
Abstract
Objective
The purpose of this study was to systematically evaluate the methodological quality of massage-related clinical practice guidelines (CPGs)/consensus on massage using the Appraisal of Guidelines Research and Evaluation (AGREE II) instrument and to summarize the current status of recommendations in the CPGs.
Methods
The Chinese National Knowledge Infrastructure (CNKI), WanFang Data, China Science and Technology Journal Database (VIP), China Biology Medicine disc (CBM), PubMed, Embase, and guideline websites (such as the Chinese Medical Ace Base, the China Association of Chinese Medicine, the World Health Organization, Guideline International Network, National Institute for Health and Care Excellence, Scottish Intercollegiate Guidelines Network) were searched from inception to October 31, 2022. In addition, the reference lists of relevant studies were reviewed to identify domestic and overseas massage CPGs/consensus. The search terms adopted a combination of subject words and free words, mainly including traditional Chinese medicine, complementary therapies, Tuina, massage, manipulation, chiropractic/osteopathic, spinal, acupressure, guideline, and consensus. Two researchers independently completed the eligible records and extracted the data. Before the formal research, calibrations were performed twice on AGREE II, and all reviewers completed the pilot test three times until they understood and reached an agreement on the assessment items. Three researchers appraised the methodological quality of the included guidelines using the AGREE II instrument and calculated the overall intraclass correlation coefficient (ICC) of agreement.
Results
The evaluation results showed that among the 49 eligible CPGs/consensus, 4 (8.2%) CPGs/consensus were considered “recommended”, 15 (30.6%) CPGs/consensus were considered “recommended with modifications”, and 30 (61.2%) CPGs/consensus were considered “not recommended”, while the consensus was considered “not recommended”. Generally, the scores in the six domains of the guidelines were all higher than the consensus. Evaluation results for the overall quality of 36 CPGs showed that 4 (11%) were “good quality”, 15 (42%) were “sufficient quality” and 17 (47%) were “lower quality”. The AGREE II quality scores of domains ranged from 0.30 to 0.75 ([ICC = 0.993, 95% CI (0.992, 0.995)]). The domain of scope and purpose (domain 1), with a median score of 0.75 (0.52~0.91), performed best in the guidelines with AGREE II, and stakeholder involvement (domain 2) [median 0.39 (0.31~0.56)] and application (domain 5) [median 0.30 (0.17~0.47] obtained lower scores. The consensus score of domain 1 was better at 26.0 (21.6~44.8), followed by rigor of development (domain 3) with a score of 18.0 (10.0~28.9). A total of 119 massage-related recommendations were extracted from 49 guidelines/consensuses, including “in favor” (102, 85.7%), “against” (9, 7.6%), and “did not make recommendations” (8, 6.7%).
Conclusion
The overall quality of the included guidelines was low, and most of the guidelines were not “recommended”. In future guideline updates, the existing evidence should be used, the professional composition of members of the expert group should be enriched, and patients’ values and preferences should be fully considered. It is necessary to clearly propose recognizable recommendations and strengthen the rigor and standardization of guideline formulation. Thus, clear standard guidelines can be formulated to better guide clinical practice.
Similar content being viewed by others


Introduction
Massage dates back to at least the second century B.C. and is generally defined as the manipulation of soft tissue [1, 2]. It is one of the oldest therapeutic techniques to which people around the world attach importance [3]. It can improve microcirculation and regulate the human body’s subhealth and health conditions by manipulating muscles or connective tissues [4].
Massage therapy is a widespread and beneficial intervention of complementary medicine and has been well recognized and adopted in clinical practice. Some reviews have summarized the clinical applications of massage therapy for various diseases, including improving health and development in preterm/low-birth weight infants, reducing pain and anxiety, and treating some respiratory and digestive system diseases [5, 6]. In a systematic review of abdominal massage, massage was used for adult digestive disorders, pediatric disorders, gynecological disorders, obstetric disorders, metabolic disorders, and psychological disorders [7]. In the absence of sufficiently effective and safe pharmacological treatments for these diseases, massage as a nonpharmacological therapy has become a viable means of treating these diseases by avoiding possible side effects while reducing pain and discomfort [8].
