
Abstract
Purpose
A breast cancer (BC) diagnosis may negatively affect health-related quality of life (HRQoL). However, there are few comparisons of HRQoL at several time points for women with BC, and particular when subdivided into invasive and in situ tumors. The purpose of this study was to investigate various aspects of HRQoL in women recently diagnosed with invasive BC or ductal carcinoma in situ (in situ) compared to age-matched BC free controls in a population-wide sample recruited through the Cancer Registry of Norway.
Methods
This cross-sectional study utilized HRQoL data collected in 2020–2022 from a digital survey including 4117 cases (3867 women with invasive BC and 430 with in situ) and 2911 controls. HRQoL was assessed ≥ 21 days after diagnosis, using EORTC QLQ-C30. This includes scores assessing global quality of life (gHRQoL) and HRQoL functions and symptoms. Multivariable regression analyses were used to compare HRQoL between cases and controls and to identify factors associated with gHRQoL and fatigue. Additionally, HRQoL 14 months after diagnosis was analyzed in 1989 of the included cases and in 1212 of the controls. Score differences of ≥ 10 points were considered clinically relevant and thus presented in the results.
Results
Invasive BC cases had lower gHRQoL, role- and social functioning in addition to more fatigue than controls. In situ cases had lower role—and social functioning than controls. Invasive BC cases scored worse than in situ on all domains, but the differences were not considered clinically relevant. Physical activity was associated with better gHRQoL and less fatigue in invasive BC, in situ and controls. Both invasive BC and in situ cases improved their role- and social functioning scores from diagnosis to 14 months follow-up, however no improvement was seen for fatigue.
Conclusion
Women with invasive BC and in situ reported lower role- and social functioning scores than controls right after diagnosis with improvements 14 months after diagnosis. Physical activity was associated with better gHRQoL and less fatigue and should, whenever possible, play a key role in the care for BC patients.
Similar content being viewed by others


Background
Due to advances in diagnostics and treatments, the 5-year relative survival rate for women with breast cancer (BC) is steadily increasing and has exceeded 90% in several western countries [1, 2]. Effective BC treatment is often associated with adverse effects ranging from minor and transient, to serious and persistent conditions [3]. This again can cause reductions in functioning, social participation, and health-related quality of life (HRQoL) in the affected individuals [3,4,5]. HRQoL covers the subjective perceptions of physical, emotional, social, and cognitive functions as well as disease symptoms and side effects of treatment [6]. One of the most common and distressing symptoms during and after BC treatment is fatigue [7, 8]. Given the long life expectancy after BC, an important goal is to alleviate adverse effects during and after cancer treatment and to enhance patients’ HRQoL [3]. To optimize such care, early identification of those most at risk of poor HRQoL is important [9, 10]. Some studies have found differences across several HRQoL domains between individuals with invasive BC, ductal carcinoma in situ (in situ) and controls both shortly after diagnosis [11, 12], and several years after BC diagnosis [11, 13,14,15]. These differences seem to be more prominent for the physical health parameters, and less in the well-being or mental health parameters [12, 13].
A healthy lifestyle can have beneficial effects on several aspects of HRQoL in BC survivors [16, 17], however, exactly which factors play a role and how, is not clear. In the present study, we utilized national, patient reported outcomes (PROs) data on HRQoL collected between 2020 and 2022 in the Cancer Registry of Norway (CRN)’s HRQoL-Survey [18].
The aims were to compare HRQoL between women with invasive BC or in situ cancer in the breast shortly after diagnosis (baseline) and age-matched BC free controls, and to study changes in global HRQoL (gHRQoL), role- and social functioning and fatigue from baseline to 14-month follow-up. Further, we aimed to study the associations between lifestyle factors and HRQoL among women with invasive BC, in situ cases and controls.
Material and methods
The Cancer Registry of Norway and the Norwegian Breast Cancer Registry
The CRN receives comprehensive information on all cancer diagnoses from several sources including pathology reports, doctors’ registrations and hospitals [1]. Reporting of cancer cases and cases of certain precancerous conditions to the registry is mandatory by law, providing close to complete data [19]. The CRN administers the Norwegian Breast Cancer Registry, which contains detailed information on BC characteristics and treatment. Information on BC characteristics in the current study were obtained from these registries.
