
Abstract
Background
Walking and running provide cyclical loading to the knee which is thought essential for joint health within a physiological window. However, exercising outside the physiological window, e.g. excessive cyclical loading, may produce loading conditions that could be detrimental to joint health and lead to injury and, ultimately, osteoarthritis. The purpose of this study was to assess the effects of a stepwise increase in speed and duration of treadmill training on knee joint integrity and to identify the potential threshold for joint damage.
Methods
Twenty-four Sprague-Dawley rats were randomized into four groups: no exercise, moderate duration, high duration, and extra high duration treadmill exercise. The treadmill training consisted of a 12-week progressive program. Following the intervention period, histologic serial sections of the left knee were graded using a modified Mankin Histology Scoring System. Mechanical testing of the tibial plateau cartilage and RT-qPCR analysis of mRNA from the fat pad, patellar tendon, and synovium were performed for the right knee. Kruskal-Wallis testing was used to assess differences between groups for all variables.
Results
There were no differences in cartilage integrity or mechanical properties between groups and no differences in mRNA from the fat pad and patellar tendon. However, COX-2 mRNA levels in the synovium were lower for all animals in the exercise intervention groups compared to those in the no exercise group.
Conclusions
Therefore, these exercise protocols did not exceed the joint physiological window and can likely be used safely in aerobic exercise intervention studies without affecting knee joint health.
Similar content being viewed by others

Key Points
-
A stepwise increase in the speed and duration of exercise did not lead to osteoarthritis-like changes in the knee.
-
Chronic exercise appeared to produce a protective effect on the knee.
-
Working within an optimal physiological exercise window is beneficial for joint health across the life span.
Background
Exercise has been used to promote health and fitness as far back as 2500 BC [1]. However, in the past years, exercise has been postulated to act like a drug [2] and, as such, provides advantages and risks to an individual’s health and fitness. Specifically, aerobic exercise has been shown to lead to increased bone mineral density, insulin sensitivity, high-density lipoprotein cholesterol levels, resting and maximal stroke volume, maximal oxygen uptake, and basal metabolism [3, 4]. Exercise has also been shown to reduce body fat, fasting blood insulin levels, low-density lipoprotein cholesterol levels, resting heart rate, and systolic and diastolic blood pressure [3, 4]. However, the effects of exercise on joint health remain controversial [5,6,7,8].
In a prospective survey, aimed at examining the relationship of self-reported physical activity and physician-diagnosed osteoarthritis (OA) from 1970 to 1995, a positive association between OA incidence and physical activity was found. Running was suggested to lead to an increased risk for developing OA in some studies [8], but not in others [5,6,7]. Chakravarty et al. [5] did not find an increased risk for knee OA in masters runners compared to controls over an 18-year period [5], and Miller et al. [7] suggested that running does not increase the risk for knee OA compared to walking. However, Cheng et al. [8] reported a positive association between running more than 32 km per week and clinician-diagnosed knee OA.
If exercise is thought to act like a drug preventing joint disease, the dosage may be critical to its success. It has been shown that moderate exercise, such as walking and running, exerts added loading to the knee joint, and cyclical loading is thought to be vital for maintaining cartilage integrity/homeostasis and healthy joints [9,10,11]. In contrast, in vivo and vitro studies with excessive repetitive joint loading have been implicated with the development of OA [12, 13]. Joints are thought to be designed to operate within a “physiological window” to maintain proper function and allow for positive adaptations [12]. Loading outside this window may put the joint, and specifically the cartilage, at risk for degeneration [14, 15].
In rodent model of exercise, for example, Galois et al. [16] suggested that different levels of treadmill training may have different influences on the severity of chondral lesions in anterior cruciate ligament transection (ACLT) model of osteoarthritis in Wistar rats; while slight to moderate levels seemed to be beneficial to the knee cartilage health, more strenuous exercise may be detrimental. Controversially, Yang et al. [17] showed that treadmill exercise up to 1 h per day, 5 days a week, for 8 weeks, in Sprague-Dawley rat model of monosodium iodoacetate-induced OA, has a chondroprotective effect, and this effect was more prominent in rats that fulfill in three times per day the 1 h treadmill exercise, suggesting that an adaptive phase training may be an important factor in protecting the knee joint from OA-like changes.
Wistar rats, without previous lesion in the knee, have also been randomly assigned to a sedentary control group, a low-intensity running, a medium-intensity running, and a high-intensity running [18]. As a result, rats in the high-intensity running demonstrated OA-like changes in their knees, while rats in the other running groups did not. Moreover, in a study in rodent models where the animals were allowed minimum [19] or not allowed an adaptive phase [18], they have demonstrated OA-like changes in their knees. However, it is unknown how much exercise is too little or too much. Therefore, the purpose of this study was to determine the effects of a stepwise increase in speed and duration of treadmill training on knee joint integrity and to identify the potential treadmill training threshold for the development of joint damage in the rat knee. We hypothesized that excessive chronic treadmill training leads to the development of OA-like changes in the knee, while moderate levels of treadmill training maintain cartilage integrity and induce positive adaptive responses. The key outcome measures were joint integrity, body composition, gene expression patterns, and blood-based and synovial fluid-based biomarkers.