With the widespread use of massage therapy, clinical evidence of the use of massage for various diseases or symptoms is rapidly growing. A recent review summarized the evidence related to pediatric massage based on 38 published systematic and nonsystematic reviews. The results presented more positive effects than lack of effect, and no negative effects were found in four major outcome groups with regard to physical and metabolic aspects, well-being and quality of life, mental health and behavior, and management [9]. For the improvement of psychological variables and subjective symptoms, such as pain and quality of life, there appears to be better evidence [10], which provides an important basis for the clinical application of massage.
With the development of complementary and alternative medicine, massage therapy is no longer supported solely by the personal experience of the physician or practitioner but is also supported by high-quality scientific evidence. Some clinical practice guidelines (CPGs) on massage have been developed to assist physicians and practitioners with the integration of evidence into clinical decision-making. These CPGs involve acute or chronic pain [11], cancer [12], and some digestive system diseases of children [13, 14].
High-quality CPGs are a decision-making tool to narrow the gap between current best evidence and clinical practice. They can help healthcare providers balance the risks and benefits of therapies, which ultimately leads to better patient outcomes and improves medical quality [15, 16]. Therefore, it is very important to assess the quality of CPGs.
Although many massage-related CPGs/consensuses have been developed internationally and have played a positive role in promoting the standardized use and treatment of disease with massage therapy, the quality of these guidelines/consensuses is not clear. Therefore, the integration of guidance evidence is necessary. This study systematically evaluated the methodological quality of massage-related CPGs/consensus using the Appraisal of Guidelines Research & Evaluation (AGREE II) instrument (available at http://www.agreetrust.org/) and summarized the current status of recommendations in the CPGs.
Methods
Eligibility criteria
No restriction was placed on classifications of massage, and eligible CPGs/consensus were included with reference to the “PICAR” framework [17].
-
(1)
Population, interventions, and comparators
The population of eligible CPGs/consensus for patients who require massage intervention. This review does not state ‘comparators’.
-
(2)
Attributes of the CPG/consensus
The following criteria were used: (1) the title or abstract included the keywords ‘CPG’ or ‘guideline’ or ‘guidelines’ or ‘guidance’ or ‘consensus’; (2) the full text included ‘massage’ or ‘chiropractic’ or ‘acupressure’ or ‘manipulation’ or ‘osteopathic’ or ‘Tuina’ or ‘spinal’; (3) CPGs/consensus included recommendations related to ‘massage’ or ‘chiropractic’ or ‘acupressure’ or ‘manipulation’ or ‘osteopathic’; (4) CPGs/consensus were released or published in scientific paper or were the latest versions of CPGs available when multiple versions exist.
We excluded CPGs according to the following criteria: (1) full text of guidelines was not available; (2) earlier versions of guidelines with an available updated version, secondary or multiple publications; (3) interpretation or translation of guidelines/consensus, abstract of submission, systematic reviews, narrative reviews, primary studies, critical/clinical pathways, training manuals for medical professionals, textbook-like publications, guidelines for patients, editorials, translations of foreign guidelines or short summaries; (4) did not contain recommendations on ‘massage’ or ‘chiropractic’ or ‘acupressure’ or ‘manipulation’ or ‘osteopathic’; and (5) guidelines published in languages other than Chinese or English.
Search strategy
The literature search was conducted by two reviewers (M.Y.F., B.Q.L.) from inception to October 31, 2022. The search was limited to humans and the Chinese or English language. The systematic literature search was conducted in the following databases: Chinese Biomedical Literature database (http://www.sinomed.ac.cn/), WanFang database (Chinese Medicine Premier, http://www.wanfangdata.com.cn/), VIP (Chinese journals full-text database, http://data.whlib.ac.cn/), China National Knowledge Infrastructure (http://www.cnki.net/), China Biology Medicine disc (www.sinomed.ac.cn), PubMed (https://pubmed.ncbi.nlm.nih.gov), Excerpta Medica Database (https://www.embase.com), and guideline websites, such as the Chinese Medical Ace Base (http://seleguide.yiigle.com/), the China Association of Chinese Medicine (http://www.cacm.org.cn/category/), the World Health Organization (https://www.who.int), Guideline International Network (https://guidelines.ebmportal.com), National Institute for Health and Care Excellence (https://www.nice.org.uk), Canadian Medical Association CPG Infobase (https://joulecma.ca/cpg/), Scottish Intercollegiate Guidelines Network(https://www.sign.ac.uk/). Search terms were (“guidelines as topic” OR “guideline” OR guideline* OR guidance OR recommendation* OR consensus) AND (massage OR chiropractic OR acupressure OR “massage” OR “chiropractic” OR “acupressure” OR “Tuina” OR “manipulation” OR “osteopathic” OR “spinal”) AND (“Complementary Therapies” OR “Medicine, East Asian Traditional” OR complementary OR “East Asian Traditional” OR TCM OR “Chinese medicine” OR “traditional Chinese” OR “traditional medicine” OR “alternative” OR “oriental medicine” OR “east Asian medicine”) AND “human” OR human. Detailed construction of these search strategies is attached in Supplementary Material: Appendix 1.
