
Abstract
Background
Saudi Arabia is one of the countries seriously affected by coronavirus disease 2019 (COVID-19) worldwide. With a few cases in early March, the daily spread of this disease increased to nearly 5000 at one point in time during the first wave to mid-June 2020. With committed efforts and public health interventions, it has been controlled to nearly 1000 by the end of August 2020 and less than 217 by November 28, 2020; thereafter, reporting declines and small increases. However, by December 2021, a third wave started, lasting for 2 months, during which the infection rate increased rapidly. By April 1, 2022, the number of infected persons in the country was 750,998, with 9047 deaths, 7131 active, and approximately 400 critical cases. This analysis of COVID-19 statistics of the Ministry of Health of Saudi Arabia (March 2020–April 2022) is carried out along with population data to extract patient proportions per 100,000 persons to illustrate the hypothesized social and community impact, which influences families and households.
Results
The results showed a high rate of infection and mortality, but with recovery. These rates varied across localities and cities. A few cities with higher population densities are less affected by the spread of the epidemic. However, few localities and upcoming cities/townships were severely affected. These effects are explained as the percentage of the population affected, which exposes the impact on societies, families, and individual members. With concerted efforts, they are brought under control through recovery and adopting mitigation methods.
Conclusions
Localities could be classified into four categories based on the proportion of the infected population: rapidly increasing, moderately increasing, declining, and stabilizing. Moreover, differential proportions of the affected population have implications at social and familial levels. Analysis and understanding of these trends, considering the base population, are important for policy building and intervention strategies accounting for grassroots-level demographics, which might serve as a tool to enhance interventions at population and family levels. Strategies for awareness creation and compassionate care are essential to address the psychosocial impact of health emergencies, as proved by the Ministry of Health, Saudi Arabia.
Similar content being viewed by others


Background
The outbreak of coronavirus disease 2019 (COVID-19), as stated by Zhou et al. (2020), created tensions even within well-knit family units, especially in poor infrastructure conditions and crowded living arrangements. Such tensions changed family and social life, restricting interpersonal contacts and affective gestures within the small circle of people, as well as strict disciplined precautions of social distancing, protection of face masks, and no handshakes (Iqbal et al. 2020). This led to containment, quarantine, lockdowns, and curfews (Zhou et al. 2020). Such isolations implemented to curb disease spread paved the way for conflicts, tensions, and violence: physical, psychological, and financial (Usher et al. 2020). In contrast, COVID-19 manifests differently among family members depending upon contact: some are infected but not others because of different immune responses (Sun et al. 2020).
As a result, there have been enormous changes and unparalleled consequences in the society and families, including financial, resulting in a demand for government support (Hitchings and Maclean 2020; Michels et al. 2020). Therefore, social distancing, isolation, quarantine, and lockdown strategies for epidemic transmission control management are central to the public health strategy toward mitigation and containment, which in turn influences social and family dynamics and economics (Usher et al. 2020; Humphreys et al. 2020; Motlhatlhedi et al. 2020).
In Saudi Arabia, the pandemic spread was addressed in the Riyadh declaration on digital health formulated in August 2020 to create the infrastructure necessary for effective evidence-based practices and high-quality real-time data aimed at providing actionable information to more health systems and countries (Al-Knawy et al. 2020). Although attempts to address COVID-19 spread have been assessed and investigated from a medical perspective in addition to the daily data release from the Ministry of Health, assessments of economic, social, and community impacts have not been carried out, especially at the social and family levels (Almaghlouth et al. 2020). However, there are few analyses indirectly exposing the family to this issue. For example, a study of oncology management experience during the epidemic explains the use of national and international guidelines to minimize infection risk and subsequent complications mentioning the risk of infection from healthcare staff to other family members (Ibrahim et al. 2020). Another study revealed moderate to severe psychological impact in one-fourth of the general population (Alkhamees et al. 2020), whereas another study explained the negative psychological effect of COVID-19 on physicians (Al-Sulais et al. 2020). Barry et al. (2020a) narrated the spread of Middle East respiratory syndrome coronavirus (MERS-CoV2; COVID-19) in the Kingdom. In addition, Barry et al. (2020b) and Salam et al. (2022) explained the case fatality rate, transmission exacerbating factors, and awareness of disease spread as a result of the Kingdom’s swift community action and hospital preparedness toward mitigation. All these studies have highlighted the importance of population, society, and family in addressing the disease. Still, many more investigations are necessary to succeed in such emergency situations, especially the demographic and public health analyses bringing out various aspects of population -, society, family, and individuals. More than small local-level survey-based research, national-level data analysis and macro-level interpretations are needed to enlighten policies and intervention strategies in the country. Here, we explain the national scenario by considering population size as denominator.
