
Abstract
Background
Rheumatoid arthritis (RA) is an autoimmune disease in which the immune system attacks the tissues of the joints by mistake. Different factors—either genetic or environmental—affect the development of the RA disease in patients. A lot of studies aimed to examine the genetic associations with this disease in different populations. This research aspires to perform a genetic association study between six single-nucleotide polymorphisms (SNPs) and RA disease in the Egyptian population with 49 controls and 52 patients. The SNPs that are included in this study are MIR146A rs2910164 (C:G), MIR499/MIR499A rs3746444 (T:C), MTMR3 rs12537(C:T), MIR155HG rs767649 (A:T), IRAK1 rs3027898 (A:C) and PADI4 rs1748033 (C:T).
Methods
Real-time PCR with TaqMan allelic discrimination assay were both used to perform the genotyping. The Odds ratio models with 95% confidence interval were used to test the associations. The used models are multiplicative, recessive, dominant and co-dominant.
Result
The demonstrated results indicated that rs2910164 and rs12537 were associated with RA, while rs3746444 showed no association in all the tested models. The remaining SNPs were excluded as they didn't pass the Hardy–Weinberg equilibrium test.
Conclusion
The MIR146A and MTMR3 polymorphisms showed susceptibility to RA. Moreover, MIR499/MIR499A had no role in the disease.
Key points
-
1.
MIR146A (C allele) had a protective role in rheumatoid arthritis association. MTMR3 was associated with rheumatoid arthritis using the dominant, Co-dominant heterozygote and recessive models. MIR499/MIR499A had no association with rheumatoid arthritis.
Similar content being viewed by others

Background
Rheumatoid arthritis (RA) is a chronic inflammatory disorder, it mostly affects the joints, but it can also reach and affect other organ systems such as skin and the lungs as well. RA is an autoimmune process that is typically triggered by an interaction between a genetic factor and an environmental factor. A person, with a certain gene for an immune protein—like human leukocyte antigen or HLA-DR1 and HLA-DR4, might develop RA [1] after getting exposed to an environmental factor like cigarette smoke or a specific pathogen. RA is known to occur with higher chances in females rather than males with a 3:1 chance. The average age in females for the disease to appear is in the 30 s and 40 s wherein males it is discovered further delayed than females [2].
This work aims to observe the genetic association between six different single-nucleotide polymorphisms (SNPs) and the RA disease. The study applied four statistical genetic models for measuring the association between the SNPs and the disease, which are multiplicative, dominant, recessive and co-dominant. Each model works on a different exposed group and unexposed group in cases and controls, where the data represented in two by two contingency table. The multiplicative model works on the alleles level. The dominant model compares major allele homozygote versus heterozygote and minor allele homozygote, while the recessive compares major allele homozygote and heterozygote versus minor allele homozygote. The co-dominant model compares the major homozygote versus minor allele homozygote or the heterozygote.
Some studies found that micro-ribonucleic acid (miRNA) changes T cell selection and receptor sensitivity [3, 4]; accordingly, miRNA may be associated with autoimmune diseases; also there are studies showed that miRNAs play a role in the progress of RA [5, 6].
This study worked on examining 6 SNPs that are located within six different genes and on different chromosomes. SNP rs2910164 is located on the microRNA146a (MIR146A) gene and on chromosome 5. SNP rs3746444 is located between two genes that are microRNA 499 (MIR499) and microRNA 499a (MIR499A); mir-499 can affect the production of C-reactive protein (CRP) and inflammation in RA [7]. This SNP is located on chromosome 20. The rs12537 is located on myotubularin related protein 3 (MTMR3) and chromosome 22. SNP rs767649 is located on MIR155 host gene (MIR155HG) and on chromosome 21. SNP rs3027898 is located on interleukin 1 receptor-associated kinase 1 (IRAK1) and belongs to the X chromosome. And finally, SNP rs1748033 is located on peptidyl arginine deiminase type 4 (PADI4) that is located on chromosome 1. (PADI4) gene encodes PADI4 enzyme; PADI4 enzyme produces autoantigen citrullinated peptides recognized by anti-cyclic citrullinated peptide (anti-CCP) [8] that increases the risk of being diagnosed of RA disease.