Methods
The aim of this study was to determine the effects of a stepwise increase in speed and duration of treadmill training on knee joint integrity and to identify the potential treadmill training threshold for the development of joint damage in the rat knee.
Animals
Twenty-four 10- to 14-week-old male Sprague-Dawley rats were housed individually and randomized into four groups: moderate duration exercise (MD, n = 6), high duration exercise (HD, n = 6), extra high duration exercise (EHD, n = 6), or no exercise (control, n = 6). Rats were fed (ad libitum) a standard chow diet (Diet #5001, Lab Diet, USA). A minimum sample size of five rats per group is based on the ability to detect a minimal meaningful difference in histological scoring of the knee joint to provide an α = 0.05 and a power of 80%. Calculation of sample size was performed using G*Power Software (version 3.0.10, Germany) [20]. Data for sample size calculations were obtained from a previous study [21]. All experiments were approved by the University of Calgary Life and Environmental Sciences Animal Care Committee, and all methods were conducted in accordance with the animal welfare regulations and guidelines at the University of Calgary.
Exercise Training Protocol
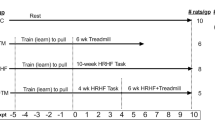
Following 1 week of acclimatization to the housing environment, rats were exposed to their respective exercise programs (see Table 1 for details of the exercise programs) on a Columbus Instruments Exer-3R treadmill (Columbus, OH, USA) for 12 weeks. The moderate duration group progressively built up to 30 min of treadmill training each day, five times per week at 25 m/min. The high duration group built up to 60 min of treadmill training per day for 5 days per week at 25 m/min. Rats in the extra high duration protocol reached 60-min training sessions 7 days per week at 25 m/min. In weeks 10, 11, and 12, these rats trained twice, three times, and four times for 1 h daily, respectively. This last training intervention has previously been used to elicit overtraining in Wistar rats [22]. Animals in the control group were placed on the treadmill 5 days a week and completed 15 min of exercise at 10 m/min once per week. This was done to account for the stress of handling and avoiding confound results. A shock grid at the back of the treadmill was used to prevent animals from falling behind the pace of the treadmill.
Body Composition
Body mass was measured at the beginning of each week. Body mass for each animal was normalized to that of week 1 (familiarization week) and was expressed as the percent increase in body mass from that initial value. One week after completing the 12-week training protocol, and immediately prior to sacrifice, rats were lightly anesthetized with isoflurane and body composition was measured using dual X-ray absorptiometry (DXA) with software for small animals (Hologic ODR 4500; Hologic, MA, USA). An average of three scans for each animal was used for analysis.
Blood Analysis
Following 12 h of fasting, rats were anesthetized with isoflurane and a blood sample was collected by cardiac puncture. Blood was centrifuged at 3000 rpm for 15 min at 4 °C and serum stored in aliquots at − 80 °C until analyzed. Rats were sacrificed by heart excision. Serum cytokines and adipokines were quantified using a Rat 27 Multiplex Discovery Assay with Luminex® xMAP technology (eotaxin, EGF, fractalkine, IL-1α, IL-1β, IL-2, IL-4, IL-5, IL-6, IL-10, IL-12(p70), IL-13, IL-17A, IL-18, IP-10/CXCL10, GRO/KC, IFN-γ, TNF-α, G-CSF, GM-CSF, MCP-1, leptin, LIX, MIP-1α, MIP-2, RANTES, VEGF; Eve Technologies, Calgary, AB, Canada).
Knee Joints
Knee joints were collected from both hind limbs. The left knee was harvested by cutting the femur and tibia/fibula 2 cm above and below the joint line. Excess muscles were removed, and joints were fixed in a 10% neutral buffered formalin solution (Thermo Fisher Scientific, MA, USA) for 14 days at room temperature. Knees were then decalcified at room temperature, using Cal-Ex II solution (10% formic acid in formaldehyde, Thermo Fisher Scientific). The decalcification solution was changed daily. The end of decalcification was determined by chemical testing with a 5% ammonium oxalate solution (Thermo Fisher Scientific) until no precipitate was detected for 5 days (on average 21 days). Samples were then processed using an automatic paraffin processor (Leica TP 1020, Leica Microsystems Inc., Concord, Ontario, Canada). They were dehydrated in a graded series of alcohols, cleared in xylene, and infiltrated with 50% Paraplast X-TRA® wax (Thermo Fisher Scientific) and 50% Paraplast Plus® wax (Thermo Fisher Scientific). Further, the left knee joints were embedded in paraffin wax and stored at room temperature until sectioning. Serial, sagittal plane sections of 10-μm thickness were obtained using a Leica RM 2165 microtome (Leica Biosystems, Nussloch, Germany). Sections were mounted onto Super Frost plus slides (Thermo Fisher Scientific) and allowed to dry at 40 °C for 7 days. Alternate slides were stained sequentially with hematoxylin, fast green, and safranin-O (Thermo Fisher Scientific) using an auto stainer (Leica ST 5010, Leica Biosystems). Sections were then dehydrated in a graded series of alcohols, cleared in xylene, and mounted with Cytoseal 60 mounting media (Thermo Fisher Scientific) using an auto cover slipper (Leica CV 5030, Leica Biosystems). Slides were dried at room temperature for 7 days before being evaluated using a light microscope (Zeiss Axiostar plus, Carl Zeiss Inc., Ontario, Canada). Two independent graders scored all histological sections in a blinded manner using a modified Mankin Histology Scoring System [23]. Osteoarthritis Research Society International (OARSI) histologic [24] subscores for bone changes, synovial thickening, and meniscus were also determined for each joint. The total modified Mankin score for each animal represents the sum of all Mankin scores and OARSI subscores. Tibial and femoral cartilage thickness were determined from histological slides.
