
Abstract
Background
Endoscopic myringoplasty allows full visualization of the external ear canal, tympanic membrane, and middle ear without the need to reposition the patient’s head. The endoscope allows accessing hidden areas and structures not properly viewed by the microscope such as sinus tympani, facial recess, and hypotympanum. It also provides sharp, magnified image and shortens the duration of the surgery. The postoperative pain and morbidity are reduced and hence the hospital stay.
The aim of this work was to evaluate the efficacy of the endoscopic-assisted permeatal transperforation “push-through” myringoplasty by assessing the graft take rate and hearing results.
Our study included twenty patients (14 females and 6 males) with chronic suppurative otitis media without cholesteatoma that underwent endoscopic-assisted permeatal transperforation myringoplasty.
Results
The case was considered '”successful'” if there was complete healing of the tympanic membrane and improvement of hearing. Graft uptake success rates were 85% with P-value 0.132. Average air-bone gap (A-B gap) preoperative was 18.20 dB; average A-B gap 1-month postoperative was 7.75 dB.
Conclusion
Endoscopic transcanal myringoplasty provided sharp, magnified visualization and operability as it avoids retroauricular skin incision and minimizes surgical procedures to expose hidden areas. There is less bleeding, a shorter operating time, less postoperative morbidity, and minimal postoperative care.
Similar content being viewed by others


Background
Early applications of the otoendoscope was in second-look mastoidectomies to avoid postauricular incision during second-look surgery for cholesteatoma. Other applications of endoscopes in ears were examination of the middle ear recesses for residual cholesteatoma during cholesteatoma surgery, specifically the sinus tympani [1].
The role of the otoendoscope has expanded from a tool for diagnosis to the use as the sole visual device in otological surgeries. It provides a wider more comprehensive view from within with decreased tissue damage, at the expense of one-handed technique and loss of depth perception [2].
The use of the otoendoscope in myringoplasty is not only for assessment but also for the repair of the tympanic membrane perforation. It provides a sharp magnified vision. It allows the surgeon to switch easily from a close-up to wide vision just by moving the endoscope back and forth [3].
Methods
This is a prospective study that was conducted on 20 patients admitted at the Otorhinolaryngology Department, Kasr-Al Ainy Hospital, Cairo University suffering from chronic suppurative otitis media without cholesteatoma during the period from August 2019 until February 2020.
Fourteen patients were females, and six patients were males. The age of the patients ranged between 17 and 53 years. The ethical committee has given approval for this study.
Inclusion criteria
-
1.
The age of the patient should range from 15 to 60 years.
-
2.
Central perforation of small, medium, or large size
-
3.
The perforation should be dry for at least 4 weeks.
-
4.
The air-bone gap is matching the size of the perforation.
-
5.
ABG of ≤ 30 dB
Exclusion criteria
-
1.
The age of the patient is below 15 or above 60.
-
2.
Total and marginal perforation
-
3.
The perforation is wet or dry for less than 4 weeks.
-
4.
The presence of otitis externa or otomycosis.
-
5.
Patients who were unfit for surgery
-
6.
Patients with suspected cholesteatoma
-
7.
Patients with history of previous ear surgery in the same ear
All patients signed a consent for conducting the study. All patients were subjected to a preoperative assessment protocol that included the following:
-
Full history taking of the ear condition with past history of medical or surgical treatment and history of any general medical conditions and special habits of medical importance
-
Examination of the ear using the otoscope and otoendoscope to confirm diagnosis of CSOM (safe type) and to detect size and site of drum perforation, ear discharge, condition of the middle ear, and exclude scars of previous operations. Tuning fork tests (Weber & Rinne) were performed. Other ear was examined and assessed.
-
Nasal and oral examination were carried out to exclude any other diseases or risk factor.
-
Preoperative audiological assessment including PTA and tympanometry
-
Routine preoperative laboratory investigations
The surgical procedure
-
1.
The surgical procedure was performed under general anesthesia.