This consolidation was conducted to discuss the proportion of the population affected by COVID-19 and its probable influence on societal and family dynamics. This study has been carried out with the hypothesis that a large part of the statistics is misunderstood and misleading, without exposing the denominator, the population at risk, which shows the disease load and burden at the society, community, and family levels. There are countries with a population of a few million to a hundred million, or even a billion. The number of infected persons is treated as a percentage of the total population, which provides scope for understanding the number of infected persons per family. Although data availability at the national level by demographic, social, or economic characteristics raises concerns, this analysis is important.
Methods
This analysis is based solely on the daily status reports of the Ministry of Health, Saudi Arabia, from its beginning on March 21, 2020 to April 1, 2022, giving the number of infections recorded at various localities. Calculations are performed with these data based on total population size, at the national level, accessed online (worldometers, populationstats, and worldpopulationreview), at various points during 2021 and 2022. Adopting population size (35,257,261 on April 28; 35,301,732 on May 28; 35,349,168 on June 28; 35,393,638 on July 28; 35,439,591 on August 28; 35,484,062 on September 28; 35,575,968 on November 28; 35,626,369 on December 28, 2021; 35,712,345 on February 28; and 35,753,851 on March 28, 2022, cited on www.worldometers.info) for each month, as the denominator, the following indicators are calculated for the country as a whole:
-
Daily reported cases per 100,000 population
-
Total cases and total recoveries per 100,000 population
-
Total deaths per 100,000 population
-
Critical cases per 100,000 population
-
Active cases per 100,000 population
Calculations are performed to show the affected locations and the 100,000 population. In addition, they were presented in a graph and divided into four groups. Such analyses were performed to quantitatively explore the effect. Furthermore, with the available information on the number of cases in various localities and their corresponding population data gathered from the above-mentioned sources, their rates per 100,000 population were calculated, tabulated, and discussed. This is a proxy for the number of persons affected by the family. On the other hand, it explains the seriousness or threat to society. All these available statistics could lead to a situation analysis; the non-availability of further breakups limits the scope to a large extent. However, this preliminary analysis gives a lead, input, and indication for further analysis and extensions.
Results
Results of analyses are given below under two heads.
Epidemic infection as proportion of population
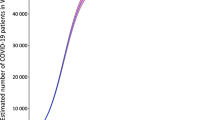
There are a total of 750,998 infected cases, as of April 1, 2022 (2100 per 100,000 persons), with higher infection rates, but almost all recovered (734,820; 2055 per 100,000 persons), while the rest either passed away (9047; 25 per 100,000 persons) or were under treatment (7131; 20 per 100,000 persons). Thus, there is a narrow gap between infected and recovered persons, especially in the first two waves but different in the third wave. However, they are bridged at a faster pace, as shown in Fig. 1. It is the mortality from COVID-19 which has received greater concern in the country due to its ups and downs.

Spread of COVID-19, recoveries and fatality per 100,000 persons
This higher cause-specific mortality creates a large burden on the public health system. However, daily reports of cases also show reductions in infections and mortality coupled with intermittent increases in infections and case fatality. With healthcare interventions, there were reductions in cases and mortality, showing firm commitments and accountability, which could be modeled to regain family solidarity in epidemic-prone situations, especially the healthy mix of awareness creation and compassionate care.