The CRN HRQoL-Survey
The CRN has, since September 2020, administered the CRN HRQoL-Survey [18], an ongoing digital survey sent to individuals with different cancer types and age-matched controls. For BC, eligible cases are women aged ≥ 18 years when diagnosed with first occurrence of pathologically verified invasive BC (ICD10 = C50) or (ductal carcinoma) in situ (ICD10 = D05.9). According to the protocol, cases are invited from 21 days after date of the malignant biopsy to ensure that they are not invited to the survey before being informed about their BC diagnosis by their physician [18]. Potential controls are identified from the population registry and frequency matched to the distribution across age groups and region of residence of cases. Controls are randomly selected within these strata.
Individuals who use the official website for health communication in Norway (Helsenorge.no) or have an official digital mailbox (Digipost/e-box) are eligible and invited to the survey through this system. In 2020, the CRN were able to invite 79% of all individuals diagnosed with BC, whereas in 2022 the corresponding numbers were 86% [18]. The survey is available for 30 days, with a reminder sent to non-responders after 14 days.
At present, there are additionally two follow-up surveys sent to all women with BC. The first survey is sent about 14 months following diagnosis in BC cases (and on a similar date to controls), the second about 36 months following diagnosis.
In the present study, we included data on HRQoL measures from baseline (≥21 days following diagnosis), and also 14 months after diagnosis for a group of women diagnosed with BC and controls in a two-year period.
Participants
A total of 10,242 women diagnosed after August 1st, 2020, were invited between September 1st 2020 and December 31st, 2022. Among these cases, and the randomly sampled 11,364 age-matched controls, 8710 cases and 9005 controls could be invited digitally to the CRN HRQoL-Survey. A total of 4279 cases (49%) and 2911 controls (32%) responded. After more detailed review of the pathology records, we excluded 162 cases who did not have a malignant BC diagnosis during this period. Consequently, we included 4117 women with BC and 2911 controls in the analysis of baseline data. Of these, 1989 cases and 1212 controls also had data on the survey sent 14 months after diagnosis (Fig. 1).

Flowchart of participant inclusion. Breast cancer patients and controls were invited from September 2020 to December 2022 (this includes breast cancer patients diagnosed from August 2020)
Variables
The CRN HRQoL-Survey largely adheres to the International Consortium for Health Outcomes Measurement (ICHOM) standards [10]. The survey includes (among others) the European Organization for Research and Treatment of Cancer Quality of Life 30-item Questionnaire (EORTC QLQ-C30) which has been widely used to assess HRQoL in oncological studies [20], and selected self-reported sociodemographic and lifestyle questions.
Health-related quality of life
EORTC QLQ-C30 includes a global health status and quality of life (gHRQoL) scale, functioning scales (physical, role, emotional, cognitive and social), symptoms scales (fatigue, nausea and vomiting, pain), other common cancer-related symptoms items (dyspnoea, insomnia, appetite loss, constipation, diarrhoea) and financial difficulties.
The EORTC QLQ-C30 scales ranging from 0 to 100 were calculated according to the EORTC QLQ-C30 scoring manual. At least 50% of the items within a scale must be answered to receive a score on that domain [20, 21]. High scores on gHRQoL and functional scales implies better gHRQoL and higher functioning [20]. High scores on symptom scales/items imply more, or worse, symptoms [20]. In the current study, a between group difference of ≥ 10 points or more in EORTC QLQ-C30 scale scores was considered clinically relevant [22].