The right knee joints were opened to collect the synovium, menisci, fat pad, and patellar tendon. The tissues were snap-frozen in liquid nitrogen and stored at − 80 °C for RNA isolation and subsequent RT-qPCR analysis. Genes analyzed for the patellar tendon and synovium were Col-1, Col-3, iNOS, COX-2, IGF-1, IL-1, IL-6, and TGF-β. Genes analyzed for the fat pad were iNOS, PPAR-γ, COX-2, IL-1B, IP-10, leptin, TF, TFPI, and VEGF. Genes analyzed for the menisci were Col-1, Col-3, iNOS, PPAR-γ, COX-2, IGF-1, IL-1, IL-6, TGF-β, IP-10, leptin, TF, TFPI, VEGF, and PRG4 (see Table 2 for details). Synovial fluid was also collected from the right knee shortly after sacrifice using the Whatman chromatography paper method [25]. Samples were weighed, diluted 1:50, and stored at 4 °C overnight. After 24 h, samples were centrifuged and stored at − 80 °C until analysis. Synovial fluid cytokines and adipokines were quantified using a Rat 27 Multiplex Discovery Assay with Luminex® xMAP technology (eotaxin, EGF, fractalkine, IL-1α, IL-1β, IL-2, IL-4, IL-5, IL-6, IL-10, IL-12(p70), IL-13, IL-17A, IL-18, IP-10/CXCL10, GRO/KC, IFN-γ, TNF-α, G-CSF, GM-CSF, MCP-1, leptin, LIX, MIP-1α, MIP-2, RANTES, VEGF; Eve Technologies).
The right tibia was stored at − 20 °C until assessment of the biomechanical properties of cartilage was performed. A spherical indenter (r = 175 ± 2.5 μm) made of a stainless steel 316 L shaft and a spherical glass bead was installed under the multiaxial load cell (force resolution: Fz = 3.5 mN and Fx = Fy = 2.5 mN) of a three-axis mechanical tester (Mach-1 v500css, Biomomentum, QC, Canada). The tibia was fixed in a sample holder using dental cement. The sample was then immersed into a testing chamber that contained PBS and was equipped with a camera registration system (Biomomentum). A position grid was superimposed on the image of the tibia articular surface for a mechanically controlled surface mapping [26]. Stress relaxation tests for cartilage properties were performed on 11 sites each for the medial and lateral tibial plateau using the automated mapping system, and Young’s modulus were calculated for each test site.
Statistical Analysis
Non-parametric Kruskal-Wallis testing was used to determine differences between the four animal groups for all variables (RT-qPCR analyses, body fat, body mass, cartilage thickness, Mankin/OARSI score, equilibrium Young’s modulus, and protein assays). If significant (p < 0.05), post hoc testing using the Mann-Whitney U test was used to indicate differences between groups. Further, estimates of effect size were calculated using the ANOVA univariate approach on SPSS (version 22). Partial eta squared (partial η2) were reported to provide small (partial η2 = 0.01), medium (partial η2 = 0.06), and large (partial η2 = 0.14) effects [27].
Results
Training Distances
Rats in the control group traveled a distance of 150 m per week from week 2 to week 12, with a total distance of 1.65 km at the end of the experimental protocol. Rats in the MD and HD groups had a gradual increase in speed and duration from week 2 to week 5 (4 weeks of adaptation), and then, they ran in a constant speed and duration from week 6 to week 12, leading to a total distance traveled of 37.9 and 69.9 km, respectively (Fig. 1, Table 1). Rats in the EHD group have a stepwise increase in distance traveled from week 2 to week 5, then a constant distance traveled from week 6 to week 9, and another stepwise increase in distance traveled from week 10 to week 12, leading to a total distance traveled of 162.8 km by the end of the exercise protocol.

a Travel distance per week per group. Notice, the control group was exposed to a constant amount of exercise throughout the protocol, 150 m per week. For the other groups, there was a gradual increase in the amount of exercise from week 2 to week 5. From week 5 to the end of the intervention period, the levels of exercise were constant for rats in the MD and HD groups. For rats on the EHD group, the exercise distance doubled, tripled, and quadrupled in weeks 10, 11, and 12 compared to weeks 5–9, respectively. b Body fat. % body fat measured in the end of the experimental protocol. c Total modified Mankin scores: No significant differences were found between groups. MD moderate duration exercise, HD high duration exercise, EHD extra high duration exercise. * indicates significant difference when compared to control group. # indicates significant difference when compared to moderate duration group
Body Composition
Rats in all groups exhibited a gradual increase in body mass during the intervention period. However, body fat was significantly reduced by 4.5% (p = 0.046), 6.9% (p = 0.032), and 9.4% (p = 0.003) in the MD, HD, and EHD group rats, respectively, compared to that in the control group rats at the end of the exercise intervention period. Body fat was also significantly reduced by 4.9% (p = 0.025) in the EHD rats compared to that in the MD group rats (Fig. 1b, Table 3).
