
Abstract
Purpose
We sought to examine how splenectomy as part of up-front cytoreductive surgery in ovarian cancer influences the postoperative course and affects survival.
Methods
We reviewed cases of ovarian cancer diagnosed at Massachusetts General Hospital from 1994 to 2008 and found 44 patients who had a splenectomy as part of their up-front cytoreductive surgery. These were compared to 171 patients who did not undergo splenectomy. We evaluated age at diagnosis, estimated blood loss, percentage of patients whose disease was optimally cytoreduced (<1 cm), reason for splenectomy (oncologic vs. surgical), length of stay, time to first chemotherapy treatment, and survival.
Results
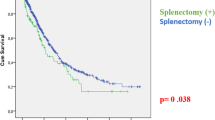
In the splenectomy cohort, the mean age at diagnosis was 64 (44–83) years. A total of 37 of 44 (84%) patients were optimally cytoreduced. Mean estimated blood loss was 1326 ml. The purpose of splenectomy was to accomplish an optimal cytoreduction (oncologic) in 82% of cases. Median length of stay was 13 (6–76) days. Median time to first chemotherapy was 13.5 (5–54) days. The median disease-free interval and overall survival of the splenectomy cohort were 8 and 30 months, respectively. The median overall survival for patients whose disease was optimally cytoreduced in the splenectomy cohort compared to the no-splenectomy group was 30 and 45 months (P < 0.045), respectively.
Conclusions
The addition of splenectomy to up-front cytoreductive surgery was feasible and safe. However, it appears to carry with it a shortened survival that is unrelated to postoperative morbidity. Our data raise the questions that splenectomy is needed for optimal cytoreduction in more biologically aggressive disease and that splenectomy may be an independent prognostic factor related to depressed immune function.


Similar content being viewed by others


References
Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–49.
Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96.
Winter WE 3rd, Maxwell GL, Tian C, et al. Prognostic factors for stage III epithelial ovarian cancer: a Gynecologic Oncology Group study. J Clin Oncol. 2007;25:3621–7.
Griffiths CT. Surgical resection of tumor bulk in the primary treatment of ovarian carcinoma. Natl Cancer Inst Monogr. 1975;42:101–4.
Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol. 2002;20:1248–59.
Eisenkop SM, Friedman RL, Wang HJ. Complete cytoreductive surgery is feasible and maximizes survival in patients with advanced epithelial ovarian cancer: a prospective study. Gynecol Oncol. 1998;69:103–8.
Chi DS, Franklin CC, Levine DA, et al. Improved optimal cytoreduction rates for stages IIIC and IV epithelial ovarian, fallopian tube, and primary peritoneal cancer: a change in surgical approach. Gynecol Oncol. 2004;94:650–4.
Eisenhauer EL, Abu-Rustum NR, Sonoda Y, et al. The addition of extensive upper abdominal surgery to achieve optimal cytoreduction improves survival in patients with stages IIIC–IV epithelial ovarian cancer. Gynecol Oncol. 2006;103:1083–90.
Kehoe SM, Eisenhauer EL, Chi DS. Upper abdominal surgical procedures: liver mobilization and diaphragm peritonectomy/resection, splenectomy, and distal pancreatectomy. Gynecol Oncol. 2008;111:S51–5.
Glockzin G, Schlitt HJ, Piso P. Peritoneal carcinomatosis: patients selection, perioperative complications and quality of life related to cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. World J Surg Oncol. 2009;7:5.
Meigs JV. Tumors of Female Pelvic Organs. New York: Macmillan Co; 1934.
Le T, Krepart GV, Lotocki RJ, Heywood MS. Does debulking surgery improve survival in biologically aggressive ovarian carcinoma? Gynecol Oncol. 1997;67:208–14.
Makar AP, Baekelandt M, Trope CG, Kristensen GB. The prognostic significance of residual disease, FIGO substage, tumor histology, and grade in patients with FIGO stage III ovarian cancer. Gynecol Oncol. 1995;56:175–80.
Covens AL. A critique of surgical cytoreduction in advanced ovarian cancer. Gynecol Oncol. 2000;78:269–74.
Eisenkop SM, Spirtos NM. What are the current surgical objectives, strategies, and technical capabilities of gynecologic oncologists treating advanced epithelial ovarian cancer? Gynecol Oncol. 2001;82:489–97.
Eisenkop SM, Spirtos NM, Lin WC. Splenectomy in the context of primary cytoreductive operations for advanced epithelial ovarian cancer. Gynecol Oncol. 2006;100:344–8.