Sociodemographic data
For this study, sociodemographic information included age at survey-response, relationship status (categorized as in a relationship versus not), level of education (primary school/secondary school/high school or university ≤ 4 years/high school or university > 4 years), and employment status assessed by the question “Are you employed?” and categorized as employed vs non-employed (including retired). Physical activity included information on both exercise (regular activities of higher intensity, such as running of at least 30 min duration) and light intensity activities such as walking, biking and gardening. These were combined as follows: “No exercise, but light activity ≤ 3 hours per week” (i.e physically inactive), “no exercise, but light activity > 3 hours per week”, “exercise 0–1 hour per week”, “exercise 2–3 hours per week” and “exercise ≥ 4 hours per week”. Smoking was assessed by the questions: “Do you smoke?” and “If no, have you smoked previously” (Yes/No), and based on this information, categorized into current, former or never smoker. Alcohol consumption was assessed by the question: “Do you drink alcohol?” (Yes/No). Body mass index (BMI, kg/m²) was calculated from the self-reported height (m) and weight (kg).
Medical data
BC characteristics (stage, tumour characteristics etc.), and information on surgery/radiotherapy in relation to survey response were obtained from the CRN. Information on systemic BC therapies were unavailable.
Statistical analysis
Continuous variables were described by either means and standard deviations (SD) or median, minimum and maximum values (min-max), and categorical variables as numbers and percentages. Chi-square- and t-tests were used to compare differences between invasive BC, in situ and controls.
Multivariable linear regression models were used to compare mean differences in each of the HRQoL domains between groups at baseline. Univariable linear regression models were used to assess the change from baseline to 14 months after diagnosis for selected HRQoL domains. Multivariable linear regression models were also used to explore potential differences in associations between lifestyle, gHRQoL and fatigue separately in invasive BC, in situ cases and controls at baseline. All results are presented with 95% confidence intervals (95% CI). In all multivariable models, adjustments included the (a priori identified) potential confounding variables age (age groups), educational level, physical activity/exercise, smoking, alcohol use (yes/no) and BMI groups. To explore the strength of effects of each individual independent variable on gHRQoL and fatigue, we report the standardized β coefficients (std beta) from multivariable analysis. The std beta have standard deviations as their units, which allows for comparability across the set of independent variables [23].
All analyses were performed in Stata version 18.0 (StataCorp. 2023. Stata Statistical Software: Release 18. College Station, TX: StataCorp LLC.)
Sensitivity analyses
To address the influence of having surgery or radiation therapy, we conducted the analysis stratified by whether the cases had responded before or after surgery or radiation therapy. Women who did not have surgery at all were included in the “before surgery” category.
Results
Participant characteristics
Of the 4117 BC cases, 3867 (89.6%) were diagnosed with invasive BC, whereas 430 (10.4%) had in situ. Invasive and in situ BC cases were on average 58 years old at diagnosis and corresponding controls were 59 years. Most BC cases and controls had a partner, higher education and were employed. Lifestyle factors were similar among invasive BC, in situ and controls, with 13.5, 10.9 and 11.1% being inactive in the three groups. Mean BMI indicated slight overweight in all three groups (Table 1).
In total 49% of invasive BC cases were diagnosed and included at stage 1, and the majority of invasive BC cases were ER+ or PR+ and HER2‒. The median number of days between date of diagnosis (from pathology reports) to survey response were 47 (18–483) for invasive BC and 48 (21–257) for in situ, of which 47 and 45% respectively responded ≤ 1 month after diagnosis. In total 28% of invasive BC cases and 14% of in situ cases responded prior to surgery (including those who did not have surgery at all). Those who had surgery at time of survey completion had most frequently breast conserving therapy alone or in combination with radiation therapy (Table 2).
Differences in health-related quality of life in cases versus controls
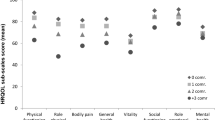
Invasive BC cases had lower scores [adjusted mean difference (95% CI)] on gHRQoL: [−9.82 (−10.83, −8.82)], role functioning [−19.66 (−21.02, −18.30)] and social functioning [−15.26 (−16.46, −14.06)] compared to controls. Furthermore, they reported a higher fatigue score (indicating more fatigue) [10.80 (9.66, 11.94)] compared to controls.
In situ cases had lower scores on role functioning [−14.71 (−17.52, −11.91)] and social functioning [−10.22 (−12.70, −7.74)], and higher score on fatigue [7.03 (4.68, 9.39)] compared to controls.