Many studies included these SNPS to explore the linkage between them and rheumatoid arthritis disease such as rs767649 [9], rs2910164 [10,11,12], rs3746444 [7, 10], rs12537 [13], rs3027898 [14, 15], rs1748033 [16], and this research is following the footsteps of these by studying these SNPS as well.
Methods
Molecular genetic methods
DNA was extracted from whole blood using Qia-amplification DNA extraction kit (Qiagen, USA). 200 ul EDTA whole blood was used for extraction of DNA by DNA extraction kit according to the protocol provided with the kit. The extracted DNA samples were subjected to DNA quantitation and purity assessment using the NanoDrop® (ND)-1000 spectrophotometer (NanoDrop Technologies, Inc. Wilmington, USA). Genotyping was performed using real-time PCR with TaqMan allelic discrimination assay (Applied Biosystems, USA). The DNA used is (100 μg); this study is consistent with the declaration of Helsinki. Each participant gave a written consent before experiment. A predesigned primer/probe set for the two genotypes was used (Applied Biosystems, USA). Probes were synthesized with reporter dye FAM or VIC covalently linked at the 5/end and a quencher dye MGB linked to the 3/end of the probe (Applied Biosystems, USA) (rs2910164 (C/G), rs3746444 (T/C), rs12537(C/T), rs767649 (A/T), rs3027898 (A/C) and rs1748033 (C/T)). Real-time PCR was performed using a Rotor gene Q Real-Time PCR System (Qiagen, Valencia, CA, USA) with the following conditions: after a denaturation time of 10 min at 95 °C, 45 cycles at 92 °C for 15 s then 60 °C for 90 s for annealing and extension were carried out and fluorescence was measured at the end of every cycle and at the endpoint.
Statistical methods
The Chi-square test (χ2-test) was used to analyze genotype and allele distributions of cases and controls. Odds ratio (OR) and 95% confidence interval (95% CI) were calculated as well. Hardy–Weinberg equilibrium (HWE) test was applied on the controls. If the HWE p value was less than 0.001 [17, 18], this indicates a deviation in the population from HWE and the corresponding SNP was excluded from the study. The ratio of the males versus females between the cases and controls was analyzed by proportion test using STATA software, and it showed that the ratio is not statistically significant as the p value was equals to 0.068 which passes the defined 0.05 threshold.
The Chi-square test is a formal statistical test used to analyze categorical data to verify the statistical significance of the results. Generally, the lower the χ2 value, the greater the likelihood that there is no significant difference between cases and controls. To be sure that the Chi-square result gives a real statistically significant difference, the p value should be looked up. A low p value indicates a low expectation of finding these results by coincidence, while a high p value means a high probability of finding these results by chance.
In case of p value of 1, it means that the two groups were not different at all. Odds ratio is one of the most popular measures of the strength of association between a disease severity and a biomarker SNP. OR is used to determine the probability of disease severity presence versus the disease severity absence in exposed and unexposed individuals.
Confidence interval (CI) is a formula that shows how to use a sample data to calculate an interval that estimates a point estimate (OR). A large CI marks a low level of precision of the OR, while a narrower CI indicates a reliable OR. When the two values of CI are less than 1, this indicates a protective association. When the two values of CI are greater than 1, this indicates a susceptible association.
The used equations for calculating OR, CI, and Chi-square test are as follows:
For the allelic odds ratio:
where m11 and m21 indicate allele a in cases and controls, respectively, and m12 and m22 refer to allele A in cases and controls, and the equation is to calculate the OR for allele A.
The following formulas are used for a 95% confidence interval (CI):
Chi-square test formula:
where Oi represents the observed frequency and Ei represents the expected frequency.
Study population
RA patients were diagnosed by physician investigators and followed the 1987 American College of Rheumatology (ACR) criteria. DAS28 (Disease Activity Score in 28 Joints), which is a validated score for established RA, was used as a measure for disease activity.