Knee Joint Integrity and Inflammatory Markers
There were no differences in cartilage integrity (Fig. 1c, Table 3), mechanical properties, and cartilage thicknesses (Fig. 2a, Table 3) between groups across all joint locations. There were also no differences between groups in gene expression levels for the fat pad, patellar tendon, and menisci. Cyclooxygenase 2 (COX-2) levels in the synovium were lower for the three exercise group animals than those in the control group animals (p = 0.010) (Fig. 2b). Epidermal growth factor (EGF) levels in the synovial fluid were significantly greater in EHD and HD group animals than those obtained in the control group animals (p = 0.039, p = 0.014, respectively; Table 4, Fig. 2c). Serum interleukin-12 (IL-12) levels were significantly higher for the EHD group animals than for the control (p = 0.015) group and the HD (p = 0.008) group animals (Table 4).

a Cartilage thicknesses across six sites on the knee joint measured through histology. No significant differences were found between groups. b COX-2 mRNA levels for the synovium expressed as fold change from control group (dashed gray line). c EGF exhibiting significant differences between groups for synovial fluid; 27 proteins were analyzed with a Luminex-based protein assay. MD moderate duration exercise, HD high duration exercise, EHD extra high duration exercise, MFC-ant anterior medial femoral condyle, MFC-post posterior medial femoral condyle, LFC-ant anterior lateral femoral condyle, LFC-post posterior lateral femoral condyle. * indicates a significant difference when compared to control group values
Discussion
Inactivity is the fourth leading risk factor for global mortality [28]. A physically inactive lifestyle is associated with the development of non-communicable diseases [29], including OA [30]. In contrast, exercise is reported to be a strong factor in health promotion and the prevention or delay of many non-communicable diseases [29]. However, poor health outcomes have been reported in athletes exposed to extra high levels of exercise [31, 32], and it has been reported that top-level athletes have an increased risk of developing knee OA [33]. Consequently, exercise can be beneficial or detrimental to the general health. Mechanical loading of joints due to exercise may be minimal but sufficient to maintain tissue homeostasis, it may be within the optimal physiological window and help maintain tissue homeostasis and produce positive tissue adaptations, or it may be strenuous, thus exceeding the physiological window and lead to disruptions of tissue homeostasis, leading to joint disease. In this study, we investigated the effects of a stepwise increase in speed and duration of treadmill training on knee joint health in Sprague-Dawley rats.
We randomized 24 male Sprague-Dawley rats into four groups: moderate duration exercise (MD), high duration exercise (HD), extra high duration exercise (EHD), or no exercise (control). We did not detect changes in cartilage structure, mechanical properties, or thickness between groups and across joint locations. Therefore, the speed and duration of even the most strenuous treadmill exercise protocol used here (up to 4 h of exercise daily) was not detrimental to the knee joint cartilage in these animals. Thus, the load applied to the knee through the exercise intervention protocol provided here was likely within the physiologic loading window that has been suggested to allow for adaptation, remodeling, and proper functioning of cells and tissues [9,10,11,12, 15].
An aggressive endurance exercise protocol in 16- to 18-week-old Wistar rats has been shown to lead to OA-like changes in the knee [19]. These rats were allowed 1 week of familiarization to the exercise protocol, followed by exercising twice a day, 5 days per week, for 3 and 6 weeks, for a total of 30 and 55 km of distance traveled [19]. In our study, rats were allowed a prolonged adaptation period and were introduced gradually to the increasing speed and duration of the exercise protocol, a factor which may be critical for joint health outcomes. The gradual increase in speed and duration of the exercise sessions may have allowed the cartilage to adjust gradually to the increasing load requirements, operating within the physiological window. The adaptive training phase in our study consisted of 4 weeks, and has been suggested to trigger increases in fitness and health in Wistar rats [22], and may be an important factor in the protection of the knee joint. It has been shown that a gradual increase in running volume in Wistar rats results in bone and cartilage remodeling by reducing catabolic genes and increasing aggrecan expression [34]. However, to our knowledge, there is no study systematically investigating adaptive training phase in order to protect the knee joint, and this is a limitation of our study. Additionally, in the present study, rats in the EHD group doubled, tripled, and quadrupled the amount of exercise in weeks 10, 11, and 12, respectively, relative to weeks 5–9. If these levels of exercise were sustained for an extended period, they may cause damage to the knee. Additionally, the physiological window for knee health is thought to be highly individual and may be influenced by genetics, sex, lifetime loading history, presence of prior injury/scar tissue, systemic pathology, and local anatomy [15].
Rats from all groups exhibited a gradual increase in body mass during the exercise intervention period. This increase was consistent with the expected increase in body mass of laboratory rats with age [35]. However, the MD, HD, and EHD group rats were leaner than the control group rats, and the EHD group rats were leaner than the MD group rats at the end of the intervention period. Body fat has been shown to decrease with aerobic exercise in humans [36] and mice [37]. Since body fat was reduced in the exercise group animals, but body weight was similar across all groups, the lean body mass (muscle mass) must have increased in the exercise group animals compared to that in the control group animals (not evaluated in our study). Results similar to ours have been reported for human studies where strength and endurance exercise did not produce differences in body mass but resulted in a reduction in body fat for individuals in an exercise program compared to individuals in a non-exercising group [38]. A reduction in body fat is considered a positive outcome for overall health and has been shown to reduce risks for diabetes, cardiovascular disease, metabolic syndrome, and knee OA [39,40,41,42].