Invasive BC cases had slightly worse HRQoL scores than in situ cases, with the largest difference seen for social functioning [−5.04 (−7.49, −2.59)] (Table 3).
Difference from baseline to 14 months after diagnosis
From baseline to 14 months after diagnosis, both invasive BC and in situ cases experienced improvements in gHRQoL, role- and social functioning. The HRQoL scores for controls were largely unchanged from baseline to 14 months after diagnosis. The largest improvements were observed for in situ cases, particular for role-functioning [mean difference 13.9 (9.5, 18.3)]. There was little difference in the fatigue scores for all three groups (Table 4).
Lifestyle factors associated with gHRQoL
In invasive BC cases, weekly physical activity was associated with clinically relevant higher scores on gHRQoL, with the highest std beta (0.26) observed for exercise 2–3 times a week. A positive association between gHRQoL and some (versus totally avoiding) alcohol consumption with std beta 0.08 was also observed. Additionally, age groups ≥ 50 years were associated with higher scores on gHRQoL with std beta ≥ 0.15, while former smoking was associated with lower gHRQoL (-std beta −0.04).
The same positive associations for physical activity and drinking alcohol were seen for in situ cases with highest std beta 0.32 for exercise ≥ 4 times a week, and 0.14 for drinking alcohol. Contrary, former smoking (std beta-0.16) and higher body mass index (std beta −0.11 and −0.10 for overweight and obesity respectively) were negatively associated with gHRQoL. Compared to the lowest education level, higher educational level was associated with lower gHRQoL in in situ cases, but with wide confidence intervals.
The results for controls followed the same pattern as for cases for physical activity with highest std beta (0.23) for exercise ≥ 4 times. Age ≥ 50 years was positively associated with gHRQoL (std beta 0.14), whereas overweight/obesity and former/current smoking was negatively associated with gHRQoL (std beta −0.06/−0.14 and −0.06/−0.10) (Table 5).
Lifestyle factors associated with fatigue
Among invasive BC, higher levels of weekly physical activity and higher age (≥50 years) were inversely associated with fatigue, with the highest std beta (−0.25) for exercise 2–3 h per week. Drinking alcohol (compared to totally avoiding) was also associated with less fatigue with std beta −0.09. Former smoking was associated with more fatigue.
Among women with in situ, associations were similar. The highest std beta (−0.28) was observed for exercise > 4 h a week. Drinking alcohol was associated with less fatigue (std beta −0.13), whereas former smoking and overweight (compared to normal weight) were associated with more fatigue (std beta 0.17 and 0.15, respectively).
For controls, increasing physical activity levels were associated with less fatigue, with highest std beta for exercise > 4 h a week (−0.21). Age 50–69 and alcohol consumption were also associated with less fatigue among controls, while overweight/obesity and former/current smoking were associated with more fatigue (Table 6).
Sensitivity analyses
We compared HRQoL differences between those who responded to the survey prior to surgery and/or radiation therapy or did not have surgery/radiation therapy (n = 1020 invasive and n = 61 in situ), to those who had received surgery or radiation therapy at time of survey response (n = 2667 invasive, n = 369 in situ). Except for role functioning, the case-control differences were somewhat larger prior to surgery than after surgery. However, the differences were generally small, except for the case-control difference for social functioning which was larger for those who responded prior to surgery −19.4 (−21.1, −17.6) compared to after surgery −13.4 (−14.6, −12.2) (Supplementary File 1).
Discussion
Main findings
We found that invasive BC cases as well as those with in situ tumours had clinically relevant lower scores on role- and social functioning right after diagnosis compared with controls. Invasive BC cases also had lower gHRQoL and more fatigue. The role- and social functioning scores of invasive BC and in situ cases were higher at 14 months after diagnosis, but there was no change in fatigue scores. Physical activity was the strongest predictor for high HRQoL and most strongly inverse predictor of fatigue among both cases and controls.