The observed controls had no signs of RA, including morning joint stiffness, citrulline antibody, positive rheumatoid factor (RF), or the findings of rheumatoid nodules. Furthermore, the patients with other inflammatory disorders or autoimmune diseases unrelated to RA were not included.
Subjects
The study consists of 52 RA patients, 85% of them are females, and 49 controls that 67% of whom are females. In cases, the mean age of females’ ± standard deviation (SD) was 40 ± 9.6 years. The mean age of males was 37 ± 16.64 years. In the controls, the mean age of females was 40 ± 9.92 years, while the mean age of males was 37.2 ± 10.7 years. The average disease duration of RA in females was 6.63 ± 4.29 years, while the duration of RA in males was 9.06 ± 8.25.
The study was approved by the Ethical Committee of Faculty of Medicine, Cairo University, and an oral and written informed consent was obtained from all participants.
Results
In this study, HWE, minor allele frequency (MAF), and the percentage of individual genotyped for each SNP have been conducted. The minimum accepted genotype percentage was 80%. The markers that were significantly deviated from HWE, where the HWE p value was less than 0.001, were excluded.
The minimum MAF accepted is at 0.05. Table 1 showcases the results of the marker checks. All the SNPs for all individuals were fully genotyped, and just three SNPs passed the marker checks. Table 1 also provides ID, physical position, chromosome number, major allele, and minor allele for each SNP. From Table 1, it can be observed that rs2910164, rs3746444, and rs12537 passed all the marker checks, and accordingly, they are included in the association study. The other excluded SNPs’ results are shown as reference for future studies.
Table 2 presents the association between the SNPs that passed HWE test and the RA disease; the highlighted cells with the green color present the RA protective association of the examined SNPs, while the purple color indicates the susceptible association of the SNPs to the RA.
Figure 1 shows a graphical representation of the association results for the included SNPs, while Fig. 2 demonstrates the genotype distribution in RA cases and controls. It is deduced from Table 2 and Fig. 2 that both MIR146A and MTMR3 are significantly associated with RA, while MIR499, MIR499A showed no associativity with the disease. As for the excluded SNPs MIR155HG, IRAK1, and PADI4, Figs. 3 and 4 represent the genotype distribution between patients and control groups and the association analysis, respectively. Table 3 demonstrates the excluded SNPs analysis with different models, with same color scheme meaning used in Table 2.

Association analysis for examined SNPs with RA disease. The horizontal line in each model represents the significance level of the p value (0.05). a Multiplicative model, b dominant model, c recessive model, d co-dominant with heterozygote model, e co-dominant with minor homozygote model

Genotype distribution in RA cases and controls for the included SNPs

Genotype distribution in RA cases and controls for the excluded SNPs

Association analysis for the excluded SNPs. The horizontal line in each model represents the significance level of the p value (0.050). a Multiplicative model, b dominant model, c recessive model, d co-dominant with heterozygote model, e co-dominant with minor homozygote model
Figure 1 shows the associativity of each studied SNP with RA according to all models (multiplicative, dominant, recessive, co-dominant).
As for the excluded SNPs, MIR155HG had a protective association in the recessive and co-dominant minor models, while the SNP IRAK1 had a susceptible association in the dominant and the co-dominant heterozygote, and protective association in the recessive model. Finally, PADI4 had only a susceptible association in the dominant model.
Discussion
This study examined the association with the RA susceptibility in the Egyptian population with 52 cases and 49 controls. There are six SNPs that had been investigated with their distribution of genotypes and alleles.
As shown in Table 2 and Fig. 2, MTMR3 and MIR146A are associated with RA. Firstly, for MIR146A rs2910164 (C:G), the major allele C is protective in the multiplicative model, wherein the dominant model the major homozygote (CC) is also protectively associated. Both co-dominant models, heterozygote and minor homozygote, also verify the protective association. The recessive model, however, didn’t indicate any association. As for MIR499, MIR499A rs3746444 (T:C), the results presented no association with RA in any of the tested models.
Furthermore, MTMR3 rs12537 (C:T) indicates no association with RA in both the multiplicative and co-dominant minor homozygote; however, the major homozygote is susceptible in both the dominant and co-dominant heterozygote models while the recessive model indicated that the minor homozygote is susceptible. At the same time, [13] concluded that rs12537TT was positively associated with disease severity in RA. They identify a novel role of rs12537 in the susceptibility and progression of RA through increased autophagy.