-
2.
A total of 2.7-mm endoscope (0°) was used in all cases.
-
3.
The endoscope was introduced through transcanal route. Wax and debris, if present, were removed from external canal. Visualization and assessment of the perforation, ossicular chain, middle ear mucosa, and eustachian tube opening were performed.
-
4.
Trimming of the perforation edges using a needle and a forceps
-
5.
Round knife was used to curette the under surface of the drum.
-
6.
The perforation size was measured using a 2-mm Rosen round knife (Fig. 1)
-
7.
The size of perforation was classified into the following:
-
Small perforation: 1–3 mm
-
Medium-sized perforation: 3–5 mm
-
Large perforation : > 5 mm
-
8.
Harvesting the Tragal Cartilage Graft. The tragal cartilage was made 2 mm larger than estimated perforation size.
-
9.
Gel foam was placed in middle ear.
-
10.
Graft placement using a forceps, by the underlay technique through the perforation (Figs. 2, 3)

Measuring the perforation with Rosen round knife

The cartilage graft being placed to through the EAC

The cartilage graft sealing the tympanic membrane perforation
Postoperative care
Most patients were discharged on the same day and prescribed a systemic antibiotic and an analgesic. The patients were instructed to avoid any form of straining and avoid introducing water to the ear.
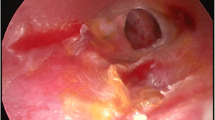
Examination of the ear using otoscopy or otoendoscopy was performed in the outpatient clinic on a weekly basis for 1 month and then every 2 weeks for up to 3 months to evaluate the graft uptake and to detect any infection (Fig. 4). Pure tone audiometry was performed 2 months postoperatively. Complete healing of the perforation of the drum, in addition to the improvement in the air-bone gap, was considered a success.

Endoscopic view of the cartilage graft 1 week postoperatively
The Statistical Package for Social Science (IBM SPSS) version 20 was utilized to analyze the data in our study. The comparison between two groups was done by using chi-square test, and/or Fisher exact test was used instead of chi-square test when the expected frequency was found less than 5. The p-value was considered significant as the following:
-
p > 0.05: nonsignificant
-
p < 0.05: significant
-
p < 0.01: highly significant
Results
This study included 20 patients. Fourteen patients (70%) were females, and 6 patients (30%) were males. Their age ranged from 17 to 53 years. As regards to size of perforation, 10 patients (10%) had small perforations, 7 patients (35%) had medium perforations, and 3 patients (15%) had large perforations. As regards to site of perforation, 11 patients (55%) had central perforations, 7 patients (35%) mainly anterior, and 2 patients (10%) mainly posterior perforations (Table 1).
Preoperative
Average air-bone gap (A-B gap) preoperative was 18.20 ± 7.78.
Postoperative
Average A-B gap 2 months postoperative was 7.75 ± 4.82 (Table 2).
Relation between size of perforation and success of graft take
In small size perforation, graft take was 100%, in medium size perforation, graft take 71.4%, and in large size perforation, graft take 66.7% (Table 3). Graft success rates were 85% with p-value 0.132.
In this study, the surgery was considered to be '”successful'” if there was complete healing of the tympanic membrane and improvement of hearing postoperatively (i.e., decrease in the A-B gap). Cases with residual perforation or no hearing improvement postoperatively were considered “failed.” Eighteen patients were considered successful, while 2 patients were considered failed.
Postoperative pain
In our study, 17 patients (85%) had no pain, and 3 patients (15%) had mild pain or discomfort (Fig. 5).

Postoperative pain
Discussion
The endoscopic “push-through” cartilage myringoplasty technique has many advantages: no postauricular incision, no tympanomeatal flap, no ear packing postoperatively, minimal or no pain, 1-day surgery, shorter operation time (20–35 min), and relative low costs.
