
Abstract
Background
Very few studies from Western centers have compared D2 and D3 dissection in the surgical treatment of gastric cancer. The aim of the prospective observational study reported here was to analyze the postoperative outcome and potential risk factors for complications following D2 and D3 lymphadenectomy.
Methods
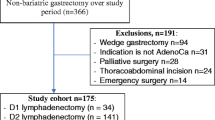
A total of 330 consecutive patients, of which 251 submitted to D2 lymphadenectomy and 79 were treated by D3 lymphadenectomy, were enrolled in the study. Twenty potential risk factors for morbidity and mortality were studied by means of univariate and multivariate analysis.
Results
Overall morbidity and mortality rates were 34% (111 patients) and 4% (14 patients), respectively. Abdominal abscess, anastomotic leakage, pleuropulmonary diseases and pancreatitis were the most commonly observed complications. No differences in morbidity, surgical morbidity, mortality rates and mean hospital stay between D2 and D3 lymphadenectomy were found. Multivariate analysis revealed that American Society of Anesthesiologists’ (ASA) class II/III versus class I, perioperative blood transfusions, and low albumin serum levels were independent predictors of postoperative complications. Age, surgical radicality (R1/R2 vs. R0) and low albumin serum levels independently predicted mortality. Mortality rate was .5% in the 203 patients aged 75 years or younger who underwent curative surgery. Most of deaths were observed in patients older than 75 years with low albumin serum levels or treated by non-curative surgery.
Conclusions
D2 lymphadenectomy represents a feasible procedure associated to acceptable morbidity and mortality rates. In specialized centers, D3 lymphadenectomy may be performed without increasing the risk of postoperative complications and associated deaths in carefully selected patients. These techniques should be avoided in subgroups of patients with a high risk of postoperative mortality.


Similar content being viewed by others


References
Sobin LH, Wittekind C. TNM Classification of Malignant Tumours, 5th edn. New York: John Wiley & Sons; 1997
Bozzetti F, Marubini E, Bonfanti G, Miceli R, Piano C, Gennari L. Subtotal versus total gastrectomy for gastric cancer: five-year survival rates in a multicenter randomized Italian trial. Italian Gastrointestinal Tumor Study Group. Ann Surg1999; 230:170–8
de Manzoni G, Verlato G, Roviello F, et al. Italian Research Group for Gastric Cancer. Subtotal versus total gastrectomy for T3 adenocarcinoma of the antrum. Gastric Cancer 2003; 6:237–42
Maruyama K, Sasako M, Kinoshita T, Sano T, Katai H. Surgical treatment for gastric cancer: the Japanese approach. Semin Oncol 1996; 23:360–8
Sano T, Sasako M, Yamamoto S, et al. Gastric cancer surgery: morbidity and mortality results from a prospective randomized controlled trial comparing D2 and extended para-aortic lymphadenectomy–Japan Clinical Oncology Group study 9501. J Clin Oncol 2004; 22:2767–73
Baxter NN, Tuttle TM. Inadequacy of lymph node staging in gastric cancer patients: a population-based study. Ann Surg Oncol 2005; 12:981–7
Brennan MF, Karpeh MS Jr. Surgery for gastric cancer: the American view. Semin Oncol 1996; 23:352–9
de Manzoni G, Verlato G, Guglielmi A, Laterza E, Genna M, Cordiano C. Prognostic significance of lymph node dissection in gastric cancer. Br J Surg 1996; 83:1604–7
Siewert JR, Bottcher K, Stein HJ, Roder JD, and the German Gastric Carcinoma Study Group. Relevant prognostic factors in gastric cancer. Ten-year results of the German Gastric Cancer Study. Ann Surg 1998; 228:449–61
Roukos DH, Lorenz M, Karakostas K, Paraschou P, Batsis C, Kappas AM. Pathological serosa and node-based classification accurately predicts gastric cancer recurrence risk and outcome, and determines potential and limitation of a Japanese-style extensive surgery for Western patients: a prospective with quality control 10-year follow-up study. Br J Cancer 2001; 84:1602–9
Roviello F, Marrelli D, Morgagni P, et al. Italian Research Group for Gastric Cancer. Survival benefit of extended D2 lymphadenectomy in gastric cancer with involvement of second level lymph nodes: a longitudinal multicenter study. Ann Surg Oncol 2002; 9:894–900
Bonenkamp JJ, Hermans J, Sasako M, et al. Dutch Gastric Cancer Group. Extended lymph-node dissection for gastric cancer. N Engl J Med 1999; 340:908–14
Cuschieri A, Weeden S, Fielding J, et al. Patient survival after D1 and D2 resections for gastric cancer: long-term results of the MRC randomized surgical trial. Surgical Co-operative Group. Br J Cancer 1999; 79:1522–30
Hartgrink HH, van de Velde CJ, Putter H, et al. Extended lymph node dissection for gastric cancer: who may benefit? Final results of the randomized Dutch gastric cancer group trial. J Clin Oncol 2004; 22:2069–77
Roukos DH, Lorenz M, Encke A. Evidence of survival benefit of extended (D2) lymphadenectomy in western patients with gastric cancer based on a new concept: a prospective long-term follow-up study. Surgery 1998; 123:573–8