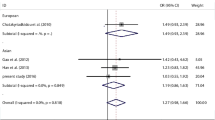
Table 4 demonstrates a summary of previous studies along with this study of the 6 genes included and their associations with RA. This study shows a protective association to RA on MIR146A; on the other hand, other studies showed no association to RA. The other studies were conducted on Greek, Iranian, Polish, Asian, Chinese, and Egyptian populations; they all concluded that there is no association with the disease [24]. This variation might be a result of the difference in sample sizes between the studied populations as shown in Table 4, while both this study and the one in [23] studied Egyptian population. This study included both genders males and females while [23] included females only.
[30] concluded that miRNA-146a (rs2710164) was significantly associated with RA susceptibility. The C allele of miRNA-146a (rs2710164) can be considered to be protective.
As for MIR499, MIR499A [26, 27], these studies were applied on two different Chinese population, and their conclusion was that there is no association with the disease. In a further study on the same SNP rs3746444 conducted on Han Chinese [22], there was no association when tested; however, the finding indicated that CT genotype increases the level of anti-CCP antibody which increases the risk of RA. Other studies showed a variation in associations; for example, in [21] Zhou et. al. studied Caucasian and Asian populations. Their conclusion was that the gene is susceptible in Caucasian, while there was no association in the Asian population. The gene was susceptible to RA in an Egyptian population study [7]. Another study of the Egyptian population, but limited to females only, indicated the association of the gene with RA [23].
miRNA-146a (rs2710164) polymorphism, the GG genotype was significantly higher in RA patients compared to the control subjects and the frequency of the G allele of the miRNA-146a (rs2910164) polymorphism was significantly higher in the RA patients than in the control subjects. The C allele of miRNA-146a (rs2710164) can be considered to be protective, as patients with the CC genotype had decreased deformity frequency and DD [30].
Additionally, [13] results suggest that rs12537 could increase the risk and progression of RA by reducing MTMR3 levels leading to increased autophagy level.
This study has some limitations, including the small sample size and the number of SNPS. The study could be applied on more patients or another bigger population for verification.
Conclusion
In summary, this study examined six SNPs in the Egyptian population; three of them were included in the association study, the rest were excluded on an HWE basis, but its results are shown for references. The MIR146A and MTMR3 polymorphisms showed association with RA. However, it has been demonstrated that MIR499/MIR499A has no role in the disease. Further work needs to be done on a larger sample size on the Egyptian population to confirm the results.
Availability of data and materials
The data used during the current study are not publicly available due to subject confidential agreement but are available from the corresponding author on reasonable request.
References
Kampstra ASB, Toes REM (2017) HLA class II and rheumatoid arthritis: the bumpy road of revelation. Immunogenetics. https://doi.org/10.1007/s00251-017-0987-5
Freeman J (2018) RA facts: What are the latest statistics on rheumatoid arthritis? Rheum Arthritis Support Network. https://www.mendeley.com/guides/web-citation-guide. Accessed 13 May 2019
Li QJ, Chau J, Ebert PJR, Sylvester G, Min H, Liu G et al (2007) miR-181a is an intrinsic modulator of T cell sensitivity and selection. Cell. https://doi.org/10.1016/j.cell.2007.03.008
