
Abstract
Background
Triple-negative breast cancer (TNBC) subtype and young patient age are both associated with an increased risk of local recurrence (LR) and distant recurrence (DR). In young women with TNBC, it is unclear whether subtype or patient age is driving prognosis.
Methods
Patients treated for primary TNBC from 1998 to 2011 were identified from the breast surgery database. Clinicopathologic characteristics, treatment, and outcomes were compared between patients <40 and ≥40 years of age at diagnosis. Multivariate models were used to identify factors independently associated with LR and DR.
Results
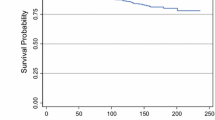
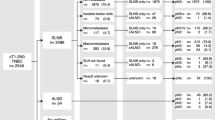
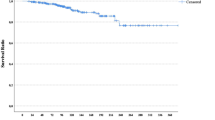
Among 1930 patients with TNBC, 289 (15 %) were <40 and 1641 (85 %) were ≥40 years of age at diagnosis. Younger patients were more likely to present with higher stage disease and more likely to receive mastectomy (p < 0.01), axillary node dissection (p < 0.01), and chemotherapy (p < 0.01). At a median follow-up of 74 (0–201.1) months, there was no difference in LR or disease-free survival (DFS) by age group [5-year LR = 3.9 % (95 % confidence interval (CI) 1.5–6.2) vs. 4.5 % (95 % CI 3.5–5.6) and 5-year DFS = 75.3 % (95 % CI 70.2–80.7) vs. 77.7 % (95 % CI 75.6–79.8), p = 0.94] in patients aged <40 and ≥40 years, respectively. On multivariate analysis, larger tumor size, lymphovascular invasion, and nodal positivity were associated with increased risk of DR. Age and type of surgery were not significantly associated with either outcome.
Conclusions
Young age at diagnosis is not an independent risk factor for LR or DR in patients with TNBC.
Similar content being viewed by others
References
Sidoni A, Cavaliere A, Bellezza G, Scheibel M, Bucciarelli E. Breast cancer in young women: clinicopathological features and biological specificity. Breast. 2003;12:247–50.
Li ZH, Xiong QY, Tu JH, et al. Tau proteins expressions in advanced breast cancer and its significance in taxane-containing neoadjuvant chemotherapy. Med Oncol. 2013;30:591.
Collins LC, Marotti JD, Gelber S, et al. Pathologic features and molecular phenotype by patient age in a large cohort of young women with breast cancer. Breast Cancer Res Treat. 2012;131:1061–6.
Xiong Q, Valero V, Kau V, et al. Female patients with breast carcinoma age 30 years and younger have a poor prognosis: the MD Anderson Cancer Center experience. Cancer. 2001;92:2523–8.
Dent R, Trudeau M, Pritchard KI, et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res. 2007;13:4429–34.
Wang SL, Li YX, Song YW, et al. Triple-negative or HER2-positive status predicts higher rates of locoregional recurrence in node-positive breast cancer patients after mastectomy. Int J Radiat Oncol Biol Phys. 2011;80:1095–101.
Montagna E, Maisonneuve P, Rotmensz N, et al. Heterogeneity of triple-negative breast cancer: histologic subtyping to inform the outcome. Clin Breast Cancer. 2013;13:31–9.
Pilewskie M, King TA. Age and molecular subtypes: impact on surgical decisions. J Surg Oncol. 2014;110:8–14.
Kim EK, Noh WC, Han W, Noh DY. Prognostic significance of young age (<35 years) by subtype based on ER, PR, and HER2 status in breast cancer: a nationwide registry-based study. World J Surg. 2011;35:1244–53.
Liedtke C, Hess KR, Karn T, et al. The prognostic impact of age in patients with triple-negative breast cancer. Breast Cancer Res Treat. 2013;138:591–9.
Ahn SH, Son BH, Kim SW, et al. Poor outcome of hormone receptor–positive breast cancer at very young age is due to tamoxifen resistance: nationwide survival data in Korea—a report from the Korean Breast Cancer Society. J Clin Oncol. 2007;25:2360–8.
Partridge AH, Hughes ME, Warner ET, et al. Subtype-dependent relationship between young age at diagnosis and breast cancer survival. J Clin Oncol. 2016;34:3308–14.
Sheridan W, Scott T, Caroline S, et al. Breast cancer in young women: have the prognostic implications of breast cancer subtypes changed over time? Breast Cancer Res Treat. 2014;147:617–29.