While applying the total population as the denominator, daily infection of COVID-19, as plotted, reached its peak point of 14 per 100,000 persons on June 17, 2020, corresponding to the highest number of infections of 4919 in the country, reported on a particular day. On the same day, the total number of cases was 401 per 100,000 people. With strenuous efforts and health interventions, these rates have steadily reduced. It is to be noted that the highest recovery of 7718 (22 per 100,000 persons) was recorded on July 14, 2020. However, the number of daily infections per 100,000 persons from its highest mark declined sharply to 1 on February 28, which increased to 3 on April 30, 2021. While the daily cases declined to none per 100,000 persons on January 3, 2021, and increased thereafter. Similarly, total cases declined in 2021 to 1030 on January 3, 1070 on February 28, and 1184 on April 30 per 100,000 persons; total recoveries were 1005, 1044, and 1136; and total deaths were 18, 18, and 20 per 100,000 persons, respectively. From December 2021–January 2022, the third wave and daily infections reached a height of 5928 on January 19 (17 per 100,000 persons with a recovery of 14 per 100,000 persons).
Major localities including future cities
Saudi Arabia is divided into 13 administrative areas and 118 governorates. Reports of COVID-19 considered a mixed geographical pattern of 213 affected localities in the country. Certain localities with higher infection per household were identified from the data. The top 30 localities in each time period, including other future cities at various months, gave rise to a total of 48 localities. These localities vary in terms of population size; thus, this analysis across the number of affected persons per 100,000 persons was carried out using population size as of 2021, cited in the above-mentioned online sources (Table 1). Major localities, such as big cities, are seriously affected by the epidemic but are less intense when considering the density of infection on the specified parameters. For example, the largest city, the capital city of Riyadh, had the highest number of affected persons (58,589) until November 28, accounting for 1393 per 100,000 persons. Attention should be paid to neighborhoods such as Hofuf (6781), Dammam (2544), Dhahran (4373), Jazan (3255), Baish (2868), Bishah (1882), and Safwa (3616) for their higher number of affected persons per 100,000 persons. These are comparatively higher than those of other larger cities, such as Jeddah, Makkah, and Madinah.
This section has data available only up to November 28, 2020, where these localities are observed to fall under four categories based on the proportion of the affected population such as (a) rapidly increasing, (b) reasonably increasing, (c) slowly decreasing, and (d) stabilizing to a low level. The first group, which rapidly increases, includes five future cities, Madina, Buraydah, Hail, Arar, and Jazan, and 12 other localities, Khamis Mushait, Dhahran, Yanbu, Unaiza, AlZelfi, Wadi Ad Dawasir, Khulais, Bqeeq, Al-Khafji, Al-Nairiya, Al Dawadmi, and Al Majmaa. As a result, these localities rapidly increased on a daily basis (Fig. 2). The second group comprised of eight localities: five future cities of Riyadh, Makkah, Najran, Sakaka, and Abha, and three other neighborhoods of Raz Tanura, Mahayel Asir, and Al-Muzahmiah. The third category comprises ten localities: three future cities of Jeddah, Dammam, and Qatif, and seven other localities of Al Jubail, Al-Mubarass, Samta, Qunfudah, Ahad Al Rufaidah, Ar Raz, and Hofuf. The last category had 14 localities: four future cities of Taif, Al Ahsa, Tabouk, and Al Baha, and ten other localities of Bishah, Ad Diriyah, Saihat, Al Hada, Khobar, Baish, Hafar Al Batin, Safwa, Abu Arish, and Al Kharj.

Neighborhoods classified according to the infection spread per 100,000 persons
Although these data have not been updated, it is assumed that the trend continued, keeping in mind the mass control programs executed in major administrative areas, locations, and cities. In addition, overcrowded and densely populated urban pockets are equipped with resources of manpower and materials to address epidemics than the less populated, rapidly developing urban pockets. Such trends have implications for individuals, families, communities, and societies in controlling infections, particularly in protecting people from the threat of epidemics.