HRQoL in invasive BC and in situ cases and controls
The clinically relevant lower scores of role- and social functioning for both invasive and in situ cases are in line other studies on BC patients demonstrating differences across several HRQoL domains about 6 weeks after diagnosis [11]. Invasive BC cases had worse HRQoL than in situ cases, in line with other studies [12, 13, 24], however no between-group differences were considered clinically relevant. Most invasive BC cases in our study were diagnosed at stage I and II, thus lower HRQoL scores could have been excepted if we ought to include more advanced stage BC patients [25].
We suspect that the disruptions found in several domains such as role- and social functioning in both invasive BC and in situ cases compared to controls partly reflect the negative effects of BC therapies on these women’s ability to work (58% of invasive BC cases and 62% of in situ cases were employed) and participate in everyday activities [26]. Results emphasizing lower social functioning in women with BC compared to controls have been demonstrated in other studies [27, 28] and is associated with pessimism [27, 28]. One might suspect that in general, individuals with more pessimistic personality traits might seek and have less social support available, leaving them at greater risk of experiencing low overall HRQoL. Reasuringly, both invasive BC and in situ cases had significant improvements in role- and social functioning from baseline to 14 months after diagnosis, in line with other studies in BC survivors [15, 29]. The improvements were largest for in situ cases, indicating they to a larger extent than invasive BC cases are “back to normal”, in terms of leisure activities etc., a little more than 1 year after diagnosis. In the Pink SWAN study, BC survivors had worse HRQoL at diagnosis and 1-year follow up compared to the control group, however after 2 years there was no significant difference between the groups [14]. It remains to be elucidated if a similar pattern is observed at the 36-month follow-up of the CRN HRQoL-Survey.
About 20–30% of BC survivors experience persistent fatigue up to 10 years after diagnosis [7, 8]. We observed a slightly higher fatigue score in invasive BC than in situ cases shortly after diagnosis, with somewhat larger case-control difference in those who responded prior to surgery or radiation therapy (adjusted mean difference 12.9 (11.3, 14.6) compared to post surgery (9.6 (8.5, 10.8). This may suggest that the fear of BC during the diagnostic work-up may already have induced fatigue and negatively impacted their HRQoL at the time of diagnosis. Moreover, there was minimal change in the fatigue scores from baseline to 14 months after diagnosis for both invasive BC and in situ cases, supporting that fatigue may persist long beyond the main treatment period [15, 27, 30,31,32]. Consequently, assessing fatigue symptoms and early identification of those most at risk of low HRQoL is paramount to offer early effective intervention and optimized follow-up aiming to hinder persistent low HRQoL in women diagnosed with BC. Such interventions, including psychosocial stress management interventions, psychoeducational support and physical rehabilitation [33, 34], are effective to mitigate the negative consequences of diagnosis and treatment [14, 27, 32,33,34,35]. Our study points to close follow-up of the HRQoL among women with invasive BC shortly after diagnosis for several HRQoL measures with additional long-term follow-up of both invasive BC and in situ cases when it comes to fatigue. In Norway, implementation of “standardized pathway HOME” is ongoing, exactly aiming to improve this part of cancer care [36].
Lifestyle factors affecting gHRQoL and fatigue
Being physically active was associated with better gHRQoL and less fatigue in invasive BC and in situ cases, in line with other studies in this patient group [16, 17, 37]. This study thus emphasizes physical activity as an important, low threshold self-management strategy for BC patients [3, 38]. The evidence regarding specific types or doses of physical activity unique for BC survivors is however limited [37]. We found stronger associations with HRQoL for exercising 2–4 h week (compared to less) in both BC cases and controls, and for invasive BC cases and controls the results indicated that “the more the exercise the better”. This observation is supported by a study showing that low physical activity is associated with HRQoL deterioration [39].
