
Abstract
Background
The tumor microenvironment after treatment with ipilimumab is not well described. Furthermore, the safety of surgery for patients being treated with ipilimumab for metastatic melanoma has not been well reported. This study analyzed the safety of surgery and the immune phenotype of tumors resected while on ipilimumab.
Methods
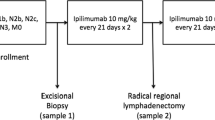
From our prospective melanoma database, we identified patients undergoing surgery for any indication within 30 days of receiving a dose of induction ipilimumab or while on maintenance ipilimumab therapy. Surgical toxicity was graded 1–5 by the Clavien classification. Tumor-infiltrating lymphocytes were classified by flow cytometry and compared with peripheral blood.
Results
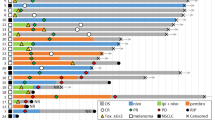
23 patients were identified who underwent 34 operations a median of 27 weeks after initiation of ipilimumab (1–123 weeks). Subcutaneous resections were the most frequent, followed by intra-abdominal and nodal procedures. Grade 1 or 2 wound complications were seen in 22 % of patients. No Grade 3–5 complications were seen. Analysis of the T cell infiltrate and matched peripheral blood from ten patients showed an elevated % of CD4+FOXP3+ T-regulatory cells and a 2.8-fold lower ratio of CD8+/CD4+FOXP3+ in the tumor compared with blood (p = 0.02). In addition, all CD8+ T cells had a higher expression of PD-1 in the tumor, compared with peripheral blood.
Conclusions
Surgery for patients on ipilimumab is safe. This study highlights the immunosuppressive phenotype in tumors not responding to immunotherapy. The high percentage of T-regulatory cells and low T-effector cells in progressive tumors suggests a possible mechanism of immune escape.


Similar content being viewed by others

References
Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363(8):711–23.
Robert C, Thomas L, Bondarenko I, et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med. 2011;364(26):2517–26.
Prieto PA, Yang JC, Sherry RM, et al. CTLA-4 blockade with ipilimumab: long-term follow-up of 177 patients with metastatic melanoma. Clin Cancer Res. 2012;18(7):2039–47.
Topalian SL, Hodi FS, Brahmer JR, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012;366(26):2443–54.
Curran MA, Montalvo W, Yagita H, Allison JP. PD-1 and CTLA-4 combination blockade expands infiltrating T cells and reduces regulatory T and myeloid cells within B16 melanoma tumors. Proc Natl Acad Sci USA. 107(9):4275–80.
Hodi FS, Butler M, Oble DA, et al. Immunologic and clinical effects of antibody blockade of cytotoxic T lymphocyte-associated antigen 4 in previously vaccinated cancer patients. Proc Natl Acad Sci USA. 2008;105(8):3005–10.
Quezada SA, Peggs KS, Curran MA, Allison JP. CTLA4 blockade and GM-CSF combination immunotherapy alters the intratumor balance of effector and regulatory T cells. J Clin Invest. 2006;116(7):1935–45.
Jacobs JF, Nierkens S, Figdor CG, de Vries IJ, Adema GJ. Regulatory T cells in melanoma: the final hurdle towards effective immunotherapy? Lancet Oncol. 2012;13(1):e32–42.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–13.
Yuan J, Page DB, Ku GY, et al. Correlation of clinical and immunological data in a metastatic melanoma patient with heterogeneous tumor responses to ipilimumab therapy. Cancer Immun. 2010;10:1.
Carthon BC, Wolchok JD, Yuan J, et al. Preoperative CTLA-4 blockade: tolerability and immune monitoring in the setting of a presurgical clinical trial. Clin Cancer Res. 2010;16(10):2861–71.
Dong H, Strome SE, Salomao DR, et al. Tumor-associated B7-H1 promotes T-cell apoptosis: a potential mechanism of immune evasion. Nat Med. 2002;8(8):793–800.
Morton DLM, N; Kashani-Sabet M, Thompson JF, Kelley MC, et al. Long-term cure after complete resection and adjuvant immunotherapy for distant melanoma metastases (Suppl abstr 8534). vol 30. Chicago: American Society of Clinical Oncology (ASCO); 2012.
Howard JH, Thompson JF, Mozzillo N, et al. Metastasectomy for distant metastatic melanoma: analysis of data from the first Multicenter Selective Lymphadenectomy Trial (MSLT-I). Ann Surg Oncol. 2012;19(8):2547–55.
Neuman HB, Patel A, Hanlon C, Wolchok JD, Houghton AN, Coit DG. Stage IV melanoma and pulmonary metastases: factors predictive of survival. Ann Surg Oncol. 2007;14(10):2847–53.
Tafra L, Dale PS, Wanek LA, Ramming KP, Morton DL. Resection and adjuvant immunotherapy for melanoma metastatic to the lung and thorax. J Thorac Cardiovasc Surg. 1995;110(1):119–28, discussion 129.
Leung AM, Hari DM, Morton DL. Surgery for distant melanoma metastasis. Cancer J. 2012;18(2):176–84.
Wong JH, Skinner KA, Kim KA, Foshag LJ, Morton DL. The role of surgery in the treatment of nonregionally recurrent melanoma. Surgery. 1993;113(4):389–94.
Wolchok JD, Hoos A, O’Day S, et al. Guidelines for the evaluation of immune therapy activity in solid tumors: immune-related response criteria. Clin Cancer Res. 2009;15(23):7412–20.
Thompson RH, Dong H, Lohse CM, et al. PD-1 is expressed by tumor-infiltrating immune cells and is associated with poor outcome for patients with renal cell carcinoma. Clin Cancer Res. 2007;13(6):1757–61.
Fourcade J, Kudela P, Sun Z, et al. PD-1 is a regulator of NY-ESO-1-specific CD8 + T cell expansion in melanoma patients. J Immunol. 2009;182(9):5240–9.
Brahmer JR, Tykodi SS, Chow LQ, et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med. 2012;366(26):2455–65.
Disclosures
CA and JW serve on advisory board for BMS; JPA is inventor of intellectual property licensed to BMS.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gyorki, D.E., Yuan, J., Mu, Z. et al. Immunological Insights from Patients Undergoing Surgery on Ipilimumab for Metastatic Melanoma. Ann Surg Oncol 20, 3106–3111 (2013). https://doi.org/10.1245/s10434-013-2999-1
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-013-2999-1