
Abstract
Background
Surgical margin involvement is an important outcome after pancreatic cancer surgery; however, variation in pathologic review practices may limit its use as a quality indicator. Our objectives were to assess variation in hospital performance and the reliability of margin involvement after pancreatic cancer surgery.
Methods
From the National Cancer Data Base, patients who underwent pancreatic resection for stage I to III adenocarcinoma were identified. Risk-adjusted surgical margin involvement was evaluated using hierarchical regression methods, and variation in hospital performance and reliability was determined.
Results
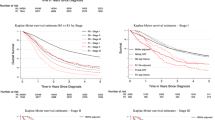
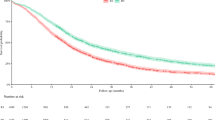
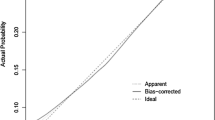
From 1,002 hospitals, 14,889 patients underwent pancreatic resection for adenocarcinoma, and 3,573 (24.0 %) had an involved surgical margin (R1 22.8 %; R2 1.2 %). The strongest predictors associated with margin involvement were T stage [T3: odds ratio (OR) 2.08, 95 % confidence interval (CI) 1.68–2.59; T4: OR 7.26, 95 % CI 5.50–9.60; vs. T1] and tumor size (2–3.9 cm: OR 1.66, 95 % CI 1.39–1.98, ≥4 cm: OR 2.28, 95 % CI 1.90–2.74; vs. <2 cm). Factors associated with a decreased likelihood of margin involvement were the use of neoadjuvant therapy and hospital type (academic and National Cancer Institute-designated comprehensive cancer centers vs. community). At the hospital level, the mean risk-adjusted surgical margin involvement rate was 25.9 % and ranged 10.1 to 50.5 %. Twenty-one (2.1 %) hospitals had lower-than-expected and 17 (1.7 %) had higher-than-expected margin involvement. A minimum acceptable reliability of 0.4 was met after 13 cases and was achieved by 249 hospitals that performed 79 % of pancreatic resections assessed.
Conclusions
Despite differences in pathologic evaluation practices, hospitals can be feasibly and reliably provided comparative data on surgical margin status after resection for pancreatic cancer.



Similar content being viewed by others
References
Department of Health and Human Services. Centers for Medicare and Medicaid Services. Fed Reg. 77(170). http://www.gpo.gov. Accessed 17 April 2013.
US Department of Health and Human Services. Hospital compare. http://www.hospitalcompare.hhs.gov/. Accessed 1 Feb 2013.
Hewitt ME, Simone JV, US National Cancer Policy Board. Ensuring quality cancer care. Washington: National Academies Press; 1999.
Wasif N, Cormier JN, Ko CY, et al. Quality measurement in cancer care delivery. Ann Surg Oncol. 2011;18:611–8.
Spinks TE, Walters R, Feeley TW, et al. Improving cancer care through public reporting of meaningful quality measures. Health Aff (Millwood). 2011;30:664–72.
Bilimoria KY, Bentrem DJ, Lillemoe KD, Talamonti MS, Ko CY. Assessment of pancreatic cancer care in the United States based on formally developed quality indicators. J Natl Cancer Inst. 2009;101:848–59.
Adams RB, Allen PJ. Surgical treatment of resectable and borderline resectable pancreatic cancer: expert consensus statement by Evans et al. Ann Surg Oncol. 2009;16:1745–50.
Evans DB, Farnell MB, Lillemoe KD, Vollmer C Jr, Strasberg SM, Schulick RD. Surgical treatment of resectable and borderline resectable pancreas cancer: expert consensus statement. Ann Surg Oncol. 2009;16:1736–44.
Bilimoria KY, Talamonti MS, Sener SF, et al. Effect of hospital volume on margin status after pancreaticoduodenectomy for cancer. J Am Coll Surg. 2008;207:510–9.
Neoptolemos JP, Stocken DD, Dunn JA, et al. Influence of resection margins on survival for patients with pancreatic cancer treated by adjuvant chemoradiation and/or chemotherapy in the ESPAC-1 randomized controlled trial. Ann Surg. 2001;234:758–68.
Konstantinidis IT, Warshaw AL, Allen JN, et al. Pancreatic ductal adenocarcinoma: is there a survival difference for R1 resections versus locally advanced unresectable tumors? What is a “true” R0 resection? Ann Surg. 2013;257:731–6.
Oettle H, Post S, Neuhaus P, et al. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA. 2007;297:267–77.
Verbeke CS, Gladhaug IP. Resection margin involvement and tumour origin in pancreatic head cancer. Br J Surg. 2012;99:1036–49.