Cobb BS, Hertweck A, Smith J, O’Connor E, Graf D, Cook T et al (2006) A role for Dicer in immune regulation. J Exp Med. https://doi.org/10.1084/jem.20061692
Sonkoly E, Ståhle M, Pivarcsi A (2008) MicroRNAs: novel regulators in skin inflammation. Clin Exp Dermatol. https://doi.org/10.1111/j.1365-2230.2008.02804.x
Roy S, Sen CK (2010) MiRNA in innate immune responses: novel players in wound inflammation. Physiol Genomics. https://doi.org/10.1152/physiolgenomics.00160.2010
Fattah SA, Ghattas MH, Saleh SM, Abo-Elmatty DM (2018) Pre-micro RNA-499 gene polymorphism rs3746444 T/C is associated with susceptibility to rheumatoid arthritis in Egyptian population. Indian J Clin Biochem. https://doi.org/10.1007/s12291-017-0652-7
Schellekens GA, Visser H, De Jong BAW, Van Den Hoogen FHJ, Hazes JMW, Breedveld FC et al (2000) The diagnostic properties of rheumatoid arthritis antibodies recognizing a cyclic citrullinated peptide. Arthritis Rheum. https://doi.org/10.1002/1529-0131(200001)43:1%3c155::AID-ANR20%3e3.0.CO;2-3
Shaker OG, Abdelaleem OO, Fouad NA, Ali AMEA, Ahmed TI, Ibrahem EG et al (2019) Association between miR-155, Its polymorphism and ischemia-modified albumin in patients with rheumatoid arthritis. J Interf Cytokine Res 39:428–437. https://doi.org/10.1089/jir.2019.0001
Ahmadi K, Soleimani A, Soleimani Motlagh S, Ahmadi SB, Almasian M, Kiani AA (2020) Polymorphisms of pre-miR-499 rs3746444 T/C and Pre-miR-146a rs2910164 C/G in the autoimmune diseases of rheumatoid arthritis and systemic lupus erythematosus in the West of Iran, vol 49
Hu Q, Li B, She R, Wu X, Tan J, Hu JTQ (2019) Association of polymorphisms of miR-146a rs2910164 locus with clinical features of rheumatoid arthritis. Chinese J Med Genet 36:505–507
Bagheri-Hosseinabadi Z, Mirzaei MR, Hajizadeh MR, Asadi F, Rezaeian M, Abbasifard M (2021) Plasma MicroRNAs (miR-146a, miR-103a, and miR-155) as potential biomarkers for rheumatoid arthritis (RA) and disease activity in iranian patients. Mediterr J Rheumatol 32:324–30
Senousy MA, Helmy HS, Fathy N, Shaker OG, Ayeldeen GM Association of MTMR3 rs12537 at miR-181a binding site with rheumatoid arthritis and systemic lupus erythematosus risk in Egyptian patients. https://doi.org/10.1038/s41598-019-48770-5
Zhao P, Li Q, Liang R, He X (2020) Interleukin-1 receptor-associated kinase gene polymorphisms contribute to rheumatoid arthritis risk: a meta-analysis. https://doi.org/10.1111/1756-185X.13946
Gamil Shaker O, Ahmed N, Boghdady EL, El-Dessouki A, Sayed E (2018) Cellular physiology and biochemistry cellular physiology and biochemistry original paper association of MiRNA-146a, MiRNA-499, IRAK1 and PADI4 polymorphisms with rheumatoid arthritis in Egyptian population. Cell Physiol Biochem 46:2239–2249. https://doi.org/10.1159/000489592
Hashemi M, Zakeri Z, Taheri H, Bahari G, Taheri M (2015) Association between peptidylarginine deiminase type 4 rs1748033 polymorphism and susceptibility to rheumatoid arthritis in Zahedan, Southeast Iran. Iran J Allergy Asthma Immunol 6:66
Fox CS, Heard-Costa N, Cupples LA, Dupuis J, Vasan RS, Atwood LD (2007) Genome-wide association to body mass index and waist circumference: the Framingham Heart Study 100K project. https://doi.org/10.1186/1471-2350-8-S1-S18
Abdelaleem EA, Zaghlol HM, Abdelshafy S, Mohamed RA (2018) Tumour necrosis factor gene polymorphisms in Egyptian patients with rheumatoid arthritis and their relation to disease activity and severity. Centr Eur J Immunol 44:277–284. https://doi.org/10.5114/ceji.2019.89602
