
Abstract
Background
In cases where breast conservative surgery was performed for infiltrative ductal carcinoma (IDC), margin status is an independent prognostic factor for local ipsilateral relapse (LIR). There is no validated definition of a clear margin. We investigated factors associated with residual disease on re-excision specimen and the impact of margin status on the risk of LIR.
Methods
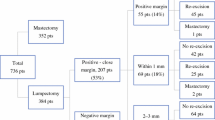
From January 1992 to December 2002, 454 patients were retrospectively included. Patients had undergone conservative surgery and radiotherapy for IDC. Two groups were defined: group 1, involved or close margin (<3 mm) and a re-excision; and group 2, involved or close margin without re-excision. The risk factors for residual disease in the re-excision specimen were analyzed in group 1, and the rate of 5-year LIR was analyzed in both groups.
Results
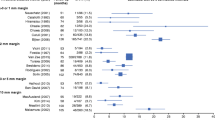
Among patients who experienced a surgical re-excision for involved or close margin, 21 % (55 of 206) had residual tumor. The multivariate analysis showed that only a margin involved with intraductal carcinoma remained predictive for residual disease. According to the multivariate analysis, only hormone therapy (p < 10−6), diffuse involved margins (p = 0.003), and margins involved with intraductal component (p < 10−6) were predictive of LIR. Re-excision for a margin involved with intraductal carcinoma significantly improved local relapse-free survival (p < 0.001).
Conclusions
In cases of IDC, re-excision for a close margin or a focally involved margin had no impact on local relapse-free survival. The decision to perform a surgical re-excision for an involved margin should not be systematic but should take multiple risk factors into consideration, such as patient age or margin diffuse involvement.


Similar content being viewed by others

References
Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, et al. Twenty years follow up of a randomized trial comparing total mastectomy, lumpectomy and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347:1233–41.
van Dongen JA, Voogd AC, Fentiman IS, Legrand C, Sylvester RJ, Tong D, et al. Long-term results of a randomized trial comparing breast-conserving therapy with mastectomy: European Organization for Research and Treatment of Cancer 10801 trial. J Natl Cancer Inst. 2000;92:1143–50.
Komoike Y, Akiyama F, Iino Y, Ikeda T, Akashi-Tanaka S, Ohsumi S, et al. Ipsilateral breast tumor relapse (IBTR) after breast-conserving treatment for early breast cancer: risk factors and impact on distant metastases. Cancer. 2006;106:35–41.
Park CC, Mitsumori M, Nixon A, Recht A, Connolly J, Gelman R, et al. Outcome at 8 years after breast-conserving surgery and radiation therapy for invasive breast cancer: influence of margin status and systemic therapy on local relapse. J Clin Oncol. 2000;18:1668–75.
Singletary SE. Surgical margins in patients with early-stage breast cancer treated with breast conservation therapy. Am J Surg. 2002;184:383–93.
Azu M, Abrahamse P, Katz SJ, Jagsi R, Morrow M. What is an adequate margin for breast-conserving surgery? Surgeon attitudes and correlates. Ann Surg Oncol. 2010;17:558–63.
McCahill LE, Single RM, Aiello Bowles EJ, Feigelson HS, James TA, Barney T, et al. Variability in reexcision following breast conservation surgery. JAMA. 2012;307:467–75.
Morrow M, Jagsi R, Alderman AK, Griggs JJ, Hawley ST, Hamilton AS, et al. Surgeon recommendations and receipt of mastectomy for treatment of breast cancer. JAMA. 2009;302:1551–6.
Morrow M, Harris JR, Schnitt SJ. Surgical margins in lumpectomy for breast cancer—bigger is not better. N Engl J Med. 2012;367:79–82.
Park CC, Mitsumori M, Nixon A, Recht A, Conolly J, Gelman R, et al. Outcome at 8 years after breast conserving surgery and radiation therapy for invasive breast cancer: influence of margin status and systemic therapy on local recurrence. J Clin Oncol. 2000;18:1668–75.
Gupta A, Subhas G, Dubay L, Silapaswan S, Kolachalam R, Kestenberg W, et al. Review of re-excision for narrow or involved margins of invasive and intraductal carcinoma. Am Surg. 2010;76:731–4.
