
Abstract
Background
A number of accepted criteria, including pathological tumor, node, metastasis system stage, lymph node metastasis, and tumor differentiation, predict survival in patients undergoing surgery for gastroesophageal cancer. We examined the interrelationships between standard clinicopathological factors, systemic and local inflammatory responses, tumor proliferative activity, and survival.
Methods
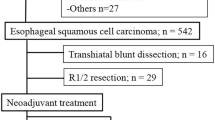
The interrelationships between the systemic inflammatory response (Glasgow prognostic score, mGPS), standard clinicopathological factors, local inflammatory response (Klintrup criteria, macrophage infiltration), and tumor proliferative activity (Ki-67) were examined by immunohistochemistry in 100 patients (44 esophageal [19 squamous, 25 adenocarcinoma], 19 junctional, and 37 gastric cancers) selected for potentially curative resection.
Results
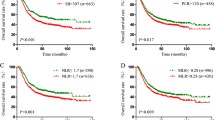
The minimum follow-up was 59 months. On multivariate survival analysis, lymph node ratio (hazard ratio [HR] 1.63, 95% confidence interval [CI] 1.11–2.40, P < 0.05), tumor differentiation (HR 2.63, 95% CI 1.45–4.77, P = 0.001), mGPS (HR 3.91, 95% CI 1.96–8.11, P < 0.001), Klintrup score (HR 3.47, 95% CI 1.14–10.55, P < 0.05), and Ki-67 (HR 0.67, 95% CI 0.47–0.96, P < 0.05) were independently associated with cancer-specific survival. A higher lymph node ratio was associated with poor tumor differentiation (P < 0.05), low-grade Klintrup criteria (P < 0.005), and low tumor proliferative activity (P < 0.05).
Conclusion
Tumor proliferation rate and local and systemic inflammatory responses are important predictors of survival, albeit in a heterogeneous cohort of patients including esophageal, junctional, and gastric cancers. These scores may be combined with accepted tumor-based factors to improve prediction of outcome.



Similar content being viewed by others

References
Cancer Research UK Information Resource Centre. CancerStats. http://infocancerresearchukorg/cancerstats. 2004.
Hundahl SA, Phillips JL, Menck HR. The National Cancer Data Base Report on poor survival of U.S. gastric carcinoma patients treated with gastrectomy: Fifth Edition American Joint Committee on Cancer staging, proximal disease, and the “different disease” hypothesis. Cancer. 2000;88:921–32.
Jamieson GG, Mathew G, Ludemann R, Wayman J, Myers JC, Devitt PG. Postoperative mortality following oesophagectomy and problems in reporting its rate. Br J Surg. 2004;91:943–7.
Siewert JR, Bottcher K, Stein HJ, Roder JD. Relevant prognostic factors in gastric cancer: ten-year results of the German Gastric Cancer Study. Ann Surg. 1998;228:449–61.
Roder JD, Busch R, Stein HJ, Fink U, Siewert JR. Ratio of invaded to removed lymph nodes as a predictor of survival in squamous cell carcinoma of the oesophagus. Br J Surg. 1994;81:410–3.
Shiu MH, Perrotti M, Brennan MF. Adenocarcinoma of the stomach: a multivariate analysis of clinical, pathologic and treatment factors. Hepatogastroenterology. 1989;36:7–12.
Robey-Cafferty SS, el-Naggar AK, Sahin AA, Bruner JM, Ro JY, Cleary KR. Prognostic factors in esophageal squamous carcinoma. A study of histologic features, blood group expression, and DNA ploidy. Am J Clin Pathol. 1991;95:844–9.
Khan OA, Alexiou C, Soomro I, Duffy JP, Morgan WE, Beggs FD. Pathological determinants of survival in node-negative oesophageal cancer. Br J Surg. 2004;91:1586–91.
Rosenwald IB. The role of translation in neoplastic transformation from a pathologist’s point of view. Oncogene. 2004;23:3230–47.
Brown DC, Gatter KC. Ki67 protein: the immaculate deception? Histopathology. 2002;40:2–11.
Solcia E, Klersy C, Mastracci L, et al. A combined histologic and molecular approach identifies three groups of gastric cancer with different prognosis. Virchows Arch. 2009;455:197–211.
Ressiot E, Dahan L, Liprandi A, et al. Predictive factors of the response to chemoradiotherapy in esophageal cancer. Gastroenterol Clin Biol. 2008;32:567–77.
McMillan DC. Systemic inflammation, nutritional status and survival in patients with cancer. Curr Opin Clin Nutr Metab Care. 2009;12:223–6.
Colotta F, Allavena P, Sica A, Garlanda C, Mantovani A. Cancer-related inflammation, the seventh hallmark of cancer: links to genetic instability. Carcinogenesis. 2009;30:1073–81.
Roxburgh CS, McMillan DC. Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol. 2010;6:149–63.
Ma XC, Hattori T, Kushima R, Terata N, Kodama M. Expression of HLA-class II antigen in gastric carcinomas. Its relationship to histopathological grade, lymphocyte infiltration and five-year survival rate. Acta Oncol. 1994;33:187–90.
Lee HE, Chae SW, Lee YJ, et al. Prognostic implications of type and density of tumour-infiltrating lymphocytes in gastric cancer. Br J Cancer. 2008;99:1704–11.
Hyakudomi M, Matsubara T, Hyakudomi R, et al. Increased expression of fractalkine is correlated with a better prognosis and an increased number of both CD8+ T cells and natural killer cells in gastric adenocarcinoma. Ann Surg Oncol. 2008;15:1775–82.