Exercise induces multiple biochemical changes that may affect gene expression [43, 44]. In the present study, markers for oxidative stress (iNOS), collagen (Col-I and Col-III), pro-inflammation (IL-1β, COX-2, IL-6, leptin, IGF-1, IP-10), and anti-inflammation (TF, TFPI, VEGGF, TGF-β) were evaluated for the knee joint tissues. Gene expression in the fat pad, patellar tendon, and menisci were similar across all groups. However, COX-2 mRNA levels in the synovium were reduced for all animals in exercise groups compared to those in the animals in the control group. A reduction in COX-2 expression is thought to be positive for the joint environment, since drugs that inhibit COX-2 have been associated with a reduction of OA-like histological changes and suppressed chondrocyte apoptosis [45, 46]. Indeed, it has been demonstrated that exercise is a robust approach to preserve healthy cartilage [47]. Specifically, low intensity treadmill walking for 2, 5, or 15 days has been demonstrated to regulate metabolic responses at the cellular and systemic level, protecting cartilage against OA by altering gene expression of markers involved in OA onset [47]. Our findings indicate that all levels of exercise used in our study led to a reduction in COX-2 mRNA in the synovium, suggesting a potential protective effect of exercise for the knee, even in the lowest end highest exercise programs. It is important to highlight that at the end of the 12-week treadmill training, many molecular changes may have occurred to adapt to the new loading conditions and had already plateaued and normalized to the new exercise threshold by the time tissue was taken. Additionally, we did not study the protein and activity levels; this needs to be done in future studies.
Synovial fluid EGF levels were significantly higher in the EHD and HD group animals than those in the control group animals. It has been suggested that EGF is produced by the synovium in the initial stages of rheumatoid arthritis [48] and that activation of EGF receptor signaling may be a causal factor in OA [49, 50]. However, more recent studies indicated anabolic effects of EGF receptor signal activation in articular cartilage, suggesting that EGF may promote the expansion and/or activity of an endogenous EGF receptor responsive cell population within the articular cartilage [51]. Moreover, the EGF receptor is an important signaling molecule in bone development and remodeling and plays an anabolic role in bone metabolism [52]. Overall, the finding of elevated synovial fluid EGF levels in the EHD and HD group animals in the absence of OA-like changes suggests that EGF was not detrimental to knee joint health.
Serum IL-12 levels were significantly higher for the EHD group compared to those for the control group and HD group rats. This result agrees with the findings from in vitro studies. Exercise has been reported to increase IL-12 production by macrophages following lipopolysaccharide stimulation [53]. IL-12 is believed to be essential for the clearance of bacterial infections [54] and is thought to be an important pathogenetic factor in Th1-type-mediated autoimmune disease. IL-12-deficient mice have been found to be resistant to collagen-induced inflammatory arthritis [55], while transgenic over-expression of IL-12 exacerbates the course of this disease [56]. However, the role of IL-12 in maintaining knee joint integrity, and its role in the pathogenesis of osteoarthritis, is poorly understood. It should be noted that the over-expression of serum IL-12 may represent responses to exercise unrelated to the knee joint, as serum may represent input from a number of sources, i.e. muscle and vasculature. However, in combination with the other findings in our study, IL-12 may be playing a protective role for knee joint cartilage. Further mechanistic studies are required to elucidate the role of IL-12 in this model of exercise-induced changes in knee joint health, as well as follow the EHD rats for longer period of time than the 12 weeks of this protocol.
Conclusions
In summary, a stepwise increase in the speed and duration of a 12-week chronic treadmill exercise program did not lead to OA-like changes in the rat knee but appeared to produce a potential protective effect through a reduction in COX-2 mRNA levels in the synovium. Further studies aimed at elucidating the preventive and potentially harmful effects of repetitive chronic exercise need to be performed to better understand the effects of joint loading on joint health above or below the physiological window. Working within an optimal physiological exercise window is beneficial for general and for joint health across the life span. It is also important in the context of recreational and elite sports, where the optimal window may be altered following joint injury or disease and may thus affect the return to sport.