Katz MH, Merchant NB, Brower S, et al. Standardization of surgical and pathologic variables is needed in multicenter trials of adjuvant therapy for pancreatic cancer: results from the ACOSOG Z5031 trial. Ann Surg Oncol. 2011;18:337–44.
Hall BL, Hamilton BH, Richards K, Bilimoria KY, Cohen ME, Ko CY. Does surgical quality improve in the American College of Surgeons National Surgical Quality Improvement Program: an evaluation of all participating hospitals. Ann Surg. 2009;250:363–76.
Chassin MR. Achieving and sustaining improved quality: lessons from New York State and cardiac surgery. Health Aff (Millwood). 2002;21:40–51.
American College of Surgeons, Cancer Programs. The National Cancer Data Base participant user files. http://www.facs.org/cancer/ncdb/. Accessed 20 June 2012.
Bilimoria KY, Stewart AK, Winchester DP, Ko CY. The National Cancer Data Base: a powerful initiative to improve cancer care in the United States. Ann Surg Oncol. 2008;15:683–90.
Merkow RP, Bilimoria KY. Currently available quality improvement initiatives in surgical oncology. Surg Oncol Clin N Am. 2012;21:367–75.
Cancer Program Standards. 2012. Version 1.1. Ensuring patient-centered care. http://www.facs.org/cancer/coc/programstandards2012.html. Accessed 17 April 2013.
Fritz A, Percy C, Jack A, Shanmugarathnam K, Sobin L, Parkin DM, Whelan S, eds. International classification of disease for oncology. 3rd ed. Geneva: World Health Organization; 2000.
American Joint Committee on Cancer. AJCC cancer staging manual. 7th ed. Chicago, Springer, 2010.
Commission on Cancer. Cancer program accreditation. http://www.facs.org/cancer/coc/categories3.html. Accessed 12 July, 2013.
Greenland S. Principles of multilevel modelling. Int J Epidemiol. 2000;29:158–67.
Cohen ME, Ko CY, Bilimoria KY, et al. Optimizing ACS NSQIP modeling for evaluation of surgical quality and risk: Patient risk adjustment, procedure mix adjustment, shrinkage adjustment, and surgical focus. J Am Coll Surg. 2013;217:336–346.
Agency for Healthcare Research and Quality (AHRQ). QualityNet. http://www.qualitynet.org/. Accessed 17 April 2013.
Merkow RP, Hall BL, Cohen ME, et al. Validity and feasibility of the American College of Surgeons colectomy composite outcome quality measure. Ann Surg. 2013;257:483–9.
Adams J. RAND corporation: the reliability of provider profiling. http://www.rand.org/pubs/technical_reports/TR653.html. Accessed 15 July 2013.
National Quality Forum. Measurement application partnership: performance measurement coordination strategy for PPS-exempt cancer hospitals. June 2012. http://www.qualityforum.org/Publications/2012/06/Performance_Measurement_Coordination_Strategy_for_PPS-Exempt_Cancer_Hospitals.aspx. Accessed 15 July 2013.
National Quality Forum. Measure application partnership pre-rulemaking report—February 2013. http://www.qualityforum.org/Publications/2013/02/MAP_Pre-Rulemaking_Report_-_February_2013.aspx. Accessed 15 July 2013.
National Quality Forum. http://www.qualityforum.org. Accessed 1 Feb 2013.
Adams JL, Mehrotra A, Thomas JW, McGlynn EA. Physician cost profiling—reliability and risk of misclassification. N Engl J Med. 2010;362:1014–21.
Maksymov V, Hogan M, Khalifa MA. An anatomical-based mapping analysis of the pancreaticoduodenectomy retroperitoneal margin highlights the urgent need for standardized assessment. HPB. 2013;15:218–23.
College of American Pathologists. http://www.cap.org/. Accessed 1 July, 2013.
John BJ, Naik P, Ironside A, et al. Redefining the R1 resection for pancreatic ductal adenocarcinoma: tumour lymph nodal burden and lymph node ratio are the only prognostic factors associated with survival. HPB. 2013;15:674–80.
Kimbrough CW, St Hill CR, Martin RC, McMasters KM, Scoggins CR. Tumor-positive resection margins reflect an aggressive tumor biology in pancreatic cancer. J Surg Oncol. 2013;107:602–7.
Acknowledgment
RPM is supported by the American College of Surgeons Clinical Scholars in Residence Program, the Northwestern Institute for Comparative Effectiveness Research (NICER) in Oncology, and the American Cancer Society-Illinois Division Cancer Control and Population Science Grant.
Disclosure
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Merkow, R.P., Bilimoria, K.Y., Bentrem, D.J. et al. National Assessment of Margin Status as a Quality Indicator after Pancreatic Cancer Surgery. Ann Surg Oncol 21, 1067–1074 (2014). https://doi.org/10.1245/s10434-013-3338-2
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-013-3338-2