Discussions
The daily reported cases in the country increased since its inception in early March 2020, reaching its peak in July 2020 and declining thereafter, but with a less threatening second wave and a more threatening third wave. As pointed out by Stokes and Patterson (2020), population size and density are potential sources of COVID-19, especially in Arab countries. In such settings, disease prevention raises serious concerns because of the potential impact of lockdowns, isolation, and quarantine (Fisher et al. 2020; Luttik et al. 2020; Joshi et al. 2020; Patnaik and Maji 2020; Brock and Laifer 2020). The resultant disturbances lead to mental health issues associated with anxiety, depression, insomnia, stress, and obsessions in various sections of the population, including children, older adults, and vulnerable sections (Joshi et al. 2020). As applied to Saudi Arabia, especially in the major cities characterized by modern lifestyles under nuclear families, this situation affected traditional family togetherness and cohesiveness. Nevertheless, the gap between reported and recovered cases has been reduced to a minimum, enabling successful treatment outcomes, albeit with few departures (Salam et al. 2022).
There were increases in the overall total cases and mortality, which were attributed to the waves of this epidemic on a global basis. However, threats are limited, as revealed by affected persons as a percentage of the population. Still, the epidemic outbreak in the country arouses curiosity about the changing social and cultural values of people and families at various localities across the country, creating threats. Thus, population rates are more meaningful than absolute numbers for understanding their impact on societies and neighborhoods. These rates indicate the extent to which COVID-19 has impacted the population: distribution, economy, behavior, and cohesiveness, both directly and indirectly. As of June 17, 2020, the daily reported cases reached a figure of 14 per 100,000 persons, fluctuating afterward with significant declines. Later, during the third wave, it hits 17 on January 19, 2022. Such increases threaten societies, families, and individuals, especially when the density of infected individuals is higher. It has many consequences on social, economic, and psychological health and manifests in many forms of distress.
Recoveries from COVID-19 rose faster by November 28, 2020, and thereafter, the gap between total cases and recoveries appeared to be converging, giving hope for no gap very soon, both at the family and individual levels a symbol of achievements of the mitigation strategy adopted. It will relieve society and family from many disturbances and suffering, causing burdens in the long run. At this point, efforts are made to achieve maximum recovery while minimizing infections. However, there was no decline in the number of deaths due to COVID-19. This could be due to many factors, such as the age of the infected person, population age structure, and comorbidities. Unfortunately, data on such demographics are unavailable for computation. None of the countries started offering data on the age and sex of patients with COVID-19 at the national level. Small sample surveys conducted at certain locations have generated such data but are insufficient for national-level interpretations.
However, large urban pockets have a smaller proportion of families and persons affected than certain medium-sized urban pockets. This raises concerns and considerations of increasing coverage of health intervention as well as familial support to medium-sized urban localities such as Hafar Al-Batin, Hofuf, Bisha, and Baish. These upcoming towns recorded a rapid spread and were analyzed as a share of the population. Such instances have serious repercussions on people’s lives at various levels of family and society, including the burden of epidemics, anxiety, and related neurotic conditions apart from the economics.
Manifestations to those in contact depend upon immunity leading to family tragedies and long progression causing widespread and interconnected human suffering: deaths, critical illness, disrupted economies, and social structures apart from the indirect effects of intense external boundaries of physical and emotional contacts, virtual connections, and migrations (Sun et al. 2020; Lebow 2020a, b; Luttik et al. 2020; Humphreys et al. 2020; Fraenkel and Cho 2020). Such ill effects could be curbed through interventions, especially awareness creation, combined with support systems. The government of Saudi Arabia offers several economic and medical welfare measures to protect the affected families (Ministry of Media 2020). These interventions should be continued for a further period, at least until the epidemic disappears, which is until the recovery of all patients, as advocated by Stokes and Patterson (2020) and Salam et al. (2022).
A rapidly increasing epidemic progression per population has been observed in most localities, especially in medium-sized cities and towns, rather than in metropolitan cities with a large population, including migrants. The progression in Qatif is the highest, followed by Hofuf, Khobar, and Dhahran in the order while analyzed as per 100,000 population. These northern localities border Kuwait, Bahrain, and Qatar; thus, frequent international traveling which appears to be the widest spread neighborhood, followed by Bisha and Hofuf. The progression of epidemics in these localities deserves serious consideration. This clearly explains the increased risk of infection, pointing out the possible flaws in the implementation of precautionary measures as per the recommendations. Large cities confined to procedural directions could reportedly control the spread to a large extent with existing infrastructural and social networking. However, the five large cities of Riyadh, Jeddah, Makkah, Madina, and Dammam have experienced a slow progression of COVID-19 in comparison with the upcoming townships. Thus, with this lesson in front, the Ministry of Health may take immediate steps for the strict implementation of control measures in these localities.
