
Abstract
Introduction
Lymphadenectomy and thyroidectomy is standard treatment for medullary thyroid carcinoma (MTC), but the prognostic importance of the number of lymph nodes removed (lymph node yield, LNY) and the proportion of metastatic lymph nodes resected (metastatic lymph node ratio, MLNR) is unknown. We hypothesized that MTC survival is influenced by LNY and MLNR.
Methods
Patients (N = 534) who underwent thyroidectomy with lymphadenectomy for MTC between 1988 and 2004 were identified in the Surveillance, Epidemiology, and End Results (SEER) database. The Kaplan–Meier method was used for univariate comparisons of survival for LNY and MLNR with a maximum follow-up of 12 years. Cox regression models adjusted for age, sex, extent of disease, tumor size, nodal status, LNY, and MLNR.
Results
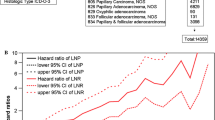
By univariate analysis, increasing LNY was associated with improved survival in all patients (P < 0.002) and node-positive patients (P < 0.001). In a multivariate analysis using LNY and MLNR as categorical variables, significant factors influencing survival included: age (P < 0.001), tumor size (P < 0.001), LNY (P = 0.007), and MLNR (P < 0.02); in node-negative patients: age (P = 0.002); in node-positive patients: age (P < 0.001), tumor size (P < 0.001), and LNY (P = 0.001). Using LNY and MLNR as continuous variables, significant factors influencing survival included: age (P < 0.001), tumor size (P < 0.001), and MLNR (P = 0.01); in node-negative patients: age (P < 0.001); in node-positive patients: age (P < 0.001) and tumor size (P < 0.001).
Conclusion
In patients undergoing thyroidectomy and lymphadenectomy for MTC, LNY and MLNR predict poorer survival, but their impact on survival was limited to node-positive patients and was otherwise dominated by the effects of age and extent of disease.



Similar content being viewed by others


References
Grozinsky-Glasberg S, Benbassat CA, et al. Medullary thyroid cancer: a retrospective analysis of a cohort treated at a single tertiary care center between 1970 and 2005. Thyroid 2007; 17:549–56.
Gulben K, Berberoglu U, Boyabatli M. Prognostic factors for sporadic medullary thyroid carcinoma. World J Surg 2006; 30:84–90.
Bhattacharyya N. A population-based analysis of survival factors in differentiated and medullary thyroid carcinoma. Otolaryngol Head Neck Surg 2003; 128:115–23.
Kebebew E, Greenspan FS, Clark OH, et al. Extent of disease and practice patterns for medullary thyroid cancer. J Am Coll Surg 2005; 200:890–6.
Leboulleux S, Travagli JP, Caillou B, et al. Medullary thyroid carcinoma as part of a multiple endocrine neoplasia type 2B syndrome: influence of the stage on the clinical course. Cancer 2002; 94:44–50.
Brierley J, Tsang R, Simpson WJ, et al. Medullary thyroid cancer: analyses of survival and prognostic factors and the role of radiation therapy in local control. Thyroid 1996; 6:305–10.
Esik O, Tusnady G, Tron L, et al. Markov model-based estimation of individual survival probability for medullary thyroid cancer patients. Pathol Oncol Res 2002; 8:93–104.
Greenblatt DY, Elson D, Mack E, et al. Initial lymph node dissection increases cure rates in patients with medullary thyroid cancer. Asian J Surg 2007; 30:108–12.
Hundahl SA, Cady B, Cunningham MP, et al. Initial results from a prospective cohort study of 5583 cases of thyroid carcinoma treated in the united states during 1996. U.S. and German Thyroid Cancer Study Group. An American College of Surgeons Commission on Cancer Patient Care Evaluation study. Cancer 2000; 89:202–17.
Brumsen C, Haak HR, Goslings BM, et al. Should patients with medullary thyroid carcinoma undergo extensive lymph node (re)operation to improve long-term survival? Henry Ford Hosp Med J 1992; 40:271–5.