Ohno S, Inagawa H, Dhar DK, et al. The degree of macrophage infiltration into the cancer cell nest is a significant predictor of survival in gastric cancer patients. Anticancer Res. 2003;23:5015–22.
Cho Y, Miyamoto M, Kato K, et al. CD4+ and CD8+ T cells cooperate to improve prognosis of patients with esophageal squamous cell carcinoma. Cancer Res. 2003;63:1555–9.
Schumacher K, Haensch W, Roefzaad C, Schlag PM. Prognostic significance of activated CD8(+) T cell infiltrations within esophageal carcinomas. Cancer Res. 2001;61:3932–6.
Klintrup K, Mäkinen JM, Kauppila S, et al. Inflammation and prognosis in colorectal cancer. Eur J Cancer. 2005;41:2645–54.
Roxburgh CS, Salmond JM, Horgan PG, Oien KA, McMillan DC. Tumour inflammatory infiltrate predicts survival following curative resection for node-negative colorectal cancer. Eur J Cancer. 2009;45:2138–45.
Roxburgh CS, Salmond JM, Horgan PG, Oien KA, McMillan DC. Comparison of the prognostic value of inflammation-based pathologic and biochemical criteria in patients undergoing potentially curative resection for colorectal cancer. Ann Surg. 2009;249:788–93.
Nozoe T, Saeki H, Sugimachi K. Significance of preoperative elevation of serum C-reactive protein as an indicator of prognosis in esophageal carcinoma. Am J Surg. 2001;182:197–201.
Shimada H, Nabeya Y, Okazumi S, et al. Elevation of preoperative serum C-reactive protein level is related to poor prognosis in esophageal squamous cell carcinoma. J Surg Oncol. 2003;83:248–52.
Ikeda M, Natsugoe S, Ueno S, Baba M, Aikou T. Significant host- and tumor-related factors for predicting prognosis in patients with esophageal carcinoma. Ann Surg. 2003;238:197–202.
Gockel I, Dirksen K, Messow CM, Junginger T. Significance of preoperative C-reactive protein as a parameter of the perioperative course and long-term prognosis in squamous cell carcinoma and adenocarcinoma of the oesophagus. World J Gastroenterol. 2006;12:3746–50.
Crumley AB, McMillan DC, McKernan M, Going JJ, Shearer CJ, Stuart RC. An elevated C-reactive protein concentration, prior to surgery, predicts poor cancer-specific survival in patients undergoing resection for gastro-oesophageal cancer. Br J Cancer. 2006;94:1568–71.
Kobayashi T, Teruya M, Kishiki T, et al. Inflammation-based prognostic score, prior to neoadjuvant chemoradiotherapy, predicts postoperative outcome in patients with esophageal squamous cell carcinoma. Surgery. 2008;144:729–35.
Siewert JR, Stein HJ. Classification of adenocarcinoma of the oesophagogastric junction. Br J Surg. 1998;85:1457–9.
Going JJ. Efficiently estimated histologic cell counts. Hum Pathol. 1994;25:333–6.
McMillan DC. An inflammation-based prognostic score and its role in the nutrition-based management of patients with cancer. Proc Nutr Soc. 2008;67:257–62.
Lee HE, Kim MA, Lee BL, Kim WH. Low Ki-67 proliferation index is an indicator of poor prognosis in gastric cancer. J Surg Oncol. 2010;102:201–6.
Morley JE, Thomas DR, Wilson MM. Cachexia: pathophysiology and clinical relevance. Am J Clin Nutr. 2006;83:735–43.
Fearon KC, Voss AC, Hustead DS. Definition of cancer cachexia: effect of weight loss, reduced food intake, and systemic inflammation on functional status and prognosis. Am J Clin Nutr. 2006;83:1345–50.
Du Clos TW, Mold C. C-reactive protein: an activator of innate immunity and a modulator of adaptive immunity. Immunol Res. 2004;30:261–77.
Krzystek-Korpacka M, Matusiewicz M, Diakowska D, et al. Acute-phase response proteins are related to cachexia and accelerated angiogenesis in gastroesophageal cancers. Clin Chem Lab Med. 2008;46:359–64.
Vashist YK, Loos J, Dedow J, et al. Glasgow prognostic score is a predictor of perioperative and long-term outcome in patients with only surgically treated esophageal cancer. Ann Surg Oncol. In press.
Shearer CJ, Going JJ, Neilson LJ, Stuart RC. Modified classification for adenocarcinoma of the gastro-oesophageal junction. ANZ J Surg. 2007;77:544–9.
McColl KE, Going JJ. Aetiology and classification of adenocarcinoma of the gastro-oesophageal junction/cardia. Gut. 2010;59:282–4.
Proctor MJ, Morrison DS, Talwar D, et al. An inflammation-based prognostic score (mGPS) predicts cancer survival independent of tumour site: a Glasgow Inflammation Outcome Study. Br J Cancer. 2011;104:726–34.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Crumley, A.B.C., Going, J.J., Hilmy, M. et al. Interrelationships between Tumor Proliferative Activity, Leucocyte and Macrophage Infiltration, Systemic Inflammatory Response, and Survival in Patients Selected for Potentially Curative Resection for Gastroesophageal Cancer. Ann Surg Oncol 18, 2604–2612 (2011). https://doi.org/10.1245/s10434-011-1658-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-011-1658-7