Hashemi M, Eskandari-Nasab E, Zakeri Z, Atabaki M, Bahari G, Jahantigh M et al (2013) Association of pre-miRNA-146a rs2910164 and pre miRNA-499 rs3746444 polymorphisms and susceptibility to rheumatoid arthritis. Mol Med Rep. https://doi.org/10.3892/mmr.2012.1176
Bogunia-Kubik K, Wysoczańska B, Piątek D, Iwaszko M, Ciechomska M, Świerkot J (2016) Significance of polymorphism and expression of miR-146a and NFkB1 genetic variants in patients with rheumatoid arthritis. Arch Immunol Ther Exp. https://doi.org/10.1007/s00005-016-0443-5
Zhou M, Jiang B, Xiong M, Zhu X (2018) An updated meta-analysis of the associations between microrna polymorphisms and susceptibility to rheumatoid arthritis. Front Physiol. https://doi.org/10.3389/fphys.2018.01604
Yang B, Zhang JL, Shi YY, Li DD, Chen J, Huang ZC et al (2011) Association study of single nucleotide polymorphisms in premiRNA and rheumatoid arthritis in a Han Chinese population. Mol Biol Rep. https://doi.org/10.1007/s11033-010-0633-x
El-Shal AS, Aly NM, Galil SMA, Moustafa MA, Kandel WA (2013) Association of microRNAs genes polymorphisms with rheumatoid arthritis in Egyptian female patients. Jt Bone Spine. https://doi.org/10.1016/j.jbspin.2013.03.005
Chatzikyriakidou A, Voulgari PV, Georgiou I, Drosos AA (2010) A polymorphism in the 3’-UTR of interleukin-1 receptor-associated kinase (IRAK1), a target gene of miR-146a, is associated with rheumatoid arthritis susceptibility. Jt Bone Spine. https://doi.org/10.1016/j.jbspin.2010.05.013
Zhou X, Zhu J, Zhang H, Zhou G, Huang Y, Liu R (2015) Is the microRNA-146a (rs2910164) polymorphism associated with rheumatoid arthritis? Association of microRNA-146a (rs2910164) polymorphism and rheumatoid arthritis could depend on gender. Jt Bone Spine. https://doi.org/10.1016/j.jbspin.2014.12.009
Zhang H, Pu J, Wang X, Shen L, Zhao G, Zhuang C et al (2013) IRAK1 rs3027898 C/A polymorphism is associated with risk of rheumatoid arthritis. Rheumatol Int. https://doi.org/10.1007/s00296-012-2379-3
Yang X-K, Li P, Zhang C, Leng R-X, Li S, Liu J et al (2017) Association between IRAK1 rs3027898 and miRNA-499 rs3746444 polymorphisms and rheumatoid arthritisAssoziation zwischen Polymorphismen von IRAK1 rs3027898 und miRNA-499 rs3746444 und rheumatoider Arthritis. Z Rheumatol. https://doi.org/10.1007/s00393-016-0169-0
Abdul-Maksoud RS, Sediq AM, Kattaia AAA, Elsayed WSH, Ezzeldin N, Abdel Galil SM et al (2017) Serum miR-210 and miR-155 expression levels as novel biomarkers for rheumatoid arthritis diagnosis. Br J Biomed Sci. https://doi.org/10.1080/09674845.2017.1343545
Atabaki M, Hashemi M, Daneshvar H, Alijani E (2017) Association between interleukin-1 receptor associated kinase 1 rs3027898 A/C gene polymorphism and rheumatoid arthritis. Biomed Rep. https://doi.org/10.3892/br.2017.855
Ayeldeen G, Nassar Y, Ahmed H, Shaker O, Gheita T (2018) Possible use of miRNAs-146a and -499 expression and their polymorphisms as diagnostic markers for rheumatoid arthritis. Mol Cell Biochem 449:145–156. https://doi.org/10.1007/S11010-018-3351-7
Acknowledgements
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
The first two authors contributed equally to this work. The third and fourth authors helped in supervising, revising, and reviewing work results. The fifth author provided the needed data to carry on the research. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethical Committee of Faculty of Medicine, Cairo University, and an oral and written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ibrahim, A.M., Hassan, N.M., Saad, M.N. et al. A genetic study of the association of six polymorphisms with rheumatoid arthritis in the Egyptian population. Egypt J Med Hum Genet 23, 132 (2022). https://doi.org/10.1186/s43042-022-00343-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43042-022-00343-4