Abbreviations
- BC:
-
Before Christ
- Col-1:
-
Type I collagen
- Col-3:
-
Type II collagen
- COX-2:
-
Cyclooxygenase-2
- DXA:
-
Dual X-ray absorptiometry
- EGF:
-
Epidermal growth factor
- EHD:
-
Extra high duration
- G-CSF:
-
Granulocyte colony-stimulating factor
- GM-CSF:
-
Granulocyte macrophage colony-stimulating factor
- GRO/KC:
-
CXCL1 chemokine, growth-related oncogene keratinocyte chemoattractant
- HD:
-
High duration
- IFN-γ:
-
Interferon gamma
- IGF-1:
-
Insulin-like growth factor 1
- IL:
-
Interleukin
- iNOS:
-
Inducible nitric oxide synthase
- IP-10/CXCL10:
-
Interferon gamma-induced protein 10
- LIX:
-
CXCL5 chemokine
- MCP-1:
-
Macrophage chemoattractant protein-1
- MD:
-
Moderate duration
- MIP:
-
Macrophage inflammatory protein
- mRNA:
-
Messenger ribonucleic acid
- OA:
-
Osteoarthritis
- OARSI:
-
Osteoarthritis Society International (Histology Scoring System)
- PPAR-γ:
-
Peroxisome proliferator-activated receptor gamma
- RANTES:
-
Regulated on activation, normal T cell expressed and secreted
- RNA:
-
Ribonucleic acid
- RT-qPCR:
-
Real-time quantitative polymerase chain reaction
- TF:
-
Tissue factor
- TFPI:
-
Tissue factor pathway inhibitor
- TGF-β:
-
Transforming growth factor-beta
- Th1:
-
Type 1 T helper cells
- TNF-α:
-
Tumor necrosis factor alpha
- VEGF:
-
Vascular endothelial growth factor
References
Albert SL, Petrucelli RJ. Medicine: an illustrated history: Abradale Press/Abrams; 1978.
Vina J, Sanchis-Gomar F, Martinez-Bello V, Gomez-Cabrera MC. Exercise acts as a drug; the pharmacological benefits of exercise. Br J Pharmacol. 2012;167(1):1–12.
Pollock ML, Evans WJ. Resistance training for health and disease: introduction. Med Sci Sports Exerc. 1999;31(1):10–1.
Bassi D, Mendes RG, Arakelian VM, Caruso FC, Cabiddu R, Junior JC, et al. Potential effects on cardiorespiratory and metabolic status after a concurrent strength and endurance training program in diabetes patients—a randomized controlled trial. Sports Med Open. 2015;2:31.
Chakravarty EF, Hubert HB, Lingala VB, Zatarain E, Fries JF. Long distance running and knee osteoarthritis. A prospective study. Am J Prev Med. 2008;35(2):133–8.
Lane NE, Oehlert JW, Bloch DA, Fries JF. The relationship of running to osteoarthritis of the knee and hip and bone mineral density of the lumbar spine: a 9 year longitudinal study. J Rheumatol. 1998;25(2):334–41.
Miller RH, Edwards WB, Brandon SC, Morton AM, Deluzio KJ. Why don’t most runners get knee osteoarthritis? A case for per-unit-distance loads. Med Sci Sports Exerc. 2014;46(3):572–9.
Cheng Y, Macera CA, Davis DR, Ainsworth BE, Troped PJ, Blair SN. Physical activity and self-reported, physician-diagnosed osteoarthritis: is physical activity a risk factor? J Clin Epidemiol. 2000;53(3):315–22.
Eckstein F, Hudelmaier M, Putz R. The effects of exercise on human articular cartilage. J Anat. 2006;208(4):491–512.
Maly MR, Robbins SM. Osteoarthritis year in review 2014: rehabilitation and outcomes. Osteoarthr Cartil. 2014;22(12):1958–88.
Hunter DJ, Beavers DP, Eckstein F, Guermazi A, Loeser RF, Nicklas BJ, et al. The Intensive Diet and Exercise for Arthritis (IDEA) trial: 18-month radiographic and MRI outcomes. Osteoarthr Cartil. 2015;23(7):1090–8.
Hart DA, Frank CB, Bray RC. Inflammatory process in repetitive motion and overuse syndromes: potential role of neurogenic mechanisms in tendons and ligaments. In: Gordon SL, Blair SJ, Fine LJ, editors. Repetitive motion disorders of the upper extremity. Rosemont, IL: American Academy of Orthopaedic Surgeons; 1995. p. 247–65.
Madden RM, Han SK, Herzog W. The effect of compressive loading magnitude on in situ chondrocyte calcium signaling. Biomech Model Mechanobiol. 2015;14(1):135–42.
Natsu-Ume T, Majima T, Reno C, Shrive NG, Frank CB, Hart DA. Menisci of the rabbit knee require mechanical loading to maintain homeostasis: cyclic hydrostatic compression in vitro prevents derepression of catabolic genes. J Orthop Sci. 2005;10(4):396–405.
Hart DA, Scott A. Getting the dose right when prescribing exercise for connective tissue conditions: the Yin [corrected] and the Yang of tissue homeostasis. Br J Sports Med. 2012;46(10):696–8.
Galois L, Etienne S, Grossin L, Watrin-Pinzano A, Cournil-Henrionnet C, Loeuille D, et al. Dose-response relationship for exercise on severity of experimental osteoarthritis in rats: a pilot study. Osteoarthr Cartil. 2004;12(10):779–86.
Yang Y, Wang Y, Kong Y, Zhang X, Bai L. The effects of different frequency treadmill exercise on lipoxin A4 and articular cartilage degeneration in an experimental model of monosodium iodoacetate-induced osteoarthritis in rats. PLoS One. 2017;12(6):e0179162.
Ni GX, Liu SY, Lei L, Li Z, Zhou YZ, Zhan LQ. Intensity-dependent effect of treadmill running on knee articular cartilage in a rat model. Biomed Res Int. 2013;2013:172392.
