
Abstract
Background
The aim of this study was to evaluate the root canal morphology of mandibular first molars in a Chinese population by using cone-beam computed tomography (CBCT).
Methods
In this study, CBCT images of 900 mandibular first molars were evaluated for the following details: (1) number of roots, (2) number of apical foramina, (3) frequency distribution of root canal configurations defined in accordance with Vertucci’s classification, and (4) frequency of occurrence of middle mesial (MM) canal.
Results
Overall, 74.9% of the evaluated mandibular first molars possessed two roots, and 55.4% exhibited three apical foramina. The evaluated teeth exhibited a relatively high prevalence of type IV canals in mesial (M) roots (76.8%) and type I canals in the distal (D) (79.4%), distobuccal (DB) (98.7%), and distolingual (DL) (100%) roots. There were no significant differences in the number of roots, incidence of apical foramina, or distribution of different canal configurations of mandibular first molars between men and women (P > 0.05). 1.9% of mandibular first molars possessed three mesial canals, and the highest frequency of occurrence of MM canals (4.1%) was among Chinese people below the age of 30 years.
Conclusions
CBCT scanning facilitates identification of the root canal system. In order to increase the success rate of treatment, it is important to obtain information about the variable morphology of root canals before endodontic treatment.
Trial registration
TJSKE20160412. Registered 12 April 2016.
Similar content being viewed by others

Background
Permanent mandibular first molars exhibit a wide variation in root canal anatomy. They appear to be the tooth type that most often requires root canal treatment (Silva et al. 2013). Long-term success of endodontic treatment depends on complete cleaning, shaping, and filling of all existing canals (Tian et al. 2016; Zheng et al. 2010). The highly variable morphology of the root canal system presents clinical challenges that mainly affect the results of chemomechanical preparation (Versiani et al. 2011). In order to increase the success rate of root canal treatment, it is essential that clinicians have thorough knowledge of anatomic variations of the root canal system.
According to previous studies, a common root and canal configuration of mandibular first molars involves two roots with one or two canals in the distal (D) root and two canals in the mesial (M) root, characterized by a widened buccolingual surface and flattened mesiodistal surface (Tian et al. 2016). A systematic review has reported the incidences of three, four, and five root canals in mandibular first molars to be 61.3, 35.7, and about 1%, respectively (de Pablo et al. 2010). In 1974, Vertucci and Williams identified the presence of the middle mesial (MM) canal in mandibular first molars (Vertucci and Williams 1974). An MM canal is occasionally observed in the developmental groove between the mesiobuccal (MB) and mesiolingual (ML) canals, with an incidence of 0.95–15% (Aminsobhani et al. 2010; Navarro et al. 2007). Sundaresh et al. reported five canal orifices (three M and two D) in the pulp chamber of a mandibular first molar in their case report (Sundaresh et al. 2013). Sharma et al. reported a case about endodontic management of a mandibular first molar with six canals (three canals in the M root and three in the D root) (Sharma et al. 2016). These studies serve to demonstrate the anatomic variation of root canals in mandibular first molars.
Several techniques, including intraoral periapical radiography, use of transparent samples and polyester resin impressions, and sectioning, have been used for in vivo and in vitro evaluation of root canal morphology (Chen et al. 2009; Martos et al. 2010; Navarro et al. 2007; Yew and Chan 1993). However, because of superimposition of dental structures or irreversible changes to tooth samples, the results obtained by these methods are not completely reliable (Song et al. 2010). Cone-beam computed tomography (CBCT) allows accurate and immediate three-dimensional (3D) reconstruction imaging of axial, sagittal, and coronal planes and minimizes the superimposition of dental structures (Zhang et al. 2011; Zhang et al. 2011). Matherne et al. demonstrated that CBCT image analysis provides more accurate data about root canal systems than digital radiograph analysis (Matherne et al. 2008). For this reason, CBCT is used as a noninvasive tool in endodontic treatment for effective evaluation of root and canal morphologies (Cotton et al. 2007; Nair and Nair 2007; Patel et al. 2007; Tyndall and Rathore 2008).
To date, few studies have evaluated the root canal morphology of mandibular first molars according to sex or the incidence of MM canals according to age in a Chinese population. Therefore, this study aimed to evaluate the variation of root canal morphology in permanent mandibular first molars in a Chinese population by using CBCT.