Nakane Y, Okamura S, Masuya Y, Okumura S, Akehira K, Hioki K. Incidence and prognosis of para-aortic lymph node metastasis in gastric cancer. Hepatogastroenterology 1998; 45:1901–6
Maeta M, Yamashiro H, Saito H, et al. A prospective pilot study of extended (D3) and superextended para-aortic lymphadenectomy (D4) in patients with T3 or T4 gastric cancer managed by total gastrectomy. Surgery 1999; 125:325–31
Takashima S, Kosaka T. Results and controversial issues regarding a para-aortic lymph node dissection for advanced gastric cancer. Surg Today 2005; 35:425–31
Kunisaki C, Akiyama H, Nomura M, et al. Comparison of Surgical Results of D2 Versus D3 Gastrectomy (Para-Aortic Lymph Node Dissection) for Advanced Gastric Carcinoma: A Multi-Institutional Study. Ann Surg Oncol 2006; 13:836–42
Roukos DH, Kappas AM. Perspectives in the treatment of gastric cancer. Nat Clin Pract Oncol 2005; 2:98–107
Marrelli D, De Stefano A, de Manzoni G, Morgagni P, Di Leo A, Roviello F; Italian Research Group for Gastric Cancer. Prediction of recurrence after radical surgery for gastric cancer: a scoring system obtained from a prospective multicenter study. Ann Surg 2005; 241:247–55
Cunningham D, Allum WH, Stenning SP, Weeden S, for the NCRI Upper GI Cancer Clinical Studies Group. Perioperative chemotherapy in operable gastric and lower oesophageal cancer: Final results of a randomised, controlled trial (the MAGIC trial, ISRCTN 93793971). J Clin Oncol (Meeting Abstracts) 2005;23[Suppl]:4001
Fatouros M, Roukos DH, Lorenz M, Arampatzis I, Hottentrott C, Encke A, Kappas AM. Impact of spleen preservation in patients with gastric cancer. Anticancer Res 2005; 25:3023–30
Roukos DH. Adjuvant chemoradiotherapy in gastric cancer: wave goodbye to extensive surgery? Ann Surg Oncol 2002; 9:620–1
Gunther K, Horbach T, Merkel S, Meyer M, Schnell U, Klein P, Hohenberger W. D3 lymph node dissection in gastric cancer: evaluation of postoperative mortality and complications. Surg Today 2000; 30:700–5
Bostanci EB, Kayaalp C, Ozogul Y, Aydin C, Atalay F, Akoglu M. Comparison of complications after D2 and D3 dissection for gastric cancer. Eur J Surg Oncol 2004; 30:20–5
Japanese Research Society for Gastric Cancer: Japanese classification of gastric carcinoma - 1st English edition. (1995) Tokyo: Kanehara & co
Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma – 2nd English edition. Gastric Cancer 1998; 1:10–24
Marrelli D, Roviello F, De Stefano A, Vuolo G, Brandi C, Lottini M, Pinto E. Surgical treatment of gastrointestinal carcinomas in octogenarians: risk factors for complications and long-term outcome. Eur J Surg Oncol 2000; 26:371–6
Golub R, Golub RW, Cantu R Jr, Stein HD. A multivariate analysis of factors contributing to leakage of intestinal anastomoses. J Am Coll Surg 1997; 184:364–2
Kodera Y, Sasako M, Yamamoto S, Sano T, Nashimoto A, Kurita A. Gastric Cancer Surgery Study Group of Japan Clinical Oncology Group. Identification of risk factors for the development of complications following extended and superextended lymphadenectomies for gastric cancer. Br J Surg 2005; 92:1103–9
de Manzoni G, Verlato G, Roviello F, et al. Italian Research Group for Gastric Cancer. The new TNM classification of lymph node metastasis minimises stage migration problems in gastric cancer patients. Br J Cancer 2002; 87:171–4
Degiuli M, Sasako M, Ponti A, Calvo F. Survival results of a multicentre phase II study to evaluate D2 gastrectomy for gastric cancer. Br J Cancer 2004; 90:1727–32
Wu CW, Hsiung CA, Lo SS, Hsieh MC, Shia LT, Whang-Peng J. Randomized clinical trial of morbidity after D1 and D3 surgery for gastric cancer. Br J Surg 2004; 91:283–7
Kooby DA, Stockman J, Ben-Porat L, et al. Influence of transfusions on perioperative and long-term outcome in patients following hepatic resection for colorectal metastases. Ann Surg 2003; 237:860–9
Gibbs J, Cull W, Henderson W, Daley J, Hur K, Khuri SF. Preoperative serum albumin level as a predictor of operative mortality and morbidity: results from the National VA Surgical Risk Study. Arch Surg 1999; 134:36–42
Bozzetti F. Rationale and indications for preoperative feeding of malnourished surgical cancer patients. Nutrition 2002; 18:953–9
Miner TJ, Jaques DP, Karpeh MS, Brennan MF. Defining palliative surgery in patients receiving noncurative resections for gastric cancer. J Am Coll Surg 2004; 198:1013–21
Baba H, Maehara Y, Inutsuka S, Takeuchi H, Oshiro T, Adachi Y, Sugimachi K. Effectiveness of extended lymphadenectomy in noncurative gastrectomy. Am J Surg 1995; 169:261–4
Acknowledgments
This work has been supported by grant PAR 2004, University of Siena, Italy
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Marrelli, D., Pedrazzani, C., Neri, A. et al. Complications after Extended (D2) and Superextended (D3) Lymphadenectomy for Gastric Cancer: Analysis of Potential Risk Factors. Ann Surg Oncol 14, 25–33 (2007). https://doi.org/10.1245/s10434-006-9063-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-006-9063-3