Magtibay PM, Adams PB, Silverman MB, Cha SS, Podratz KC. Splenectomy as part of cytoreductive surgery in ovarian cancer. Gynecol Oncol. 2006;102:369–74.
Chen LM, Leuchter RS, Lagasse LD, Karlan BY. Splenectomy and surgical cytoreduction for ovarian cancer. Gynecol Oncol. 2000;77:362–8.
Sonnendecker EW, Guidozzi F, Margolius KA. Splenectomy during primary maximal cytoreductive surgery for epithelial ovarian cancer. Gynecol Oncol. 1989;35:301–6.
Kehoe SM, Eisenhauer EL, Abu-Rustum NR, et al. Incidence and management of pancreatic leaks after splenectomy with distal pancreatectomy performed during primary cytoreductive surgery for advanced ovarian, peritoneal and fallopian tube cancer. Gynecol Oncol. 2009;112:496–500.
Nicklin JL, Copeland LJ, O’Toole RV, Lewandowski GS, Vaccarello L, Havenar LP. Splenectomy as part of cytoreductive surgery for ovarian carcinoma. Gynecol Oncol. 1995;58:244–7.
Bonenkamp JJ, Hermans J, Sasako M, et al. Extended lymph-node dissection for gastric cancer. N Engl J Med. 1999;340:908–14.
Lee KY, Noh SH, Hyung WJ, et al. Impact of splenectomy for lymph node dissection on long-term surgical outcome in gastric cancer. Ann Surg Oncol. 2001;8:402–6.
Monig SP, Collet PH, Baldus SE, et al. Splenectomy in proximal gastric cancer: frequency of lymph node metastasis to the splenic hilus. J Surg Oncol. 2001;76:89–92.
Oh SJ, Hyung WJ, Li C, et al. The effect of spleen-preserving lymphadenectomy on surgical outcomes of locally advanced proximal gastric cancer. J Surg Oncol. 2009;99:275–80.
Otsuji E, Yamaguchi T, Sawai K, Ohara M, Takahashi T. End results of simultaneous splenectomy in patients undergoing total gastrectomy for gastric carcinoma. Surgery. 1996;120:40–4.
Adachi Y, Kamakura T, Mori M, Maehara Y, Sugimachi K. Role of lymph node dissection and splenectomy in node-positive gastric carcinoma. Surgery. 1994;116:837–41.
Yang K, Chen XZ, Hu JK, Zhang B, Chen ZX, Chen JP. Effectiveness and safety of splenectomy for gastric carcinoma: a meta-analysis. World J Gastroenterol. 2009;15:5352–9.
Carrere N, Abid S, Julio CH, Bloom E, Pradere B. Spleen-preserving distal pancreatectomy with excision of splenic artery and vein: a case-matched comparison with conventional distal pancreatectomy with splenectomy. World J Surg. 2007;31:375–82.
Shoup M, Brennan MF, McWhite K, Leung DH, Klimstra D, Conlon KC. The value of splenic preservation with distal pancreatectomy. Arch Surg. 2002;137:164–8.
Robinette CD, Fraumeni JF Jr. Splenectomy and subsequent mortality in veterans of the 1939–45 war. Lancet. 1977;2:127–9.
Smith TF, Johnston RB Jr. Functions of the spleen in host defense against infection. Am J Pediatr Hematol Oncol. 1979;1:355–62.
Swirski FK, Nahrendorf M, Etzrodt M, et al. Identification of splenic reservoir monocytes and their deployment to inflammatory sites. Science. 2009;325:612–6.
McGuire WP, Hoskins WJ, Brady MF, et al. Cyclophosphamide and cisplatin compared with paclitaxel and cisplatin in patients with stage III and stage IV ovarian cancer. N Engl J Med. 1996;334:1–6.
Muggia FM, Braly PS, Brady MF, et al. Phase III randomized study of cisplatin versus paclitaxel versus cisplatin and paclitaxel in patients with suboptimal stage III or IV ovarian cancer: a gynecologic oncology group study. J Clin Oncol. 2000;18:106–15.
Tangjitgamol S, Manusirivithaya S, Laopaiboon M, Lumbiganon P. Interval debulking surgery for advanced epithelial ovarian cancer. Cochrane Database Syst Rev. 2009;(10):CD006014.
Conflict of interest
All authors have no actual or potential conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
McCann, C.K., Growdon, W.B., Munro, E.G. et al. Prognostic Significance of Splenectomy as Part of Initial Cytoreductive Surgery in Ovarian Cancer. Ann Surg Oncol 18, 2912–2918 (2011). https://doi.org/10.1245/s10434-011-1661-z
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-011-1661-z