The association between lifestyle factors and HRQoL seemed to be stronger for in situ cases than invasive BC cases, indicating that the severity of the disease may impact lifestyle factors which again impacts HRQoL [25]. Nevertheless, we found that drinking alcohol was associated with better gHRQoL and less fatigue among both cases and controls. These findings are in agreement with a Chinese study, which reported that drinking alcohol was associated with better HRQoL among more than 1000 women diagnosed with BC within the last two weeks [40]. The apparently positive effects of alcohol could be due to moderate alcohol intake in social settings [41, 42]. Besides lifestyle factors, the negative association between higher education and gHRQoL was surprising, however there were only 27 women in the lowest education group so these results may be a result of random variation.
The survey did not assess dietary factors, but previous studies have shown that a healthy dietary pattern also has positive effects on HRQoL [43], and should therefore be part of the recommended lifestyle in this patient group. Emphasize on continued healthy lifestyle beyond diagnosis and treatment is important, as recent evidence indicates that insufficient physical activity, excess body weight and smoking predict worsening of HRQoL the next years [39, 44].
Strengths and limitations
The main strength of this study is the nationwide sample of women with BC recruited through CRN, yielding a large sample size, and avoiding the potential biases arising from recruiting through cancer centers or restricted geographical areas. This solely digital CRN HRQoL-survey reached ≥ 79% of all women diagnosed with BC diagnosis in Norway after 2020 [45]. The survey largely consists of well-established and validated PROs that allow us to assess the effects of many factors simultaneously. The CRN started sending surveys to BC patients in late September 2020, therefore all surveys were completed after the start of the pandemic, and we have previously demonstrated, in the same sample of BC survivors and controls, that the case-control differences were similar across different COVID-19 phases [46].
The current study also has limitations. We do not have information on systemic BC treatment, but there are national guidelines and adherence to these are monitored through the Norwegian Breast Cancer Registry [45]. HRQoL and lifestyle factors were self-reported, which are subject to errors. Our response rate was moderate, 49% among cases and 32% among controls. Although the response rate in BC cases was similar or better than two postal PROs-surveys in Ireland and Australia using cancer registries as sampling frames [47, 48], we cannot exclude the possibility of response bias affecting our results. Furthermore, both cases and controls have on average higher education than the general population [49]. Finally, even if no response bias, generalization of the results may be limited to Norwegian women who are digitally active (80–90%).
Conclusion
Invasive BC cases had worse HRQoL measures than controls and in situ BC cases shortly after diagnosis with improvements observed 14 months later. The fatigue scores were however not improved 14 months after diagnosis, and thus early identification and consequently interventions to improve fatigue in BC survivors is warranted. Early interventions should include physical activity as this was the strongest inverse predictor of fatigue, and the largest contributor to better gHRQoL among invasive BC and in situ cases and controls.
Data availability
Raw data were generated at CRN. Derived data supporting the findings of this study are available from the corresponding author [KS] on request.
References
Cancer Registry of Norway (2021) Cancer in Norway 2020 - cancer incidence, mortality, survival and prevalence in Norway. Cancer Registry of Norway, Oslo
Siegel RL et al (2022) Cancer statistics, 2022. CA Cancer J Clin 72(1):7–33
Runowicz CD et al (2016) American cancer society/American society of clinical oncology breast cancer survivorship care guideline. J Clin Oncol 34(6):611–635
Ewertz M, Jensen AB (2011) Late effects of breast cancer treatment and potentials for rehabilitation. Acta Oncologica 50(2):187–193
Aziz NM (2007) Cancer survivorship research: state of knowledge, challenges and opportunities. Acta Oncologica 46(4):417–432