The endoscope’s wide-field vision allows visualization of the entire perforation, and the undersurface of the tympanic membrane can also be assessed. This allows for repair of the perforation without any possibility of an iatrogenic cholesteatoma, unlike the conventional myringoplasty. Furthermore, endoscopic surgery gives better demonstration of the surgical steps, along with viewing of the anatomic structures in the same field, resulting in a better appreciation of their relationship [4].
In our study, the otoendoscope was utilized for inspection of medial surface of the tympanic membrane, as well as the status of ossicular chain. With the aid of the endoscope and curved instruments, removal of epithelial ingrowth from medal surface of tympanic membrane was feasible.
Endoscopic ear surgery is a one-handed technique. The rigid endoscope has to be held in the left hand having the right hand free to operate. This becomes a challenge when there is excessive bleeding. Many solutions can help to reduce the bleeding: preoperative local preparation, low and stable operative blood pressure, local adrenalin, and special instruments with suction [4].
In our series, bleeding presented as a challenge. It was due to contact of the endoscope and instruments with the canal wall. This was more evident in our first cases. Using only one hand for the surgery and suction prompted as a learning challenge. Maintaining a low stable operative blood pressure and low pulse rate helped reduce bleeding. Adrenaline-soaked cottonoids also helped stop bleeding in the operative field.
One other drawback of endoscopic myringoplasty is the difficulty to operate directly off the endoscope leading to neck strain and backache. Therefore, the camera and monitor were always used. This increased the weight of the endoscope, leading to arm fatigue.
Celik et al. in 2015 treated 32 patients with endoscopic push-through myringoplasty with graft success rate 87.5%, air-bone gap closure </=10 dB 91% [5].
El-Guindy et al. in 1992 underwent endoscopic transcanal myringoplasty on 36 patients with graft success rate 91.7%, air-bone gap closure </=10 dB 83.3% [6].
Ayache in 2013 reported an uptake rate of 96% in the 1-year follow-up period in 30 cases operated upon [3].
Huang et al. in 2016 had a success rate of 98% in 6 months follow-up period in fifty cases using endoscopic myringoplasty with cartilage graft. His study had a hearing improvement of 8.9 dB in the air-bone gap [7].
Mokbel et al. in 2015 had a graft uptake rate of 100% in type 1 cartilage tympanoplasty in forty ears with a follow-up period between 6 months and 1 year. He had a postoperative hearing improvement of the air-bone gap of 8.50 ± 1.25 dB [8].
Singh et al. in 2013 with an uptake rate of 92.85% in twenty-eight ears at 2 year follow-up. They had an average postoperative air-bone gap of 15.65 dB [9]. Özgür et al. in 2016, after 6-month follow-up, had a success rate of 92.5% in fifty-three ears with hearing improvement, with a postoperative air-bone gap of 10 ± 7 dB. All of our surgeries were performed by the endoscopic transcanal approach; none needed microscope, nor the postaural or the endaural approach [10].
Usami et al. in 2001, in their study, had twenty-two myringoplasty patients treated with endoscopy with a follow-up period of 1 year. The perforation closure rate was 81.8%, and improvement in air-bone gap after surgery was 14.8 dB [11].
Karhketo et al. in 2001 reviewed the data of twenty-nine endoscopic-assisted myringoplasty patients with a follow-up time of 1 year. The perforation closure rate was 80%, and improvement in air-bone gap after surgery was 7 dB [12].
Raj et al. in 2001 performed twenty endoscopic transcanal tympanoplasties had a closure rate of 90%, and the postoperative air-bone gap was < 10 dB in 60% of the ears [13].
In the present study, we achieved comparable results with a graft uptake rate of 85%. There was a statistically significant improvement in hearing outcome, with ABG gain of 7.75 ± 4.82.
Unlike the microscope, the endoscope can easily be transported and used in temporary ear surgery locations that take place in far less prepared places. Also, the endoscope costs less than the microscope, so it can be an efficient substitute in the healthcare facilities which cannot afford a microscope.
