Clin Oncol. 2005;23:4588–90.
Veenstra HJ, van der Ploeg IM, Wouters MW, Kroon BB, Nieweg OE. Reevaluation of the locoregional recurrence rate in melanoma patients with a positive sentinel node compared to patients with palpable nodal involvement. Ann Surg Oncol. 2010;17:521–6.
Scoggins CR, Martin RC, Ross MI, et al. Factors associated with false-negative sentinel lymph node biopsy in melanoma patients. Ann Surg Oncol. 2010;17:709–17.
Karim RZ, Scolyer RA, Li W, et al. False negative sentinel lymph node biopsies in melanoma may result from deficiencies in nuclear medicine, surgery, or pathology. Ann Surg. 2008;247:1003–10.
Veenstra HJ, Wouters MJ, Kroon BB, Olmos RA, Nieweg OE. Less false-negative sentinel node procedures in melanoma patients with experience and proper collaboration. J Surg Oncol. 2011;104:454–7.
Miller MW, Vetto JT, Monroe MM, Weerasinghe R, Andersen PE, Gross ND. False-negative sentinel lymph node biopsy in head and neck melanoma. Otolaryngol Head Neck Surg. 2011;145:606–11.
Yee VS, Thompson JF, McKinnon JG, et al. Outcome in 846 cutaneous melanoma patients from a single center after a negative sentinel node biopsy. Ann Surg Oncol. 2005;12:429–39.
Beasley GM, Speicher P, Sharma K, et al. Efficacy of repeat sentinel lymph node biopsy in patients who develop recurrent melanoma. J Am Coll Surg. 2014;218:686–92.
Thompson JF. Local and regional therapies for melanoma: many arrows in the quiver. J Surg Oncol. 2014;109:295.
Espinosa E, Grob JJ, Dummer R, et al. Treatment algorithms in stage IV melanoma. Am J Ther. In press.
Acknowledgment
We thank Kaye Oakley for her assistance with the preparation of the article; we also gratefully acknowledge assistance from MIA colleagues. This study was supported by Melanoma Institute Australia, the Cancer Institute New South Wales, the National Health & Medical Research Council, and the Melanoma Foundation of the University of Sydney.
Disclosure
The author’s have no conflict of interest or financial disclosures.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Read, R.L., Haydu, L., Saw, R.P.M. et al. In-transit Melanoma Metastases: Incidence, Prognosis, and the Role of Lymphadenectomy. Ann Surg Oncol 22, 475–481 (2015). https://doi.org/10.1245/s10434-014-4100-0
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-014-4100-0