
Abstract
Background
We sought to quantify CTP-derived infarct core applying previously published perfusion thresholds to multi-institutional CTP data to assess the margin of error for 25 mL and 70 mL critical volume thresholds using early DWI as a reference standard.
Methods
60 patients with acute ischemic stroke undergoing CTP and DWI within 6 and 24 h of symptom onset, respectively, were retrospectively analyzed from 3 tertiary care centers. CTP-derived infarct core was calculated using published thresholds for absolute and relative CBF and CBV in addition to manual CBV tracing. Using DWI as the reference standard, performance of CTP-derived measures of infarct core was assessed using co-registered voxel-by-voxel analysis and total infarct volume comparison. Volumes of each CTP infarct core estimate were compared against DWI to determine the degree of infarct core over or underestimation at the critical volumes of 25 mL and 70 mL.
Results
Median core infarct volume was 10.8 mL. Mean CTP-derived infarct core volumes were similar to DWI for all CTP threshold methods to within ± 1 mL. CBV tracing demonstrated an overall significant core overestimation compared to DWI (p = 0.017). All CTP core volume estimations showed robust correlation with DWI (Pearson p-value < 0.001). As core volume increased, CTP demonstrated increased deviation from DWI. At the critical cut-offs of 25 mL and 70 mL, relative CBF demonstrated the best agreement with DWI for infarct core compared to the other CTP-derived measures of infarct core.
Conclusion
Our study demonstrates close approximation between multiple CTP-derived measures of infarct core and DWI infarct volume, Especially relative CBF.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
There is a continued interest in physiological imaging to select patients for reperfusion therapies in acute ischemic stroke (AIS) [1]. DWI is considered the reference standard for identifying permanently infarcted brain tissue while CTP is an alternative, although hotly debated surrogate [2–6]. Identification of potentially salvageable brain tissue facilitates a more personalized approach to thrombolytic therapy administration [1] and could improve outcomes beyond the traditional 4.5 h time window [7].
Infarct core volume is an increasingly important determinant in success of reperfusion therapy. A planimetrically measured core infarct volume of 70 mL is considered a critical upper limit above which poor outcome is experienced, despite high recanalization rates [8–11]. Additionally, a core infarct volume of ≤25 mL recently demonstrates very high rates of good outcomes with recanalization [12]. Accuracy of acute infarct core volume estimation is clinically important especially given recent studies demonstrating a degree infarct core volume overestimation using CTP compared to MR perfusion (MRP) and DWI within 1 h of CTP [1, 13]. There is ongoing debate over the validity of CTP to identify infarct core and while no clear consensus exists on the optimal parameter most predictive of tissue viability and outcome, CBF thresholds appear most promising [4, 5, 14–16]. Acknowledging that CTP processing methods are affected by many technical challenges such as threshold value used, type of CTP processing software and post-processing protocols [4, 5, 15, 17] a pragmatic argument could be made that the correlation between CTP and DWI core infarct determination need only be accurate enough to distinguish critical lesion volume thresholds such as 25 and 70 mL [15]. CTP utilization remains attractive because of widespread CT availability in the acute clinical setting especially in non-tertiary hospitals. We sought to quantify CTP-derived infarct core applying previously published perfusion thresholds to multi-institutional CTP data [18] to assess the margin of error for 25 mL and 70 mL critical volume thresholds using early DWI as a reference standard.
Methods
Study design and patient cohort
This retrospective study was approved by the local institutional research ethics board. Stroke patients were collected from the databases of three separate institutions between 2008 and 2010. Patients presenting with AIS who underwent NCCT and CTP within six hours of stroke symptom onset and acute DWI <24 h of presentation were included in the study. CT angiography was performed at a median of 24 ± 4 h after stroke onset to classify recanalization status.63 patients were identified. Three (3/63, 5 %) were excluded as the infarct core on DWI was beyond CTP coverage. Baseline characteristics including age, gender, NIHSS and 90-day mRS were recorded.