Beckett J, Jin W, Schultz M, Chen A, Tolbert D, Moed BR, et al. Excessive running induces cartilage degeneration in knee joints and alters gait of rats. J Orthop Res. 2012;30(10):1604–10.
Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–91.
Collins KH, Reimer RA, Seerattan RA, Leonard TR, Herzog W. Using diet-induced obesity to understand a metabolic subtype of osteoarthritis in rats. Osteoarthr Cartil. 2015;23(6):957–65.
Hohl R, Ferraresso RL, De Oliveira RB, Lucco R, Brenzikofer R, De Macedo DV. Development and characterization of an overtraining animal model. Med Sci Sports Exerc. 2009;41(5):1155–63.
Mankin HJ, Dorfman H, Lippiello L, Zarins A. Biochemical and metabolic abnormalities in articular cartilage from osteo-arthritic human hips. II. Correlation of morphology with biochemical and metabolic data. J Bone Joint Surg Am. 1971;53(3):523–37.
Gerwin N, Bendele AM, Glasson S, Carlson CS. The OARSI histopathology initiative—recommendations for histological assessments of osteoarthritis in the rat. Osteoarthr Cartil. 2010;18(Suppl 3):S24–34.
Seifer DR, Furman BD, Guilak F, Olson SA, Brooks SC 3rd, Kraus VB. Novel synovial fluid recovery method allows for quantification of a marker of arthritis in mice. Osteoarthr Cartil. 2008;16(12):1532–8.
Sim S, Chevrier A, Garon M, Quenneville E, Lavigne P, Yaroshinsky A, et al. Electromechanical probe and automated indentation maps are sensitive techniques in assessing early degenerated human articular cartilage. J Orthop Res. 2017;35(4):858–67.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale: L. Erlbaum Associates; 1988. p. 567. xxi
Kohl HW 3rd, Craig CL, Lambert EV, Inoue S, Alkandari JR, Leetongin G, et al. The pandemic of physical inactivity: global action for public health. Lancet. 2012;380(9838):294–305.
de Souto Barreto P. Time to challenge public health guidelines on physical activity. Sports Med. 2015;45(6):769–73.
Shrier I. Muscle dysfunction versus wear and tear as a cause of exercise related osteoarthritis: an epidemiological update. Br J Sports Med. 2004;38(5):526–35.
O'Keefe JH, Franklin B, Lavie CJ. Exercising for health and longevity vs peak performance: different regimens for different goals. Mayo Clin Proc. 2014;89(9):1171–5.
Plews DJ, Laursen PB, Kilding AE, Buchheit M. Heart rate variability in elite triathletes, is variation in variability the key to effective training? A case comparison. Eur J Appl Physiol. 2012;112(11):3729–41.
Kujala UM, Kettunen J, Paananen H, Aalto T, Battie MC, Impivaara O, et al. Knee osteoarthritis in former runners, soccer players, weight lifters, and shooters. Arthritis Rheum. 1995;38(4):539–46.
Rahnamay Moshtagh P, Korthagen NM, Plomp SG, Pouran B, Sanchez C, Henrotin Y, et al. Effect of moderate increasing exercise on the mechanical balance of the knee joint in young rats. Osteoarthr Cartil. 2017;25:S66–S7.
Sengupta P. The laboratory rat: relating its age with human’s. Int J Prev Med. 2013;4(6):624–30.
Bond Brill J, Perry AC, Parker L, Robinson A, Burnett K. Dose-response effect of walking exercise on weight loss. How much is enough? Int J Obes Relat Metab Disord. 2002;26(11):1484–93.
Pereira BC, Pauli JR, de Souza CT, Ropelle ER, Cintra DE, Rocha EM, et al. Nonfunctional overreaching leads to inflammation and myostatin upregulation in Swiss mice. Int J Sports Med. 2014;35(2):139–46.
Sipila S, Multanen J, Kallinen M, Era P, Suominen H. Effects of strength and endurance training on isometric muscle strength and walking speed in elderly women. Acta Physiol Scand. 1996;156(4):457–64.
Phelan S, Wadden TA, Berkowitz RI, Sarwer DB, Womble LG, Cato RK, et al. Impact of weight loss on the metabolic syndrome. Int J Obes. 2007;31(9):1442–8.
Pi-Sunyer FX. A review of long-term studies evaluating the efficacy of weight loss in ameliorating disorders associated with obesity. Clin Ther. 1996;18(6):1006–35. discussion 5
Toda Y, Toda T, Takemura S, Wada T, Morimoto T, Ogawa R. Change in body fat, but not body weight or metabolic correlates of obesity, is related to symptomatic relief of obese patients with knee osteoarthritis after a weight control program. J Rheumatol. 1998;25(11):2181–6.
Christensen R, Astrup A, Bliddal H. Weight loss: the treatment of choice for knee osteoarthritis? A randomized trial. Osteoarthr Cartil. 2005;13(1):20–7.
Ren JM, Semenkovich CF, Gulve EA, Gao J, Holloszy JO. Exercise induces rapid increases in GLUT4 expression, glucose transport capacity, and insulin-stimulated glycogen storage in muscle. J Biol Chem. 1994;269(20):14396–401.
Powers SK, Lennon SL. Analysis of cellular responses to free radicals: focus on exercise and skeletal muscle. Proc Nutr Soc. 1999;58(4):1025–33.
