
Abstract
Background
There remains a lack of consensus regarding the optimal treatment for patients with curable adenocarcinoma of the anal canal (AAC). We sought to determine the role of definitive surgical resection and radiation in a large cohort of patients with AAC.
Materials and Methods
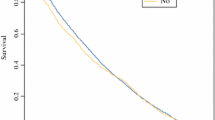
We queried the Surveillance, Epidemiology, and End Results (SEER) registry to identify all patients with nonmetastatic AAC from 1988 to 2004 and analyzed clinical factors, treatment modalities, and overall survival in this cohort. Kaplan–Meier survival curves were constructed to compare 5-year overall survival based on treatment groups: abdominal perineal resection (APR) only, APR and external beam radiation (APR and EBR), and EBR only. We performed a Cox regression analysis to determine factors predictive of outcome.
Results
A total of 165 patients were identified with nonmetastatic AAC. Of these, 30 patients were treated with an APR only, 42 patients with an APR and EBR, and 93 patients with EBR only. The 5-year survival for APR only, APR and EBR, and EBR only was 58%, 50%, and 30%, respectively. The difference in survival was statistically significant (APR vs. EBR, P = .02; APR and EBR vs. EBR, P = 0.04). Multivariate analysis completed on 86 patients in this cohort confirmed that factors accounting for the survival differences included age (P = 0.004), nodal stage (P = 0.001), and treatment groups (P = 0.03). The hazard ratio between EBR only compared with APR only was 2.78.
Conclusions
Definitive surgical treatment in the form of an APR with or without EBR is associated with improved survival in patients with AAC.


Similar content being viewed by others


Abbreviations
- AAC:
-
Adenocarcinoma of the anal canal
- SEER:
-
Surveillance, Epidemiology, and End Results registry
- EBR:
-
External beam radiation
- APR:
-
Abdominal perineal resection
References
Whiteford MH, Stevens KR, Jr., Oh S, Deveney KE. The evolving treatment of anal cancer: how are we doing? Arch Surg. 2001;136:886–91.
Morson BC, Sobin LH. Histologic typing of intestinal tumors. Geneva: WHO, 1976.
Fenger C, Morson BC. Anal duct carcinoma. Dis Colon Rectum. 1989;32:355–7.
Joon DL, Chao MW, Ngan SY, Joon ML, Guiney MJ. Primary adenocarcinoma of the anus: a retrospective analysis. Int J Radiat Oncol Biol Phys. 1999;45:1199–205.
Abel ME, Chiu YS, Russell TR, Volpe PA. Adenocarcinoma of the anal glands: results of a survey. Dis Colon Rectum. 1993;36:383–7.
Basik M, Rodriguez-Bigas MA, Penetrante R, Petrelli NJ. Prognosis and recurrence patterns of anal adenocarcinoma. Am J Surg. 1995;169:233–7.
Belkacemi Y, Berger C, Poortmans P, Piel G, Zouhair A, Meric JB, et al. Management of primary anal canal adenocarcinoma: a large retrospective study from the Rare Cancer Network. Int J Radiat Oncol Biol Phys. 2003;56:1274–83.
Surveillance, Epidemiology, and End Results (SEER) Program, (www.seer.cancer.gov) Limited-Use Data (1973-2004), National Cancer Institute, DCCPS, Surveillance Research Program, Cancer Statistics Branch, released April 2007. 7 A.D.
Fritz A, Percy C, Jack A, Shanmugaratnam K, Sobin LH, Parkin DM, Whelan S. International Classification of Diseases for Oncology. 3rd ed. Geneva: World Heath Organization, 2000.
Greene FL, Page DL, Fleming ID, Fritz AG, Balch CM. American joint committee on cancer staging manual. Philadelphia: Springer, 2002.
Myerson RJ, Karnell LH, Menck HR. The National Cancer Data Base report on carcinoma of the anus. Cancer. 1997;80:805–15.
Merlini M, Eckert P. Malignant tumors of the anus: a study of 106 cases. Am J Surg. 1985;150:370–2.
Papagikos M, Crane CH, Skibber J, Janjan NA, Feig B, Rodriguez-Bigas MA, et al. Chemoradiation for adenocarcinoma of the anus. Int J Radiat Oncol Biol Phys. 2003;55:669–78.
Behan W, Burnett R. Adenocarcinoma of the anal glands. J Clin Pathol. 1996;49:1009–11.
Hobbs CM, Lowry MA, Owen D, Sobin LH. Anal gland carcinoma. Cancer. 2001;92:2045–9.
Gaertner WB, Hagerman GF, Finne CO, Alavi K, Jessurun J, Rothenberger DA, et al. Fistula-associated anal adenocarcinoma: good results with aggressive therapy. Dis Colon Rectum. 2008;51:1061–7.
Goldstone SE, Winkler B, Ufford LJ, Alt E, Palefsky JM. High prevalence of anal squamous intraepithelial lesions and squamous-cell carcinoma in men who have sex with men as seen in a surgical practice. Dis Colon Rectum. 2001;44:690–8.
Palefsky JM, Holly EA, Ralston ML Arthur SP, Jay N, Berry JM, et al. Anal squamous intraepithelial lesions in HIV-positive and HIV-negative homosexual and bisexual men: prevalence and risk factors. J Acquir Immune Defic Syndr Hum Retrovirol. 1998;17:320–6.
Perkowski PE, Sorrells DL, Evans JT, Nopajaroonsri C, Johnson LW. Anal duct carcinoma: case report and review of the literature. Am Surg. 2000;66:1149–52.
Jensen SL, Shokouh-Amiri MH, Hagen K, Harling H, Nielsen OV Adenocarcinoma of the anal ducts. A series of 21 cases. Dis Colon Rectum. 1988;31:268–72.
Wolff P, Peiffert D. In regard to Joon et al. IJROBP 1999;45:1199–1205. Int J Radiat Oncol Biol Phys. 2001;49:1517.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kounalakis, N., Artinyan, A., Smith, D. et al. Abdominal Perineal Resection Improves Survival for Nonmetastatic Adenocarcinoma of the Anal Canal. Ann Surg Oncol 16, 1310–1315 (2009). https://doi.org/10.1245/s10434-009-0392-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-009-0392-x