Scan protocol
Multicenter stroke imaging was obtained with a 64-slice CT scanner (8*5 mm), 16-slice and 64-slice scanners (single 4*5 mm acquisition or 2 contiguous acquisitions of 4*5 mm). Follow-up DWI was obtained with 1.5 T at all institutions (7000 ms/min [repetition time (TR)/echo time (TE)], field of view [FOV] of 24 cm, matrix 128*128, section thickness (ST) of 5 mm, no gap; 5000 ms/min [TR/TE], FOV of 13 cm, matrix 128*128, ST of 5 mm, 1.5 mm gap; 6000 ms/107 min [TR/TE], FOV of 40 cm, matrix 128*128/256*256, 1 mm gap). CTA angiogram was performed at baseline with parameters: aortic arch to the vertex, 0.7-mL/kg iodinated contrast agent up to a maximum of 90 mL (iohexol, Omnipaque 300 mg iodine/mL; GE Healthcare, Piscataway, New Jersey), 5- to 10- second delay, 120 kVp, 270 mA, 1 s/rotation, 1.25-mm-thick sections, and table speed of 3.7 mm/rotation. CTP was performed locally as a biphasic examination [45 s acquisition, 0.5 s intervals, 8 slices followed by 120 s acquisition, 15 s intervals, 8 slices] [19]. Other CTP acquisition were performed as 45-75 s acquisition, 1.3 s intervals, 2*2 slices and 50-70s acquisition, 1-2 s intervals [4, 20]. In all cases 40-50 mL of iodinated contrast was injected at 4–5 mL/s.
Imaging processing
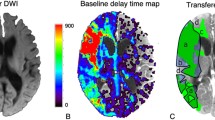
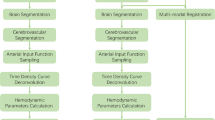
Analysis of all CTP studies was performed using CT Perfusion 4 software (GE Healthcare). Gaussian smoothing using a kernel width of 4 pixels was applied to the processed maps (Fig. 1) [1, 4]. Using Statistical Parametric Mapping (SPM8, Wellcome Trust Centre, United Kingdom), CTP and DWI maps were coregistered using tri-linear interpolation to baseline NCCT. Grey and white matter NCCT segmentation was additionally performed using SPM8.

A comparison of computed tomography perfusion (CTP) parameters. a Diffusion-weighted imaging (DWI) in identifying a right-sided infarct core. b CBV tracing, (c) absolute CBF threshold, (d) absolute CBV threshold, (e) relative CBF threshold, (f) relative CBV threshold vs. Shaded areas correspond to true-positive (green), false-positive (yellow), false-negative (purple), and true-negative (red) voxels
Imaging analysis
To identify infarct core on CTP, previously validated gray and white matter specific absolute and relative voxel-intensity thresholds (relative CBF threshold (relCBF), relative CBV threshold (relCBV), absolute CBF threshold (AbsCBF), absolute CBV threshold (AbsCBV); Table 1) were applied to CBF and CBV maps respectively with upper thresholds of <100 mL/100 g/min and <8 mL/100 g respectively to eliminate vasculature [18]. To compare visual CBV abnormality tracing compared to thresholded measures to identify infarct core an experienced neuroradiologist (XX, 10 years), blinded to DWI, manually traced areas of CBV abnormality (designated CBV tracing) using Medical Image Processing, Analysis, and Visualization (MIPAV; version: 7.0.2, National Institutes of Health, Bethesda, MD). Voxel-by-voxel comparison of the 5 generated CTP measures of infarct core was made to determine performance of each measure against the DWI reference standard utilizing MATLAB (version: 2012b, The MathWorks, Inc., Natick, MA). Finally, the volume of each CTP core estimate was compared against DWI to determine the degree of infarct core over or underestimation.