The results of this analysis show that the extent of the country’s population is affected, as are characteristics such as population size, density, and infrastructural development influencing spread of COVID-19. While the major cities with high population pressure could cope with the rapid spread of the epidemic in a short span, the upcoming medium-sized cities took a bit more time. It is a learning that such urban townships demand more care, concern, and control during instances of epidemics and similar calamities. Therefore, it can be inferred that a certain level of infrastructure networking is essential to address calamities, including epidemics, for which larger cities have an advantage.
Analyses and interpretations accounting for the total population as the denominator reflect the possible impact on the population and thereby society and family, which serve as a tool to address life at the grassroots level with welfare and benefits to uplift those in distress. This analysis was carried out with minimum publicly available data. However, this could enlighten academics to the extent possible. Detailed analyses are not amenable with this dataset, which is a limitation of this study. It would be advisable to analyze data at the national level for age, sex, and socioeconomic status through interventions that could teach lessons for the future. Such analyses are possible with the actual database of the Ministry of Health but not with the published capsuled data. We hope the researchers get an opportunity in the future to access the database and bring out detailed research reports and manuscripts for the benefit of the larger society.
Conclusions
The proportion of the population infected in society deserves special attention during an epidemic for many reasons, as it influences personal relations, intimacy, financial conditions, common forms of interpersonal communication, and patient care mechanisms. Day by day, the disease burden increases with the number of positive cases and fatalities but is comforted with recovery and improvement of living conditions. Although major cities in Saudi Arabia are negatively affected, they are less affected by population size than medium-sized upcoming cities and townships. Nevertheless, the probability of a rapid spread in densely populated metropolitan pockets and future cities cannot be neglected. Therefore, future-oriented welfare measures and policies to uplift populations and societies in crisis are required to save them from socioeconomic and relationship-related crises associated with the physical threats of COVID-19.
Availability of data and materials
This research used a compilation of daily status reports published by Ministry of Health, Saudi Arabia (www.moh.gov.sa). The compiled data, in Excel worksheet, may be made available on request.
References
Alkhamees AA, Alrashed SA, Alzunaydi AA et al (2020) The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. Compr Psychiatry 102:152192
Al-Knawy B, Adil M, Crooks G et al (2020) The Riyadh declaration: the role of digital health in fighting pandemics. Lancet 396(10262):1537–1539
Almaghlouth I, Islam T, Alamro N et al (2020) Mapping COVID-19 related research from Saudi Arabia, a scoping review: between reality and dreams. Saudi Med J 41(8):791–801
Al-Sulais ES, Mosli M, AlAmeel T (2020) The psychological impact of COVID-19 pandemic on physicians in Saudi Arabia: a cross-sectional study. Saudi J Gastroenterol 26(5):249–255
Barry M, Al-Amri M, Memish ZA (2020a) COVID-19 in the shadows of MERS-CoV in the Kingdom of Saudi Arabia. J Epidemiol Glob Health 10(1):1–3
Barry M, Ghonem L, Alsharidi A et al (2020b) Coronavirus disease-2019 pandemic in the Kingdom of Saudi Arabia: mitigation measures and hospital preparedness. J Nat Sci Med 3(3):155–158
Brock RL, Laifer LM (2020) Family science in the context of the COVID-19 pandemic: solutions and new directions. Fam Process 59:1007–1017
Fisher J, Languilaire J, Lawthom R et al (2020) Community, work, and family in times of COVID-19. Commun Work Fam 23(3):247–252
Fraenkel P, Cho WL (2020) Reaching up, down, in, and around: couple and family coping during the coronavirus pandemic. Fam Process 59(3):847–864
Hitchings E, Maclean M (2020) Unprecedented times: some thoughts on the consequences of the COVID-19 pandemic from a family and social welfare law perspective. J Soc Welf Fam Law 42(3):277–280