Drawbacks and limitations of this study
Incorporating the endoscope in ear surgery has a steep learning curve. One-handed technique poses as a challenge. External canal wall injury and bleeding could be troublesome. Availability of camera and monitor is mandatory to avoid back and arm fatigue. Operating on a larger scale for different tympanic membrane perforations regarding the size and site will give a better evaluation of the outcome using this technique.
Conclusion
The endoscope provides a wide and magnified field of vision, the ability to bypass bony overhangs or narrow areas in the external auditory canal with no need for repeated manipulations of the patient’s head. The main drawback of the endoscopic ear surgery is that it is a single-handed technique.
Endoscopic push-through technique of cartilage myringoplasty is an effective, minimally invasive, and feasible method with good success rate in terms of graft uptake as well as hearing improvement. It could be considered a first-choice approach for small- and medium-sized tympanic membrane perforations.
Availability of data and materials
Data are available from the authors upon reasonable request with permission from the Cairo University.
References
McKennan KX (1993) Endoscopic “second look” mastoidoscopy to rule out residual epitympanic/mastoid cholesteatoma. Laryngoscope. 103(7):810–814
Guy J, Muzaffar J, Coulson C (2020) Comparison of microscopic and endoscopic views in cadaveric ears. Eur Arch Otorhinolaryngol 277:1655–1658
Ayache S (2013) Cartilaginous myringoplasty: the endoscopic transcanal procedure. Eur Arch Otorhinolaryngol 270(3):853–860
Yadav SP, Aggarwal N, Julaha M, Goel A (2009) Endoscope-assisted myringoplasty. Singapore Med J. 50(5):510–512
Celik H et al (2015) Endoscopic cartilage push through myringoplasty 8(3):224–229
El-Guindy A (1992) Endoscopic transcanal myringoplasty. J Laryngol Otol 106:493Y5
Huang TY, Ho KY, Wang LF, Chien CY, Wang HM (2016) A comparative study of endoscopic and microscopic approach type, p 1
Mokbel KM, Moneir W, Elsisi H, Alsobky A (2015) Endoscopic transcanal cartilage myringoplasty for repair of subtotal tympanic membrane perforation: a method to avoid postauricular incision. J Otolaryngol Rhinol 1:1–4
Singh R, Kundu S, Sarkar S, Ghosh B, Mukhopadhyay S (2013) Comparative study of endoscopic temporalis fascia versus endoscopic cartilage tympanoplasty. Bengal J Otolaryngol Head Neck Surg 21:16–17
Özgür A, Dursun E, Terzi S, Erdivanlı ÖÇ, Coşkun ZÖ, Oğurlu M et al (2016) Endoscopic butterfly cartilage myringoplasty. Acta Otolaryngol. 136(2):144–148
Usami S, Iijima N, Fujita S, Takumi Y (2001) Endoscopic-assisted myringoplasty. ORL J Otorhinolaryngol Relat 63:287Y90
Karhuketo TS, Ilomaki JH, Puhakka HJ (2001) Tympanoscope-assisted myringoplasty. ORL J Otorhinolaryngol Relat. 63(6):353–357
Raj A, Meher R (2001) Endoscopic transcanal myringoplasty: a study. Indian J Otolaryngol Head Neck Surg. 53(1):47–49
Acknowledgements
Not applicable
Funding
None
Author information
Authors and Affiliations
Contributions
The authors read and approved the final manuscript. FG (corresponding author), writing the article and did surgeries. UN, revision and adjustment of research; AE, collection of data and preparing patients. TA, did surgeries, revision of data, and adjustment of research
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted in the Cairo University Hospital after receiving the approval from the Research Ethics Committee, reference number 18804R. Written informed consents were obtained from all participants.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gharib, F.M., Naseer, U.A., Elessi, A.M.J. et al. Endoscopic permeatal “push-through” myringoplasty: hearing gain and graft uptake. Egypt J Otolaryngol 38, 121 (2022). https://doi.org/10.1186/s43163-022-00283-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-022-00283-1