Statistical analysis
All analyses were performed using SPSS (Version 17.0. SPSS Inc., Chicago, IL). Descriptive results and quantitative baseline patient characteristics were reported as mean ± SD or median (IQR). Sensitivity and specificity were calculated for each patient for all CTP techniques and compared to DWI. Paired Student’s t-test or Wilcoxon signed-rank test compared parametric and non-parametric data respectively. Mean differences between CTP predicted infarct core and DWI infarct core volumes were compared. A correlation matrix using Pearson’s R test was performed for volumetric measures of infarct core between predicted and DWI infarct core volumes. A volumetric agreement comparison (Bland-Altman) between CTP parameters and DWI for infarct core was performed for each patient. To account for the potential of recanalization between onset and DWI, DWI/CTP differences were initially compared after dichotomizing by recanalization status. Patients were subdivided by time interval between CTP and DWI into acute (≤4 h) and subacute (>4 h) groups. A 4-h mark was chosen because this represents the upper time limit in our institution within the clinically significant therapeutic window for assessing an AIS patient while retaining sufficient time to still administer reperfusion therapy. Mean sensitivity and specificity were compared between acute and delayed group patients. Within each CTP technique, a volumetric comparison of infarct core between the acute and delayed patients was performed. Differences between predicted and actual infarct core volumes were calculated. Furthermore, patients were partitioned according to CTP scan acquisition time (<60s or ≥60s) to study the artificial reduction of CBV due to venous time density curve (TDC) truncation [15]. Lastly, cases with CTP infarct core estimation >70 mL, but DWI <70 mL (overestimation), and cases with CTP <70 mL, but DWI >70 mL (underestimation) were noted and used as a critical value for Cohen's kappa inter-modality agreement [8, 9]. The same inter-modality agreement was also assessed using a critical infarct volume of 25 mL [12]. Kappa statistics of 0.21 to 0.4, 0.41 to 0.6, 0.61 to 0.8, and 0.81 to 1 were considered fair, moderate, substantial, and nearly perfect, respectively [21]. A value of p < 0.05 was considered statistically significant.
Results
Mean patient age was 67.6 ± 13.3 and 33 % (20/60) were male. Median time from stroke symptom onset to CTP was 2.5 (IQR 1.6-3.8) hours while median time to DWI was 3.9 (IQR 1.12-15.3) hours. Recanalization occurred in 38 (63 %) of patients. Median baseline NIHSS and 90-day mRS was 16 (IQR 9–19), and 3.5 (IQR 2–5) respectively. Median core infarct volume was 10.8 mL (IQR 6.8-41.5). Figure 1 illustrates an example of the calculation of CTP performance for DWI infarct core. Mean sensitivity, specificity, and accuracy for each CTP parameter are demonstrated in Table 2. A comparison of DWI- and CTP-derived infarct core volume estimations and volumetric differences is presented in Table 3. CBV tracing demonstrated a significant core overestimation of 6.8 mL compared to DWI (p = 0.017), while CTP threshold parameters demonstrated insignificant differences (<1 mL) in comparison to DWI. All CTP core volume estimations showed robust correlation with DWI (p < 0.001). Bland-Altman plots demonstrating CTP-DWI volume difference for each CTP parameter are shown in Fig. 2. Mean volumetric 95 % confidence interval differences were: −48.7 - 48.5 mL (absCBF), −45.9 – 46.9 mL (absCBV), −44.7 – 43.2 mL (relCBF), −42.5 – 41.6 mL (relCBV), −34.5 – 48.2 mL (CBV tracing). For small (<25 mL) core volumes all CTP measures showed minimal differences in comparison to DWI. However as DWI volume increased, CTP threshold parameters tended to underestimate infarct core volume. There were no significant differences in baseline infarct core volume estimation between patients with and without recanalization.