Humphreys KL, Myint MT, Zeanah CH (2020) Increased risk for family violence during the COVID-19 pandemic. Pediatrics 146(1):e20200982
Ibrahim N, Almeziny M, Alhamad A et al (2020) Local experience for managing oncology services during COVID-19 pandemic in a tertiary care hospital in Saudi Arabia. Glob J Med Ther 2(3):1–6
Iqbal MM, Abida I, Hussain S et al (2020) The effects of regional climatic condition on the spread of COVID-19 at global scale. Sci Total Environ 739:1401011-8
Joshi G, Hooda Y, Roy D (2020) Psychosocial repercussions of COVID-19. Int J Ment Health Psychiatry 6(3):1–4
Lebow JL (2020a) Family in the age of COVID-19. Fam Process 59(2):309–312
Lebow JL (2020b) COVID-19, families, and family therapy: shining light into the darkness. Fam Process 59(3):825–831
Luttik LMA, Mahrer-Imhof R, Brødsgaard CGA et al (2020) The COVID-19 pandemic: a family affair. J Fam Nurs 26(2):87–89
Michels NRM, Scherpbier N, Karppinen H et al (2020) Do you know how COVID-19 is changing general practice/family medicine education? Educ Prim Care 31(3):196–197
Ministry of media, Saudi Arabia. (2020). Saudi Arabia's ruthless fight against corona virus. Riyadh. Center for Government communications.
Motlhatlhedi K, Bogatsu Y, Maotwe K et al (2020) Coronavirus disease 2019 in Botswana: contributions from family physicians. Afr J Prim Health Care Fam Med 12(1):a2497
Patnaik NM, Maji S (2020) Psychological issues and stress on people in the purview of COVID-19 pandemic lockdown. Food Sci Rep 1(May Special issue):36–40
Salam AA, Al-Khraif RM, Elsegaey I (2022) COVID-19 in Saudi Arabia: an overview. Front Public Health 9:736942. https://doi.org/10.3389/fpubh.2021.736942
Stokes JE, Patterson SE (2020) Intergenerational relationships, family caregiving policy, and COVID-19 in the United States. J Aging Soc Policy 32(4–5):416–424
Sun J, Jiang Y, Lin W et al (2020) Different outcome of COVID-19 in members of a family. J Infect Dis Dev Ctries 14(5):447–449
Usher KAM, Bhullar N, Durkin J, Gyamfi N, Jackson D (2020) Family violence and COVID-19: increased vulnerability and reduced options for support. Int J Ment Health Nurs 29(4):549–552
Zhou ZM, Zhou HZ, Lin XD, Su ZC, Zhao LS, Chen X (2020) Outbreak of COVID-19 in a family, Wenzhou, China. Epidemiol Infect 148(e103):1–5
Acknowledgements
The authors would like to extend their sincere appreciation to the Deanship of Scientific Research at King Saud University, Riyadh, for its funding of this research through the Research Group No. RGP-329. Other than the authors, this research group includes Dr. Abdullah Al-Mutairi and Ms. Faten Al-Mutairi as team members. Thanks are due to Researchers support services unit of King Saud University for their assistance in language editing and to the anonymous reviewers for their advices at various stages of improvements. We would like to thank Editage (www.editage.com) for English language editing.
Funding
There are no funds received specific to this research. However, this research is carried out as part of the Research Group of Deanship of Scientific Research of King Saud University, Riyadh in Saudi Arabia.
Author information
Authors and Affiliations
Contributions
AAS involved in concept development, data compilation, analysis, and writing. RMK involved in overall guidance, enabling, advices on data management, analysis, and writing. DTR involved in Guidance on data analysis, epidemiological consultation, and review and revisions. IES involved in assistance on data collection, literature search, and analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
As this is based upon published data, ethics approval and consent to participate are not applicable.
Consent for publication
As this is based upon published data, consent for publication is not applicable. However, the authors express their consent to publish this manuscript in your esteemed journal.
Competing interests
There are no competing interests or conflict of interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Salam, A.A., Al-Khraif, R.M., Dilip, T.R. et al. Coronavirus disease 2019 in proportion to population: a historical analysis of Saudi Arabia. Bull Natl Res Cent 46, 198 (2022). https://doi.org/10.1186/s42269-022-00876-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42269-022-00876-z