Ward ST, Jones BG, Jewkes AJ. A two-millimetre free margin from invasive tumour minimises residual disease in breast-conserving surgery. Int J Clin Pract. 2010;64:1675–80.
Holland R, Veling SH, Mravunac M, Hendriks JH. Histologic multifocality of Tis, T1-2 breast carcinomas. Implications for clinical trials of breast-conserving surgery. Cancer. 1985;56:979–90.
Vaidya JS, Vyas JJ, Chinoy RF, Merchant N, Sharma OP, Mittra I. Multicentricity of breast cancer: whole-organ analysis and clinical implications. Br J Cancer. 1996;74:820–4.
Zavagno G, Goldin E, Mencarelli R, Capitanio G, Del Bianco P, Marconato R, et al. Role of resection margins in patients treated with breast conservation surgery. Cancer. 2008;112:1923–31.
Caughran JL, Vicini FA, Kestin LL, Dekhne NS, Benitez PR, Goldstein NS. Optimal use of re-excision in patients diagnosed with early-stage breast cancer by excisional biopsy treated with breast-conserving therapy. Ann Surg Oncol. 2009;16:3020–7.
Margenthaler JA, Gao F, Klimberg VS. Margin index: a new method for prediction of residual disease after breast-conserving surgery. Ann Surg Oncol. 2010;17:2696–701.
Cowen D, Houvenaeghel G, Bardou V, Jacquemier J, Bautrant E, Conte M, et al. Local and distant failures after limited surgery with involved margins and radiotherapy for node-negative breast cancer. Int J Radiat Oncol Biol Phys. 2000;47:305–12.
Smitt MC, Nowels K, Carlson RW, Jeffrey SS. Predictors of re-excision findings and relapse after breast conservation. Int J Radiat Oncol Biol Phys. 2003;57:979–85.
Waddel BE, Stomper PC, DeFazio JL, Hurd TC, Edge SB. Postexcision mammography is indicated after resection of ductal carcinoma-in situ of the breast. Ann Surg Oncol. 2000;7:665–8.
Grann A, Abdou JC, Dragman N, Goodman R. The value of postexcision preradiation mammography in patients with early-stage breast cancer. Am J Clin Oncol. 2004;27:285–8.
Wazer DE, Schmidt-Ullrich RK, Ruthazer R, DiPetrillo T, Boyle T, Kanski J, et al. The influence of age and extensive intraductal component histology upon breast lumpectomy margin assessment as a predictor of residual tumor. Int J Radiat Oncol Biol Phys. 1999;45:885–91.
Houssami N, Macaskill P, Marinovich ML, Dixon JM, Irwig L, Brennan ME, et al. Meta-analysis of the impact of surgical margins on local relapse in women with early-stage invasive breast cancer treated with breast-conserving therapy. Eur J Cancer. 2010;46:3219–32.
DiBiase SJ, Komarnicky LT, Schwartz GF, Xie Y, Mansfield CM. The number of involved margins influences the outcome of women treated with breast preservation for early stage breast carcinoma. Cancer. 1998;82:2212–20.
Carter D. Margins of “lumpectomy” for breast cancer. Hum Pathol. 1986;17:330–2.
Graham RA, Homer MJ, Katz J, Rothschild J, Safaii H, Supran S. The pancake phenomenon contributes to the inaccuracy of margin assessment in patients with breast cancer. Am J Surg. 2002;184:89–93.
Mirza NQ, Vlastos G, Meric F, Buchholz TA, Esnaola N, Singletary SE, et al. Predictors of locoregional relapse among patients with early-stage breast cancer treated with breast-conserving therapy. Ann Surg Oncol. 2002;9:256–65.
Acknowledgment
The authors acknowledge Joana Ashton-Chess, and ECOMOD, for English translation and Giorgio Zavagno, from Padova University, for kind comments about the manuscript.
Disclosures
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jaffré, I., Campion, L., Dejode, M. et al. Margin Width Should Not Still Enforce a Systematic Surgical Re-excision in the Conservative Treatment of Early Breast Infiltrative Ductal Carcinoma. Ann Surg Oncol 20, 3831–3838 (2013). https://doi.org/10.1245/s10434-013-3063-x
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-013-3063-x