EORTC (2022). Quality of life. Available from https://qol.eortc.org/quality-of-life/. Cited 19 Oct 2022
Reinertsen KV et al (2010) Predictors and course of chronic fatigue in long-term breast cancer survivors. J Cancer Surviv 4(4):405–414
Bower JE (2014) Cancer-related fatigue: mechanisms, risk factors, and treatments. Nat Rev Clin Oncol 11(10):597–609
Reeve BB et al (2013) ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual Life Res 22(8):1889–1905
Ong WL et al (2017) A standard set of value-based patient-centered outcomes for breast cancer: the International Consortium for Health Outcomes Measurement (ICHOM) initiative. JAMA Oncol 3(5):677–685
Jeffe DB et al (2012) Quality of life over time in women diagnosed with ductal carcinoma in situ, early-stage invasive breast cancer, and age-matched controls. Breast Cancer Res Treat 134(1):379–391
Lauzier S et al (2010) Psychological distress and physical health in the year after diagnosis of DCIS or invasive breast cancer. Breast Cancer Res Treat 120(3):685–691
van Gestel YRBM et al (2007) A comparison of quality of life, disease impact and risk perception in women with invasive breast cancer and ductal carcinoma in situ. Eur J Cancer 43(3):549–556
Avis NE et al (2020) Health-related quality of life among breast cancer survivors and noncancer controls over 10 years: pink SWAN. Cancer 126(10):2296–2304
Tran TXM et al (2023) Long-term trajectory of postoperative health-related quality of life in young breast cancer patients: a 15-year follow-up study. J Cancer Surviv 17(5):1416–1426
Meneses-Echavez JF, Gonzalez-Jimenez E, Ramirez-Velez R (2015) Effects of supervised exercise on cancer-related fatigue in breast cancer survivors: a systematic review and meta-analysis. BMC Cancer 15:77
Lahart IM et al (2018) Physical activity for women with breast cancer after adjuvant therapy. Cochrane Database Syst Rev 1(1):Cd011292
Gjelsvik Y, Johannesen TB, Ursin G, Mykelbust TÅ (2022) A nationwide prospective collection of patient reported outcomes in the Cancer Registry of Norway. Norsk Epidemiologi
Nilbert M et al (2020) The power of empirical data; lessons from the clinical registry initiatives in Scandinavian cancer care. Acta Oncologica 59(11):1343–1356
Aaronson NK et al (1993) The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 85(5):365–376
Fayers PM, Bjordal AN, Groenvold K, Curran M, Bottomley D, A O, b.o.t.E.Q.o.L. Group (2001) The EORTC QLQ-C30 scoring manual, 3rd edn. European Organisation for Research and Treatment of Cancer, Brussels
Osoba D et al (1998) Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol 16(1):139–144
Statistics How to. Standardized beta coefficient: definition & example. Available from https://www.statisticshowto.com/standardized-beta-coefficient/. Cited 14 June 2023
Sun F-K et al (2023) Social functioning, depression, and quality of life among breast cancer patients: a path analysis. Eur J Oncol Nurs 62:102237
Roy P et al (2023) Identifying at risk populations amongst breast cancer survivors and their common symptoms and concerns. BMC Womens Health 23(1):302
Gamper E-M et al (2016) Development of an item bank for the EORTC Role Functioning Computer Adaptive Test (EORTC RF-CAT). Health Qual Life Outcomes 14(1):72
Goyal NG et al (2018) Trajectories of quality of life following breast cancer diagnosis. Breast Cancer Res Treat 169(1):163–173
Schou I et al (2005) Multiple predictors of health-related quality of life in early stage breast cancer. Data from a year follow-up study compared with the general population. Qual Life Res 14(8):1813–1823
Moro-Valdezate D et al (2013) Evolution of Health-Related Quality of Life in breast cancer patients during the first year of follow-up. J Breast Cancer 16(1):104–111
Bower JE et al (2006) Fatigue in long-term breast carcinoma survivors: a longitudinal investigation. Cancer 106(4):751–758
Reinertsen KV et al (2017) Fatigue during and after breast cancer therapy-a prospective study. J Pain Symptom Manage 53(3):551–560
Koch L et al (2013) Quality of life in long-term breast cancer survivors - a 10-year longitudinal population-based study. Acta Oncol 52(6):1119–1128
Caccia D et al (2017) Quality of life after invasive or breast-conserving surgery for breast cancer. Breast J 23(2):240–242
Carlson LE (2023) Psychosocial and integrative oncology: interventions across the disease trajectory. Annu Rev Psychol 74:457–487