Methods
CBCT images of 900 mandibular first molars were acquired from 646 patients (female, 344; male, 302; age, 13–82 years) who visited the hospital, between May and September 2016. These images had been acquired as a part of preoperative assessment for root canal treatment, implant surgery, or orthodontic treatment. Mandibular first molars were selected in accordance with the following criteria: (1) mature teeth with completely formed roots and (2) mandibular first molars without carious cavities, root resorption, root canal treatment, or restoration. The procedure for collection of imaging data was explained to the patients or legal guardians, and appropriate informed consent was obtained.
Image acquisition and analysis
Images were acquired using a CBCT device (J. Morita Mfg. Corp., Kyoto, Japan) operated at 80 kVp and 5 mA, with field of view of 8 cm × 8 cm, a scanning time of 9.4 s, and slice thickness of 0.125 mm. Image acquisition was performed by an experienced oral radiologist in accordance with the manufacturer’s instructions. The images were then adjusted and analyzed using the Volume Viewer software. Serial sagittal, coronal, and axial images were analyzed independently by two endodontists and an oral radiologist. Disagreements were settled by discussion for reaching a consensus. Additionally, 20% of the images were randomly selected and reevaluated by the three examiners after 2 months. The kappa value for repeatability was 0.9, which indicated that the data were reliable.
CBCT images of mandibular first molars were evaluated for the following details: (1) number of roots according to sex, (2) number of apical foramina according to sex, (3) frequency distribution of root canal configurations defined in accordance with Vertucci’s classification, and (4) frequency of occurrence of MM canals according to age.
The MM images of each layer were imported into the Mimics software (Mimics, V 10.01, Materialise, Belgium) and edited to create closed contours according to the gray scale of enamel, dentine, and pulp, respectively. This contour on different layers was matched to reconstruct the 3D surface model of the root canals.
Statistical analysis
Data were recorded, tabulated, and analyzed for descriptive statistics using the SPSS 22.0 software (IBM Corp, Armonk, NY, USA). The chi-square test was used for the comparison of number of roots and apical foramina between the sexes. The distribution frequency of root canal morphologies was analyzed with the Fisher exact and chi-square tests. Differences in frequency of occurrence of MM canals according to age were analyzed with the chi-square test. Significant differences were considered at P < 0.05.
Results
Number of roots in mandibular first molars according to sex
A total of 900 CBCT images were selected in accordance with the inclusion criteria. As shown in Table 1, the percentages of two- and three-rooted mandibular first molars were 74.9% (674/900) and 25.0% (225/900), respectively. A mandibular first molar with fused roots was detected, where it was difficult to distinguish the M and D roots. The numbers of mandibular first molars with two roots (M and D roots) among the female and male patients were 344 (73.3%) and 330 (76.6%), respectively; the corresponding numbers of teeth with three roots (M, distobuccal (DB), and distolingual (DL) roots) were 125 (26.7%) and 100 (23.2%), respectively. There was no significant difference in the distribution frequency of number of roots in mandibular first molars between the sexes (P > 0.05).
Number of apical foramina in mandibular first molars according to sex
The frequency of number of apical foramina was evaluated by CBCT images of axial plane and following the coronal to apical direction. Table 2 presents the number and distribution of apical foramina among the 900 eligible mandibular first molars. While 134 teeth (14.9%) possessed two apical foramina (M and D), 499 (55.4%) and 267 (29.7%) mandibular first molars exhibited three (MB, ML, and D) and four apical foramina (MB, ML, DB, and DL), respectively. The frequencies of occurrence of two, three, and four apical foramina among the female patients were 13.6% (64/469), 55.4% (260/469), and 30.9% (145/469), respectively; the corresponding frequencies among the male patients were 16.2% (70/431), 55.5% (239/431), and 28.3% (122/431). There were no significant differences in the frequencies of occurrence of apical foramina in mandibular first molars between the sexes (P > 0.05).
Distribution of root canal configurations in mandibular first molars according to sex
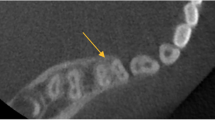
Table 3 and Fig. 1 present the variations in root canal configurations of mandibular first molars. Among the 899 evaluated two- and three-rooted mandibular first molars, the most common root canal configuration in M roots was type IV (690/899; 76.8%), followed by types II (149/899; 16.6%), I (27/899; 3.0%), V (12/899; 1.3%), III (3/899; 0.3%), and VI (1/899; 0.1%); in addition, 17 teeth (1.9%) exhibited three mesial canals (type VIII+). All MM canals merged with ML canals at the apical or middle third level. In D roots, type I root canal configuration (535/674; 79.4%) was the most prevalent, followed by type II (43/674; 6.4%). Among DB roots, 98.7% (222/225) exhibited type IV canal configuration, while 1.3% (3/225) exhibited type II configuration. All DL roots possessed type I root canals. There were no significant differences in the distribution frequencies of different canal configurations among M, D, DB, or DL roots of mandibular first molars between the sexes (P > 0.05).