King TA, Pilewskie M, Morrow M. Optimal surgical management for high-risk populations. Breast. 2015;24(suppl 2):S91–5.
Cancello G, Maisonneuve P, Rotmensz N, et al. Prognosis in women with small (T1mic,T1a,T1b) node-negative operable breast cancer by immunohistochemically selected subtypes. Breast Cancer Res Treat. 2011;127:713–20.
Gangi A, Chung A, Mirocha J, Liou DZ, Leong T, Giuliano AE. Breast-conserving therapy for triple-negative breast cancer. JAMA Surg. 2014;149:252–8.
Lowery AJ, Kell MR, Glynn RW, Kerin MJ, Sweeney KJ. Locoregional recurrence after breast cancer surgery: a systematic review by receptor phenotype. Breast Cancer Res Treat. 2012;133:831–41.
Fisher B, Dignam J, Bryant J, et al. Five versus more than five years of tamoxifen therapy for breast cancer patients with negative lymph nodes and estrogen receptor–positive tumors. J Natl Cancer Inst. 1996;88:1529–42.
Dahabreh IJ, Linardou H, Siannis F, Fountzilas G, Murray S. Trastuzumab in the adjuvant treatment of early-stage breast cancer: a systematic review and meta-analysis of randomized controlled trials. Oncologist. 2008;13:620–30.
Kiess AP, McArthur HL, Mahoney K, et al. Adjuvant trastuzumab reduces locoregional recurrence in women who receive breast-conservation therapy for lymph node-negative, human epidermal growth factor receptor 2–positive breast cancer. Cancer. 2012;118:1982–8.
Abdulkarim BS, Cuartero J, Hanson J, Deschenes J, Lesniak D, Sabri S. Increased risk of locoregional recurrence for women with T1–2N0 triple-negative breast cancer treated with modified radical mastectomy without adjuvant radiation therapy compared with breast-conserving therapy. J Clin Oncol. 2011;29:2852–8.
Adkins FC, Gonzalez-Angulo AM, Lei X, et al. Triple-negative breast cancer is not a contraindication for breast conservation. Ann Surg Oncol. 2011;18:3164–73.
Zumsteg ZS, Morrow M, Arnold B, et al. Breast-conserving therapy achieves locoregional outcomes comparable to mastectomy in women with T1–2N0 triple-negative breast cancer. Ann Surg Oncol. 2013;20:3469–76.
Pilewskie M, Ho A, Orell E, et al. Effect of margin width on local recurrence in triple-negative breast cancer patients treated with breast-conserving therapy. Ann Surg Oncol. 2014;21:1209–14.
van Laar C, van der Sangen MJ, Poortmans PM, et al. Local recurrence following breast-conserving treatment in women aged 40 years or younger: trends in risk and the impact on prognosis in a population-based cohort of 1143 patients. Eur J Cancer. 2013;49:3093–101.
Coulombe G, Tyldesley S, Speers C, et al. Is mastectomy superior to breast-conserving treatment for young women? Int J Radiat Oncol Biol Phys. 2007;67:1282–90.
Kroman N, Holtveg H, Wohlfahrt J, et al. Effect of breast-conserving therapy versus radical mastectomy on prognosis for young women with breast carcinoma. Cancer. 2004;100:688–93.
Da Silva L, Lakhani SR. Pathology of hereditary breast cancer. Mod Pathol. 2010;23(suppl 2):S46–51.
Boyle P. Triple-negative breast cancer: epidemiological considerations and recommendations. Ann Oncol. 2012;23(suppl 6):vi7–12.
Greenup R, Buchanan A, Lorizio W, et al. Prevalence of BRCA mutations among women with triple-negative breast cancer (TNBC) in a genetic counseling cohort. Ann Surg Oncol. 2013;20:3254–8.
Valachis A, Nearchou AD, Lind P. Surgical management of breast cancer in BRCA-mutation carriers: a systematic review and meta-analysis. Breast Cancer Res Treat. 2014;144:443–55.
Acknowledgment
Partly funded by a Grant provided by the German academic exchange services (DAAD; Grant No. 91533303 to J.C.R.).
Disclosure
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Radosa, J.C., Eaton, A., Stempel, M. et al. Evaluation of Local and Distant Recurrence Patterns in Patients with Triple-Negative Breast Cancer According to Age. Ann Surg Oncol 24, 698–704 (2017). https://doi.org/10.1245/s10434-016-5631-3
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5631-3