Antoni MH, Moreno PI, Penedo FJ (2023) Stress management interventions to facilitate psychological and physiological adaptation and optimal health outcomes in cancer patients and survivors. Annu Rev Psychol 74:423–455
“Standardized pathway home”/Pakkeforløp for pasienter med kreft (2021) Available from https://www.helsedirektoratet.no/nasjonale-forlop/hjem-for-pasienter-med-kreft. Cited 05 July 2023
Aune D et al (2022) Physical activity and health-related quality of life in women with breast cancer: a meta-analysis. JNCI Cancer Spectr 6(6)
Campbell KL et al (2019) Exercise guidelines for cancer survivors: consensus statement from international multidisciplinary roundtable. Med Sci Sports Exerc 51(11):2375–2390
Franzoi MA et al (2024) Patient-reported quality of life 6 years after breast cancer. JAMA Network Open 7(2):e240688–e240688
Zheng C et al (2021) Relationship between lifestyle habits and health-related quality of life of recently diagnosed breast cancer patients: a comparison between younger and older women in China. Front Public Health 9:767151
Marchand A et al (2003) The moderating effect of alcohol intake on the relationship between work strains and psychological distress. J Stud Alcohol 64(3):419–427
Standridge JB, Zylstra RG, Adams SM (2004) Alcohol consumption: an overview of benefits and risks. South Med J 664+
Rim CH et al (2019) Questionnaire study of the dietary habits of breast cancer survivors and their relationship to quality of life (KROG 14-09). Eur J Cancer Care 28(2):e12961
Meglio AD et al (2022) Dynamics of long-term patient-reported quality of life and health behaviors after adjuvant breast cancer chemotherapy. J Clin Oncol 40(27):3190–3204
Årsrapport 2022 med resultater og forbedringstiltak fra Nasjonalt kvalitetsregister for brystkreft (2023) Oslo, Kreftregisteret
Svendsen K et al (2024) How did breast cancer patients fare during different phases of the COVID-19 pandemic in Norway compared to age-matched controls? Cancers 16(3):602
Skandarajah AR et al (2021) Patient-reported outcomes in survivors of breast cancer one, three, and five years post-diagnosis: a cancer registry-based feasibility study. Qual Life Res 30(2):385–394
Drummond FJ et al (2015) Establishing a population-based patient-reported outcomes study (PROMs) using national cancer registries across two jurisdictions: the Prostate Cancer Treatment, your experience (PiCTure) study. BMJ Open 5(4):e006851
Statistics Norway (2024) Educational attainment of the population. Available from https://www.ssb.no/en/utdanning/utdanningsniva/statistikk/befolkningens-utdanningsniva. Cited 16 May 2024
Acknowledgements
We thank the Centre on Patient Reported Outcomes Data at Haukeland University Hospital for counseling regarding which PROs to include in the CRN HRQoL-Survey questionnaire.
Funding
Open access funding provided by Norwegian Institute of Public Health (FHI). The study is part of the Coping After Breast Cancer study that is funded by the Norwegian Breast Cancer Society’s “Pink Ribbon” charity funding (ID 197409-2019. PI Giske Ursin).
Open access funding provided by Norwegian Institute of Public Health (FHI)
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by A.B., T.Å.M. The first draft of the manuscript was written by S.K.H.B. and K.S. and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Participants consented to participation by electronically signing (eSigning) when returning their questionnaires. By participating, the survey participants consent to their survey data being linked to data that may be registered about them in statutory health registries, for instance the CRN, and Statistics Norway. These possible linkages are described in the invitation letter to the CRN HRQoL- Survey. The legal basis of data processing in the CRN, as well as the CRN HRQoL-Survey is the Regulations EU 2016/679 of the European Parliament and of the Council of 27 April 2016 (GDPR), supplemented by national law (the Cancer Registry Regulations and the Health Registry Act, as well as the Norwegian Regulations on Population Based Health Surveys).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bøhn, S.K.H., Svendsen, K., Balto, A. et al. Health-related quality of life among women diagnosed with in situ or invasive breast cancer and age-matched controls: a population-based study. J Patient Rep Outcomes 8, 105 (2024). https://doi.org/10.1186/s41687-024-00781-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41687-024-00781-1