Weber T, Schilling T, Frank-Raue K, et al. Impact of modified radical neck dissection on biochemical cure in medullary thyroid carcinomas. Surgery 2001; 130:1044–9.
Oskam IM, Hoebers F, Balm AJ, et al. Neck management in medullary thyroid carcinoma. Eur J Surg Oncol 2008; 34:71–6.
Moley JF, DeBenedetti MK. Patterns of nodal metastases in palpable medullary thyroid carcinoma: recommendations for extent of node dissection. Ann Surg 1999; 229:880–7; discussion 7–8.
Moley JF, Fialkowski EA. Evidence-based approach to the management of sporadic medullary thyroid carcinoma. World J Surg 2007; 31:946–56.
Green FL, Page DL, Fleming ID, et al. AJCC Cancer Staging Manual, 6th edn. 2002:77–88
Ellenhorn JD, Shah JP, Brennan MF. Impact of therapeutic regional lymph node dissection for medullary carcinoma of the thyroid gland. Surgery 1993; 114:1078–81; discussion 81–2.
Fleming JB, Lee JE, Bouvet M, et al. Surgical strategy for the treatment of medullary thyroid carcinoma. Ann Surg 1999; 230:697–707.
Kallinowski F, Buhr HJ, Meybier H, et al. Medullary carcinoma of the thyroid–therapeutic strategy derived from fifteen years of experience. Surgery 1993; 114:491–6.
Kebebew E, Ituarte PH, Siperstein AE, et al. Medullary thyroid carcinoma: clinical characteristics, treatment, prognostic factors, and a comparison of staging systems. Cancer 2000; 88:1139–48.
Machens A, Gimm O, Ukkat J, et al. Improved prediction of calcitonin normalization in medullary thyroid carcinoma patients by quantitative lymph node analysis. Cancer 2000; 88:1909–15.
Raue F. German medullary thyroid carcinoma/multiple endocrine neoplasia registry. German MTC/MEN Study Group. Medullary Thyroid Carcinoma/Multiple Endocrine Neoplasia Type 2. Langenbecks Arch Surg 1998; 383:334–6.
van Heerden JA, Grant CS, Gharib H, et al. Long-term course of patients with persistent hypercalcitoninemia after apparent curative primary surgery for medullary thyroid carcinoma. Ann Surg 1990; 212:395–400; discussion 400–1.
Pelizzo MR, Boschin IM, Bernante P, et al. Natural history, diagnosis, treatment and outcome of medullary thyroid cancer: 37 years experience on 157 patients. Eur J Surg Oncol 2007; 33:493–7.
Dralle H, Damm I, Scheumann GF, et al. Compartment-oriented microdissection of regional lymph nodes in medullary thyroid carcinoma. Surg Today 1994; 24:112–21.
Machens A, Holzhausen HJ, Dralle H. Contralateral cervical and mediastinal lymph node metastasis in medullary thyroid cancer: systemic disease? Surgery 2006; 139:28–32.
American Association of Clinical Endocrinologists and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocr Pract 2006; 12:63–102
Fialkowski E, Debenedetti M, Moley J. Long-term outcome of reoperations for medullary thyroid carcinoma. World J Surg 2008; 32:754–65.
Hundahl SA, Fleming ID, Fremgen AM, et al. A National Cancer Data Base report on 53,856 cases of thyroid carcinoma treated in the U.S., 1985–1995 [see comments]. Cancer 1998; 83:2638–48.
Acknowledgements
The authors wish to thank Dr. Scott A. Hundahl, VA Northern California Health Care System, Mather, California for his kind review of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by Grant Number KL2RR024144 from the National Center for Research Resources. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Presented in part at the 3rd Annual Academic Surgical Congress, February 12–15, 2008, Huntington Beach, California.
Rights and permissions
About this article
Cite this article
Leggett, M.D., Chen, S.L., Schneider, P.D. et al. Prognostic Value of Lymph Node Yield and Metastatic Lymph Node Ratio in Medullary Thyroid Carcinoma. Ann Surg Oncol 15, 2493–2499 (2008). https://doi.org/10.1245/s10434-008-0022-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-008-0022-z