Ou Y, Tan C, An H, Jiang D, Quan Z, Tang K, et al. Selective COX-2 inhibitor ameliorates osteoarthritis by repressing apoptosis of chondrocyte. Med Sci Monit. 2012;18(6):BR247–52.
Mastbergen SC, Marijnissen AC, Vianen ME, Zoer B, van Roermund PM, Bijlsma JW, et al. Inhibition of COX-2 by celecoxib in the canine groove model of osteoarthritis. Rheumatology (Oxford). 2006;45(4):405–13.
Blazek AD, Nam J, Gupta R, Pradhan M, Perera P, Weisleder NL, et al. Exercise-driven metabolic pathways in healthy cartilage. Osteoarthr Cartil. 2016;24(7):1210–22.
Kusada J, Otsuka T, Matsui N, Hirano T, Asai K, Kato T. Immuno-reactive human epidermal growth factor (h-EGF) in rheumatoid synovial fluids. Nihon Seikeigeka Gakkai Zasshi. 1993;67(9):859–65.
Jakob M, Demarteau O, Schafer D, Hintermann B, Dick W, Heberer M, et al. Specific growth factors during the expansion and redifferentiation of adult human articular chondrocytes enhance chondrogenesis and cartilaginous tissue formation in vitro. J Cell Biochem. 2001;81(2):368–77.
Appleton CT, McErlain DD, Henry JL, Holdsworth DW, Beier F. Molecular and histological analysis of a new rat model of experimental knee osteoarthritis. Ann N Y Acad Sci. 2007;1117:165–74.
Shepard JB, Jeong JW, Maihle NJ, O'Brien S, Dealy CN. Transient anabolic effects accompany epidermal growth factor receptor signal activation in articular cartilage in vivo. Arthritis Res Ther. 2013;15(3):R60.
Zhang X, Tamasi J, Lu X, Zhu J, Chen H, Tian X, et al. Epidermal growth factor receptor plays an anabolic role in bone metabolism in vivo. J Bone Miner Res. 2011;26(5):1022–34.
Itoh CE, Kizaki T, Hitomi Y, Hanawa T, Kamiya S, Ookawara T, et al. Down-regulation of beta2-adrenergic receptor expression by exercise training increases IL-12 production by macrophages following LPS stimulation. Biochem Biophys Res Commun. 2004;322(3):979–84.
Mattner F, Magram J, Ferrante J, Launois P, Di Padova K, Behin R, et al. Genetically resistant mice lacking interleukin-12 are susceptible to infection with Leishmania major and mount a polarized Th2 cell response. Eur J Immunol. 1996;26(7):1553–9.
McIntyre KW, Shuster DJ, Gillooly KM, Warrier RR, Connaughton SE, Hall LB, et al. Reduced incidence and severity of collagen-induced arthritis in interleukin-12-deficient mice. Eur J Immunol. 1996;26(12):2933–8.
Parks E, Strieter RM, Lukacs NW, Gauldie J, Hitt M, Graham FL, et al. Transient gene transfer of IL-12 regulates chemokine expression and disease severity in experimental arthritis. J Immunol. 1998;160(9):4615–9.
Acknowledgements
The authors thank Dr. Tannin Schmidt for providing access to the Mach-1 v500css for mechanical testing and Carolyn Hewitt for technical contributions to this paper.
Funding
This work was supported by the Canadian Institutes of Health Research # RT736475 and MOP 115076, the Canada Research Chair Programme, the Alberta Innovates Health Solutions Osteoarthritis Team Grant, Alberta Innovates Health Solutions, Killam Foundation, and the Ministry of Education, Brazil (CAPES Foundation Grant 13157-13-2).
Availability of Data and Materials
The datasets supporting the conclusions of this article are included within the article.
Author information
Authors and Affiliations
Contributions
JLR was responsible for the design of the study, execution of the study, data collection, data analysis, interpretation of data, drafting the manuscript, revising the manuscript, and approving the final submitted version. KRB was responsible for the design of the study, execution of the study, data collection, interpretation of data, revising the manuscript, and approving the final submitted version. JWM was responsible for the data collection, data analysis, interpretation of data, and approving the final submission. RAS was responsible for the data analysis, interpretation of data, and approving the final submission. DAH was responsible for the data analysis, interpretation of data, drafting the manuscript, revising the manuscript, and approving the final submission. WH contributed to the study design, interpretation of the data, writing the manuscript, revising the manuscript, and approving the final submission.
Corresponding author
Ethics declarations
Ethics Approval
All experiments were approved by the University of Calgary Life and Environmental Sciences Animal Care Committee (AC12-0139), and all methods were conducted in accordance with the animal welfare regulations and guidelines at the University of Calgary.
Consent for Publication
Not applicable.
Competing Interests
Jaqueline Lourdes Rios, Kevin Rudi Boldt, James William Mather, Ruth Anne Seerattan, David Arthur Hart, and Walter Herzog declare that they have no conflict of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Rios, J.L., Boldt, K.R., Mather, J.W. et al. Quantifying the Effects of Different Treadmill Training Speeds and Durations on the Health of Rat Knee Joints. Sports Med - Open 4, 15 (2018). https://doi.org/10.1186/s40798-018-0127-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-018-0127-2