
Abstract
Background
Preoperative localization is the first step towards minimally invasive targeted parathyroidectomy. While there are data emphasizing that surgeon experience optimizes operative outcomes, the role of the radiologist’s experience in successful preoperative imaging is unclear. We hypothesized that the accuracy of sestamibi scanning for primary hyperparathyroidism is dependent upon surgeon interpretation and radiologist volume.
Methods
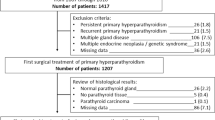
Between January 2000 to August 2009, 1,255 patients underwent parathyroidectomy for hyperparathyroidism at our institution. Of these, 763 had sestamibi scans for primary hyperparathyroidism. All scans were reviewed by surgeons and radiologists blinded, and were correlated with the operative findings and pathological reports. Radiologists were grouped into high volume (>50 cases/year, HV-RAD) or low volume (<50 cases/year, LV-RAD) based upon a database of >6,000 parathyroid cases reported by 89 regional hospitals.
Results
Of the 763 patients, 77 % were female and the mean age was 60 years. Mean baseline calcium and parathyroid hormone levels were 11.2 ± 0.03 mg/dl and 133 ± 3.27 pg/ml, respectively. The sensitivity of the surgeon (93 %) was higher than both HV (83 %) and LV (72 %) radiologists. Importantly, the positive predictive values were similar: 96 % for surgeon, 93 % for HV-RAD, and 98 % for LV-RAD. As a result, out of 99 scans which were correctly read by the surgeon but not by radiologist, 84 were read as negative by radiologist, 11 on the wrong side of the neck, and 4 on the same side but the wrong gland.
Conclusions
Surgeon interpretation and radiologist volume increase the likelihood of successful preoperative sestamibi parathyroid localization for primary hyperparathyroidism. We recommend that imaging be reviewed by experienced parathyroid surgeons rather than relying on radiological interpretation alone.

Similar content being viewed by others


References
Greene AB, Butler RS, McIntyre S, et al. National trends in parathyroid surgery from 1998 to 2008: a decade of change. J Am Coll Surg. 2009;209(3):332–43.
Westerdahl J, Bergenfelz A. Unilateral versus bilateral neck exploration for primary hyperparathyroidism: five-year follow-up of a randomized controlled trial. Ann Surg. 2007;246(6):976–80 (discussion 980–1).
Goldstein RE, Blevins L, Delbeke D, Martin WH. Effect of minimally invasive radioguided parathyroidectomy on efficacy, length of stay, and costs in the management of primary hyperparathyroidism. Ann Surg. 2000;231(5):732–42.
Chen H, Sokoll LJ, Udelsman R. Outpatient minimally invasive parathyroidectomy: a combination of sestamibi-SPECT localization, cervical block anesthesia, and intraoperative parathyroid hormone assay. Surgery. 1999;126(6):1016–21 (discussion 1021–2).
Mariani G, Gulec SA, Rubello D, et al. Preoperative localization and radioguided parathyroid surgery. J Nucl Med. 2003;44(9):1443–58.
Lal A, Chen H. The negative sestamibi scan: is a minimally invasive parathyroidectomy still possible? Ann Surg Oncol. 2007;14(8):2363–6.
Shah S, Win Z, Al-Nahhas A. Multimodality imaging of the parathyroid glands in primary hyperparathyroidism. Minerva Endocrinol. 2008;33(3):193–202.
Civelek AC, Ozalp E, Donovan P, Udelsman R. Prospective evaluation of delayed technetium-99m sestamibi SPECT scintigraphy for preoperative localization of primary hyperparathyroidism. Surgery. 2002;131(2):149–57.
Anderson SR, Vaughn A, Karakla D, Wadsworth JT. Effectiveness of surgeon interpretation of technetium tc 99m sestamibi scans in localizing parathyroid adenomas. Arch Otolaryngol Head Neck Surg. 2008;134(9):953–7.
Denham DW, Norman J. Cost-effectiveness of preoperative sestamibi scan for primary hyperparathyroidism is dependent solely upon the surgeon’s choice of operative procedure. J Am Coll Surg. 1998;186(3):293–305.
Irvin GL, Solorzano CC, Carneiro DM. Quick intraoperative parathyroid hormone assay: surgical adjunct to allow limited parathyroidectomy, improve success rate, and predict outcome. World J Surg. 2004;28(12):1287–92.
Zarebczan B, Chen H. Influence of surgical volume on operative failures for hyperparathyroidism. Adv Surg. 2011;45:237–48.
Slepavicius A, Beisa V, Janusonis V, Strupas K. Focused versus conventional parathyroidectomy for primary hyperparathyroidism: a prospective, randomized, blinded trial. Langenbecks Arch Surg. 2008;393(5):659–66.
Melton GB, Somervell H, Friedman KP, Zeiger MA, Cahid Civelek A. Interpretation of 99mTc sestamibi parathyroid SPECT scan is improved when read by the surgeon and nuclear medicine physician together. Nucl Med Commun. 2005;26(7):633–8.
Neychev VK, Kouniavsky G, Shiue Z, et al. Chasing “shadows”: discovering the subtleties of sestamibi scans to facilitate minimally invasive parathyroidectomy. World J Surg. 2011;35(1):140–6.
Chen H, Mack E, Starling JR. A comprehensive evaluation of perioperative adjuncts during minimally invasive parathyroidectomy: which is most reliable? Ann Surg. 2005;242(3):375–80 (discussion 380–3).
Chen H, Mack E, Starling JR. Radioguided parathyroidectomy is equally effective for both adenomatous and hyperplastic glands. Ann Surg. 2003;238(3):332–7 (discussion 337–8).
Chen H. Radioguided parathyroid surgery. Adv Surg. 2004;38:377–92.
Chen H, Pruhs Z, Starling JR, Mack E. Intraoperative parathyroid hormone testing improves cure rates in patients undergoing minimally invasive parathyroidectomy. Surgery. 2005;138(4):583–7 (discussion 587–90).
Elaraj DM, Sippel RS, Lindsay S, et al. Are additional localization studies and referral indicated for patients with primary hyperparathyroidism who have negative sestamibi scan results? Arch Surg. 2010;145(6):578–81.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zia, S., Sippel, R.S. & Chen, H. Sestamibi Imaging for Primary Hyperparathyroidism: The Impact of Surgeon Interpretation and Radiologist Volume. Ann Surg Oncol 19, 3827–3831 (2012). https://doi.org/10.1245/s10434-012-2581-2
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-012-2581-2