Bland-Altman plots for all CTP parameters average volumetric agreement between CTP and DWI. a absCBF, (b) absCBV, (c) relCBF, (d) relCBV, e. CBV tracing. Solid lines demonstrate the mean difference between CTP and DWI infarct core volumes. Dotted lines represent one standard deviation above and below the mean difference
Thirty one patients underwent DWI within 4 h of CTP (acute DWI) whereas 29 received delayed DWI (>4 h). Median time to DWI after CTP for acute and delayed groups was 1.2 (IQR 0.6-2.7) hours and 15.4 (IQR 8.0-24.9) hours, respectively. There was no significant difference in time from stroke onset to initial CTP between the two groups. Mean core infarct volumes and CTP/DWI differences for the two groups are displayed in Table 4. No significant sensitivity and specificity differences when comparing early versus late DWI within each CTP technique (Table 2). Compared to early DWI only CBV tracing significantly overestimated infarct core (p = 0.039). Compared to delayed DWI no significant differences for any CTP parameter and DWI was observed. When dichotomizing patients by CTP acquisition time (<60s, n = 19 vs. ≥60s, n = 41), CBV tracing on shorter acquisition time data, trended to DWI overestimation compared to the ≥60s group (13.0 mL vs. 3.6 mL; p = 0.07).
The inter-modality agreement for 25 mL and 70 mL is presented in Table 5. rCBF threshold demonstrated the best agreement for 25 mL (κ = 0.610) while rCBV and CBV tracing showed moderate agreement. AbsCBF and AbsCBV thresholds demonstrated fair agreement. Discordance was due to a CTP overestimation of core infarct compared to DWI. Similarly for 70 mL rCBF threshold demonstrated a substantial agreement while all other CTP parameters demonstrated moderate agreement (Table 5). While CTP threshold parameters had minimal overestimation (1 case), there were 4 (7 %) cases where CTP CBV tracing overestimated infarct core at the critical volume.
Discussion
The strength of the present study is the application of previously determined thresholds from a large stroke population to data from three different stroke institutions utilizing different imaging protocols [18]. This approach undoubtedly diminishes performance for infarct volume determination compared to other studies where thresholds were optimized to study-specific patient cohorts [1, 4, 18]. Nevertheless, our results indicate close agreement with DWI volumes. rCBF demonstrates the highest agreement whereas traced CBV overestimates infarct volume particularly where scan duration is <60 s.
CBV tracing demonstrated the highest volumetric correlation to DWI, but significantly overestimate infarct core. To understand this overestimation, patients were dichotomized by length of CTP acquisition to assess the influence of truncation [15, 22]. Our results show that CTP acquisitions with acquisition times <60s overestimate infarct core due to underestimation of true CBV values. CBV underestimation due to TDC truncation is important and the need for longer CTP acquisitions that capture more of the venous phase is recently highlighted [15]. Sanelli et al. demonstrated that premature TDC cut off resulted in higher CBF and lower CBV values within the infarct core [23]. This artifact remains a significant cause of infarct volume overestimation and TDC should routinely be reviewed for adequate TDC coverage prior to CTP CBV analysis or interpretation.
An underestimation of infarct core at higher DWI volumes is attributed to the limited coverage of CTP compared to DWI with extension of infarcted tissue beyond the imaged CTP slices. This could be an important limitation of CTP if the volume approximates an upper threshold where treatment may be of no benefit, but is easily addressed by extended coverage techniques such as table toggle, tandem CTP techniques or full brain coverage with 320 slice scanners [24, 25]. Increased dose concerns may be addressed by imaging at 50 mA rather than 100mAs, nulling any increased radiation dose by halving MA and doubling spatial coverage [26]. CTP (2.5 mSV) contributes approximately 30 % of total CT Stroke protocol dose (6.1 mSv) with CTA an equal contributor (2.4 mSV). Differences between CTP and early or late DWI demonstrated significant differences only for CBV tracing. Differences reduced over time reflecting infarct evolution on later DWI offsetting the effect of baseline CBV overestimation.