Examples of root canal anatomy: (a) CBCT images of coronal plane in mandibular first molars, (b) CBCT images of sagittal plane in M roots, (c) CBCT images of sagittal plane in D roots, and (d–f) CBCT images of axial plane in mandibular first molars
Frequency of occurrence of MM canals according to age
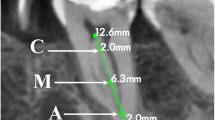
The overall frequency of occurrence of MM canals was 1.9% (17/899). Table 4 presents the distribution frequency of MM root canals in three age groups (groups A–C: < 30, 30–50, and > 50 years). Among these age groups, group A exhibited a greater occurrence of MM canals (10/241; 4.1%) than group B (6/431; 1.4%) or C (1/227; 0.4%; P = 0.003). All MM canals merged with ML canals in the apical or middle third level by observing the 3D surface models of the root canals (Fig. 2).

The 3D surface model of the root canal. a, b MM canal merged with ML canal
Discussion
In root canal treatment, overlooked canals may hinder the effectiveness of the shaping, cleaning, and filling procedures and lead to microbial colonization, thus affecting the prognosis of endodontic treatment. Therefore, it is necessary to always evaluate the root canal system at the start of the treatment. Clinical and radiographic examinations are essential methods used for evaluating root canals and detecting most anatomic variations (Mukhaimer 2014). In this study, we evaluated the anatomic variations of the root canal system in vivo by using CBCT. Several studies have demonstrated that serial sagittal, coronal, and axial views allow excellent visualization of root canal anatomy, and the number of roots and canals can be visually evaluated in serial axial images acquired by CBCT at a low radiation dosage. Blattner et al. and Zheng et al. demonstrated the reliability of CBCT in detecting the second mesiobuccal (MB2) canal in maxillary first molars (Blattner et al. 2010; Zheng et al. 2010). Wang et al., too, evaluated the root canal morphology of mandibular first molars by CBCT and indicated that CBCT is a useful tool for the study of anatomic variations (Wang et al. 2010).
In general, mandibular first molars have two roots, located mesially and distally (de Pablo et al. 2010). In the present study, two-rooted mandibular first molars (74.9%) were greater in proportion than three-rooted ones (25.0%); this proportion of two-rooted mandibular first molars is lower than that reported in a Brazilian population (87%) but higher than that reported in Korean children (66.9%) (Silva et al. 2013; Song et al. 2009). However, the present results are in general agreement with those of a previous study in a western Chinese population, in which 73.5 and 25.8% of mandibular first molars possessed two and three roots, respectively (Wang et al. 2010). The incidence of four roots in mandibular first molars is rare and has only been reported in three cases to date (Friedman et al. 1986; Ghoddusi et al. 2007; Lee et al. 2006). Four-rooted mandibular first molars were not detected among the present 900 CBCT images. As shown in Table 2, mandibular first molars with three apical foramina (55.4%) were greater in proportion than those with four (29.7%) or two (14.9%) apical foramina. This anatomic variation could be evaluated by 3D image analysis, which allows accurate observation in the sagittal, coronal, and axial directions, ultimately leading to accurate conclusions about the number of roots and apical foramina.
In the present study, the most frequent canal configuration among M roots was type IV (76.8%), followed by type II (16.6%); among D roots, the most frequent canal configuration was type I (79.4%), followed by type II (6.4%). In a Palestinian population, Mukhaimer et al. found that the most common canal configurations among M and D roots were types IV (53.8%) and I (57.5%), respectively, followed by type II (both; 38.8 and 22.5%, respectively) (Mukhaimer 2014). Mohammadzadeh Akhlaghi et al. also found types IV (55.3%) and I (61.3%) to be the most common canal configurations among M and D roots in an Iranian population (Mohammadzadeh Akhlaghi et al. 2017). The differences in distribution frequencies of root canal configurations between the present and previous studies might be because of differences in analysis methods or ethnicity of study populations.
