
Abstract
Background
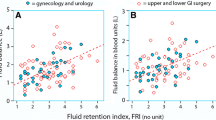
Ascites is common in patients with advanced ovarian carcinoma (AOC). Its drainage during surgery affects plasma proteins. We sought to correlate the volume of ascites with the oncological parameters of the disease, calculate its drainage effect on plasma proteins, and determine the necessary substitution requirements and a clinical way of achieving that.
Patients and Methods
We evaluated 138 patients with AOC and ascites who underwent primary cytoreductive surgery. Intraoperatively found ascites and its postoperative production were evaluated. Its drainage effect on plasma proteins and the substitution requirements were determined using a mathematic formula. Human albumin(HA) and fresh frozen plasma (FFP) were used to cover these requirements.
Results
The intraoperative ascites was found to correlate only with the stage of the disease, while its postoperative production correlated with the residual disease. Optimally debulked patients had a mean ascites production of 128 mL on postoperative day 1 compared with 668 mL of the suboptimally debulked. This production required 3 and 5–7 days, respectively, to drop <50 mL. Plasma proteins fell on their minimum level (88.9 versus 80.8%) on the second postoperative day. The protein deficit was calculated to be 379 and 691 g/day, respectively. This deficit was substituted by administering 2 HA and 2 FFP for 3–6 days.
Conclusions
Ascites drainage affects the postoperative homeostasis of plasma proteins. A mean acute drop of 12–20% is monitored on postoperative day 2. This deficit can be managed with HA and FFP for a minimum of 3 days.




Similar content being viewed by others


References
Garrison RN, Galloway RH, Heuser LS. Mechanisms of malignant ascites production. J Surg Res 1987; 42(2):126–32
Heuser LS, Miller FN, Gilley-Pietsch C. Protein leak from normal vasculature due to the malignant ascites. Am J Surg 1988; 155(6):765–9
Chu CS, Rubin SC. Management of intestinal obstruction in the terminal patient and management of ascites. In Gershenson D, Mc Guire W, Gore M, Quinn M, Thomas G (eds.) Gynecologic Cancer: Controversies in Management. Elsevier Ltd., 2004:736–7
Nagy JA, Masse EM, Herzberg KT, Meyers MS, Yeo KT, Yeo TK, Siousset TM, Dvorak HF. Pathogenesis of ascites tumor growth: vascular permeability factor, vascular hyperpermeability, and ascites fluid accumulation. Cancer Res 1995; 55(2):360–8
Wallach J. Ascites. In: Interpretation of Diagnostic Tests. Boston: Little, Brown & Co., 1975:117
Haynes GR, Navickis RJ, Wilkes MM. Albumin administration—what is the evidence of clinical benefit? A systematic review of randomized controlled trial. Eur J Anaesthesiol 2003; 20(10):771–93
Mendez CM, McClain CJ, Marsano LS. Albumin therapy in clinical practice. Nutr Clin Pract 2005; 20(3):314–20
Smorenburg CH, ter Wee PM, Gans RO. Clinical application of albumin: a closer look at indications. Ned Tijdschr Geneeskd 1997; 141(15):719–23
Vincent JL, Navickis RJ, Wilkes MM. Morbidity in hospitalized patients receiving albumin: a meta-analysis of randomized controlled trials. Crit Care Med 2004; 32(10):2029–38
Abu-Rustum NR, Richard S, Wilton A, et al. Transfusion utilization during adnexal or peritoneal cancer surgery: effects on symptomatic venous thromboembolism and survival. Gynecol Oncol 2005; 99(2):320–6
Meigs JV, Cass JW. Fibroma of the ovary with ascites and hydrothorax: report of seven cases. Am J Obstet Gynecol 1937; 33:249–67
Samanth KK, Black WC. Benign ovarian stromal tumors associated with free peritoneal fluid. Am J Obstet Gynecol 1970; 107(4):538–45
Gallagher-Allred CR, Voss AC, Finn SC, McCamish MA. Malnutrition and clinical outcomes: the case for medically nutrition therapy. J AM Diet Assoc 1996; 96:361–6
Naber TH, Schermer T, de Bree A, et al. Prevalence of malnutrition in nonsurgical hospitalized patients and its association with disease complications. Am J Clin Nutr 1997; 66:1063–4
Santoso JT, Canada T, Latson B, Aaaadi K, Lucci JA III, Coleman RL. Prognostic nutritional index in relation to hospital stay in women with gynecological cancer. Obstet Gynecol 2000; 95:844–6
Hastings GE, Wolf PG. The therapeutic use of albumin. Arch Fam Med 1992; 1(2):281–7
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vorgias, G., Iavazzo, C., Mavromatis, J. et al. Determination of the Necessary Total Protein Substitution Requirements in Patients with Advanced Stage Ovarian Cancer and Ascites, Undergoing Debulking Surgery. Correlation with Plasma Proteins. Ann Surg Oncol 14, 1919–1923 (2007). https://doi.org/10.1245/s10434-007-9404-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-007-9404-x