Clinical importance of volume disagreement using critical thresholds demonstrated moderate to substantial intermodality agreement. Threshold selection was based on data from EXTEND, DEFUSE, and Yoo et al. [8–12]. At the critical volume of 25 mL, all CTP parameters demonstrated similar false-negative underestimation of core infarct compared to DWI. However, AbsCBF, AbsCBV, and rCBV demonstrated higher false-positive overestimation for true core infarct compared to rCBF and CBV tracing. rCBF demonstrated relatively low over- and under-estimation and the best inter-modality agreement. Using 70 mL, CBV tracing demonstrated a higher false-positive overestimation of infarct core compared to DWI than other CTP parameters. Highest agreement was demonstrated for rCBF. At both critical volumes, rCBF displayed the best agreement, reinforcing the utility of this measure for infarct core determination [4]. It is notable that this parameter has been identified as the best predictor of infarct core by a number of studies irrespective of post-processing technique or particular threshold used [4, 16, 18]. rCBF is also recently used to defined core in EXTEND-IA [11] Our results vary from a recent publication that showed larger confidence intervals for DWI versus CBF and CBV differences [27]. That study employed a non-traditional approach to CTP map by applying a threshold relative to the thalamus and not accounting for threshold differences between gray and white matter - likely contributed to their wider confidence intervals.
Limitations of this study include small sample size, due to the restrictive entry criteria, limiting the power to detect potential small differences in infarct volumes between modalities. A small percentage of our patient cohort demonstrated infarct core volumes exceeding 70 mL highlighting a limitation for this threshold, however new data suggests that a 25 mL core volume may be a better threshold. Retrospective analysis limited this study due to variation in DWI time, however the median time to DWI was approximately 1 h. CBV and DWI volumes were manually traced without testing the intra-observer agreement of this measurement. This could potentially introduce a margin of error into the measurements and their correlation with perfusion parameters. Finally, thresholds used in the current paper represent validated thresholds utilizing the image processing techniques described. We eliminated variability due to different post processing techniques by using the same pipeline for all studies. Similar results may not be obtained with other vendors’ post processing techniques.
Conclusion
In conclusion, our study demonstrates close approximation of DWI-derived infarct volume assessment with multiple CTP parameters, especially rCBF. Infarct overestimation is greatest for CBV tracing likely attributable to CBV underestimation from technical factors relating to short CTP acquisition times.
Ethical standards and patient consent
We declare that all human and animal studies have been approved by the Sunnybrook Research Institute Ethics Board and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. We declare that all patients gave informed consent prior to inclusion in this study.
References
Campbell BCV et al. Comparison of computed tomography perfusion and magnetic resonance imaging perfusion-diffusion mismatch in ischemic stroke. Stroke. 2012;43(10):2648–53.
Fiebach JB et al. CT and diffusion-weighted MR Imaging in randomized order: diffusion-weighted imaging results in higher accuracy and lower interrater variability in the diagnosis of hyperacute ischemic stroke. Stroke. 2002;33(9):2206–10.
Campbell BCV et al. The infarct core is well represented by the acute diffusion lesion: sustained reversal is infrequent. J Cereb Blood Flow Metab. 2012;32(1):50–6.
Campbell BCV et al. Cerebral blood flow is the optimal CT perfusion parameter for assessing infarct core. Stroke. 2011;42(12):3435–40.
Kamalian S et al. CT cerebral blood flow maps optimally correlate with admission diffusion-weighted imaging in acute stroke but thresholds vary by postprocessing platform. Stroke. 2011;42(7):1923–8.
Young KC, Benesch CG, Jahromi BS. Cost-effectiveness of multimodal CT for evaluating acute stroke. Neurology. 2010;75(19):1678–85.
Picanço MR et al. Reperfusion after 4 · 5 hours reduces infarct growth and improves clinical outcomes. Int J Stroke. 2014;9(3):266–9.
Campbell BCV et al. A multicenter, randomized, controlled study to investigate EXtending the time for Thrombolysis in Emergency Neurological Deficits with Intra-Arterial therapy (EXTEND-IA). Int J Stroke. 2014;9(1):126–32.
Lansberg MG et al. MRI profile and response to endovascular reperfusion after stroke (DEFUSE 2): a prospective cohort study. Lancet Neurol. 2012;11(10):860–7.