In most studies, M roots have most frequently been described as possessing two canals. However, three canals are occasionally observed in M roots in cases where the isthmus between the MB and ML canals is clinically evident. The isthmus is one of the more difficult clinical challenges because the area is complex and not easy to clean thoroughly by mechanical preparation. As shown in Tables 3 and 4, 1.9% of mandibular first molars in the present study possessed three mesial canals, and the highest frequency of occurrence of MM canals was among patients in the age group A (< 30 years) (4.1%). In most case reports to date, the MM canal has been shown to join the MB or ML canal at the apical third level (Aminsobhani et al. 2010; Reyhani et al. 2007; Sharma et al. 2016). In the present study, all MM canals merged with ML canals in the apical or middle third level, and we found no instances of three independent canals in the M root. These findings suggest that endodontists should pay greater attention to the occurrence of MM canals among Chinese people below the age of 30 years.
The limitation of our study protocol was the small sample size of different ethnic groups. Further research is warranted to evaluate the variation of root canal morphology in permanent mandibular first molars among different ethnic groups with larger sample sizes.
Conclusions
Mandibular first molars most commonly possess two roots. The most common canal configurations were types IV, I, and II. The highest frequency of MM canals occurs in the population below the age of 30 years. No statistically significant differences were found between the sexes in terms of number of roots, incidence of apical foramina, or distribution of different canal configurations of mandibular first molars.
Abbreviations
- 3D:
-
Three-dimensional
- CBCT:
-
Cone-beam computed tomography
- D:
-
Distal
- DB:
-
Distobuccal
- DL:
-
Distolingual
- M:
-
Mesial
- MB:
-
Mesiobuccal
- MB2:
-
The second mesiobuccal
- ML:
-
Mesiolingual
- MM:
-
Middle mesial
References
Aminsobhani M, Bolhari B, Shokouhinejad N, Ghorbanzadeh A, Ghabraei S, Rahmani MB. Mandibular first and second molars with three mesial canals: a case series. Iran Endod J. 2010;5:36–9.
Blattner TC, George N, Lee CC, Kumar V, Yelton CD. Efficacy of cone-beam computed tomography as a modality to accurately identify the presence of second mesiobuccal canals in maxillary first and second molars: a pilot study. J Endod. 2010;36:867–70.
Chen G, Yao H, Tong C. Investigation of the root canal configuration of mandibular first molars in a Taiwan Chinese population. Int Endod J. 2009;42:1044–9.
Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG. Endodontic applications of cone-beam volumetric tomography. J Endod. 2007;33:1121–32.
de Pablo OV, Estevez R, Peix Sanchez M, Heilborn C, Cohenca N. Root anatomy and canal configuration of the permanent mandibular first molar: a systematic review. J Endod. 2010;36:1919–31.
Friedman S, Moshonov J, Stabholz A. Five root canals in a mandibular first molar. Endod Dent Traumatol. 1986;2:226–8.
Ghoddusi J, Naghavi N, Zarei M, Rohani E. Mandibular first molar with four distal canals. J Endod. 2007;33:1481–3.
Lee SJ, Jang KH, Spangberg LS, Kim E, Jung IY, Lee CY, Kum KY. Three-dimensional visualization of a mandibular first molar with three distal roots using computer-aided rapid prototyping. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:668–74.
Martos J, Lubian C, Silveira LF, Suita de Castro LA, Ferrer Luque CM. Morphologic analysis of the root apex in human teeth. J Endod. 2010;36:664–7.
Matherne RP, Angelopoulos C, Kulild JC, Tira D. Use of cone-beam computed tomography to identify root canal systems in vitro. J Endod. 2008;34:87–9.
Mohammadzadeh Akhlaghi N, Khalilak Z, Vatanpour M, Mohammadi S, Pirmoradi S, Fazlyab M, Safavi K. Root canal anatomy and morphology of mandibular first molars in a selected Iranian population: an in vitro study. Iran Endod J. 2017;12:87–91.
Mukhaimer RH. Evaluation of root canal configuration of mandibular first molars in a Palestinian population by using cone-beam computed tomography: an ex vivo study. Int Sch Res Notices. 2014;2014:583621.
Nair MK, Nair UP. Digital and advanced imaging in endodontics: a review. J Endod. 2007;33:1–6.
Navarro LF, Luzi A, Garcia AA, Garcia AH. Third canal in the mesial root of permanent mandibular first molars: review of the literature and presentation of 3 clinical reports and 2 in vitro studies. Med Oral Patol Oral Cir Bucal. 2007;12:E605–9.