Yoo AJ et al. MRI-based selection for intra-arterial stroke therapy: value of pretreatment diffusion-weighted imaging lesion volume in selecting patients with acute stroke who will benefit from early recanalization. Stroke. 2009;40(6):2046–54.
Campbell BC et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015;372(11):1009–18.
Parsons MW et al. Pretreatment diffusion- and perfusion-MR lesion volumes have a crucial influence on clinical response to stroke thrombolysis. J Cereb Blood Flow Metab. 2010;30(6):1214–25.
Lin L et al. Comparison of computed tomographic and magnetic resonance perfusion measurements in acute ischemic stroke: back-to-back quantitative analysis. Stroke. 2014;45(6):1727–32.
Bivard A et al. Defining the extent of irreversible brain ischemia using perfusion computed tomography. Cerebrovasc Dis. 2011;31(3):238–45.
Lev MH. Acute stroke imaging: what is sufficient for triage to endovascular therapies? Am J Neuroradiol. 2012;33(5):790–2.
Wintermark M et al. Imaging recommendations for acute stroke and transient ischemic attack patients: a joint statement by the American Society of Neuroradiology, the American College of Radiology, and the Society of Neurointerventional Surgery. Am J Neuroradiol. 2013;34(11):E117–27.
Fahmi F et al. Differences in CT perfusion summary maps for patients with acute ischemic stroke generated by 2 software packages. Am J Neuroradiol. 2012;33(11):2074–80.
Eilaghi A et al. Toward patient-tailored perfusion thresholds for prediction of stroke outcome. Am J Neuroradiol. 2014;35(3):472–7.
Aviv RI et al. Hemorrhagic transformation of ischemic stroke: prediction with CT perfusion. Radiology. 2009;250(3):867–77.
Zhu G et al. Computed tomography workup of patients suspected of acute ischemic stroke: perfusion computed tomography adds value compared with clinical evaluation, noncontrast computed tomography, and computed tomography angiogram in terms of predicting outcome. Stroke. 2013;44(4):1049–55.
Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–74.
Lev MH. Perfusion imaging of acute stroke: its role in current and future clinical practice. Radiology. 2013;266(1):22–7.
Sanelli PC et al. The effect of varying user-selected input parameters on quantitative values in CT perfusion maps1. Acad Radiol. 2004;11(10):1085–92.
Roberts HC et al. Multisection dynamic CT perfusion for acute cerebral ischemia: the “toggling-table” technique. Am J Neuroradiol. 2001;22(6):1077–80.
Wintermark M et al. Dynamic perfusion CT: optimizing the temporal resolution and contrast volume for calculation of perfusion ct parameters in stroke patients. Am J Neuroradiol. 2004;25(5):720–9.
Murphy A et al. Low dose CT perfusion in acute ischemic stroke. Neuroradiology. 2014;56(12):1055–62.
Schaefer PW et al. Limited reliability of computed tomographic perfusion acute infarct volume measurements compared with diffusion-weighted imaging in anterior circulation stroke. Stroke. 2015;46(2):419–24.
Disclosures/grant support
AV received funding support from Imaging Core Lab, PRISMS Trial, Genentech, Inc.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
DCH: Literature review, Project development, Data collection, Image processing, Data analysis, Manuscript writing. MWP: Literature review, Project development, Data collection, Manuscript review. MW: Literature review, Project development, Data collection, Manuscript review. AV: Data collection, Manuscript review. CDd’E: Project development, Manuscript review. RV: Data collection, Data analysis, Manuscript review. DE: Image processing, Data analysis, Manuscript review. JK: Image processing, Data analysis, Manuscript review. TJH: Data analysis, Manuscript review. AB: Data collection, Manuscript review. SS: Project development, Manuscript review. RIA: Literature review, Project development, Data collection, Manuscript writing, Manuscript review. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Huynh, D.C., Parsons, M.W., Wintermark, M. et al. Can CT perfusion accurately assess infarct core?. Neurovasc Imaging 2, 7 (2016). https://doi.org/10.1186/s40809-016-0018-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40809-016-0018-1