Patel S, Dawood A, Ford TP, Whaites E. The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J. 2007;40:818–30.
Reyhani MF, Rahimi S, Shahi S. Root canal therapy of a mandibular first molar with five root canals: a case report. Iran Endod J. 2007;2:110–2.
Sharma P, Shekhar R, Sharma A. Endodontic management of mandibular first molar with six canals using CBCT—report of a case. J Clin Diagn Res. 2016;10:ZJ12–3.
Silva EJ, Nejaim Y, Silva AV, Haiter-Neto F, Cohenca N. Evaluation of root canal configuration of mandibular molars in a Brazilian population by using cone-beam computed tomography: an in vivo study. J Endod. 2013;39:849–52.
Song JS, Choi HJ, Jung IY, Jung HS, Kim SO. The prevalence and morphologic classification of distolingual roots in the mandibular molars in a Korean population. J Endod. 2010;36:653–7.
Song JS, Kim SO, Choi BJ, Choi HJ, Son HK, Lee JH. Incidence and relationship of an additional root in the mandibular first permanent molar and primary molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107:e56–60.
Sundaresh KJ, Srinivasan R, Mallikarjuna R, Rajalbandi S. Endodontic management of middle mesial canal of the mandibular molar. BMJ Case Rep. 2013; 2013.
Tian XM, Yang XW, Qian L, Wei B, Gong Y. Analysis of the root and canal morphologies in maxillary first and second molars in a Chinese population using cone-beam computed tomography. J Endod. 2016;42:696–701.
Tyndall DA, Rathore S. Cone-beam CT diagnostic applications: caries, periodontal bone assessment, and endodontic applications. Dent Clin N Am. 2008;52:825–41. vii
Versiani MA, Pecora JD, de Sousa-Neto MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod. 2011;37:1002–7.
Vertucci FJ, Williams RG. Root canal anatomy of the mandibular first molar. J N J Dent Assoc. 1974;45:27–28 passim.
Wang Y, Zheng QH, Zhou XD, Tang L, Wang Q, Zheng GN, Huang DM. Evaluation of the root and canal morphology of mandibular first permanent molars in a western Chinese population by cone-beam computed tomography. J Endod. 2010;36:1786–9.
Yew SC, Chan K. A retrospective study of endodontically treated mandibular first molars in a Chinese population. J Endod. 1993;19:471–3.
Zhang R, Wang H, Tian YY, Yu X, Hu T, Dummer PM. Use of cone-beam computed tomography to evaluate root and canal morphology of mandibular molars in Chinese individuals. Int Endod J. 2011;44:990–9.
Zhang R, Yang H, Yu X, Wang H, Hu T, Dummer PM. Use of CBCT to identify the morphology of maxillary permanent molar teeth in a Chinese subpopulation. Int Endod J. 2011;44:162–9.
Zheng QH, Wang Y, Zhou XD, Wang Q, Zheng GN, Huang DM. A cone-beam computed tomography study of maxillary first permanent molar root and canal morphology in a Chinese population. J Endod. 2010;36:1480–4.
Acknowledgements
We thank the patients for their support during this study.
Funding
This work was supported by the Key Scientific and Technological Project of Tianjin Health Industry (grant no. 14KG132).
Availability of data and materials
A CBCT device (J. Morita Mfg. Corp., Kyoto, Japan)
The Volume Viewer software
The Mimics software (Mimics, V 10.01, Materialise, Belgium)
The SPSS 22.0 software (IBM Corp, Armonk, NY, USA)
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
Author information
Authors and Affiliations
Contributions
NN designed the experiment. NN, SC, LH, and LKZ collected and analyzed the data. NN, SC, and JY wrote the manuscript. CFZ and NN edited and finalized the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Institutional Review Board of Tianjin Stomatological Hospital, Tianjin, China (TJSKE20160412), has approved this research, registered 12 April 2016.
Consent for publication
The procedure for the collection of imaging data (CBCT images) was explained to the patients or legal guardians, and appropriate informed consent was obtained.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Ni, N., Cao, S., Han, L. et al. Cone-beam computed tomography analysis of root canal morphology in mandibular first molars in a Chinese population: a clinical study. Evid.-based endod 3, 1 (2018). https://doi.org/10.1186/s41121-018-0015-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41121-018-0015-8