CPGs/consensus selection and data extraction
Two reviewers (M.Y.F. and B.Q.L.) independently imported the bibliography into EndNote X9 and removed duplicates from the bibliography. Then, Microsoft Excel 2021 was used to screen the titles and abstracts. Finally, we screened the full texts to identify the included CPGs/consensus. Disagreements were resolved by consensus or a third reviewer (C.T.).
Two reviewers (M.Y.F. and X.W.Z.) independently extracted descriptive information from the included CPGs/consensus and cross-checked it to ensure data quality. The following three sections were extracted from the included CPGs/consensus: general characteristics of CPGs/consensus (title, authorship list, date of publication, organization/society that developed the guidelines, target users, sponsoring organization, country, updated/original, target population, disease classification, age group of target population, definition of massage/Tuina, search year covered, methods used to determine recommendations); characteristics of guidelines concerning the contents of rigor of development (systematic search, databases, comprehensive search strategies, study basis for massage recommendations, methods used to determine recommendations, peer review); general recommendations (criteria for rating evidence, criteria for grading recommendation, disease classification, number of recommendations related to massage/Tuina, population, alone or with other interventions, direction of the recommendation, basis for recommendation, certainty of evidence, strength of recommendation, type of intervention).
Assessment for guideline quality and investigation of heterogeneity
The Appraisal of Guidelines Research & Evaluation (AGREE II) instrument [18,19,20] is a tool used to assess the methodological quality of CPGs. It was translated into Chinese by Li Min Xie and Wenyue Wang at Guang’anmen Hospital [21]. The AGREE II scale is composed of 23 items grouped into 6 domains using a seven-point scale from 1 for “strongly disagree” to 7 for “strongly agree”. Based on examples and instructions in the AGREE II manual [18], the appraisers rated each of the AGREE II items and the two global rating items.
The total was calculated by summing the scores of all items within the domain and scaling the total as a percentage of the maximum possible score for that domain. A scaled domain percentage score was calculated according to the AGREE II methodology as follows:
To reflect the recommendation intention after the overall quality assessment of each CPG/consensus, the overall score was obtained by calculating the sum of six domain scores and dividing by 600%. The total score range was 0–100% [22, 23]. The domain scores were categorized as good quality (≥ 70%), sufficient quality (50–70%), and lower quality (< 50%), which indicated corresponding recommendation intentions for each CPG as “recommended” (≥ 70%), “recommended with modifications” (50–70%) or “not recommended” (< 50%). The ‘obtained score’ was the sum of the appraisers’ scores for each item, making it possible to consider the natural discrepancies between the two appraisers.
Three appraisers (M.Y.F., X.W.Z., and C.T.), including a guideline methodologist, received similar training in regard to the process and methods of guideline development as well as the application of the AGREE II instrument. They were pilot-tested before they independently conducted the CPG evaluation. Except for the guideline methodologist, the other two appraisers were clinicians with experience in massage and health care improvement. The overall evaluations, including recommend, recommend with modifications or do not recommend, were independently determined by each appraiser. Every guideline was assessed by at least two assessors.
Statistical analysis
The characteristics of the included CPGs and consensus are depicted as the number of guidelines and the proportion to the total number of guidelines (N (%)). For the AGREE II quality assessment, the scores of all eligible guidelines from three appraisers were summarized and calculated and were presented as the median and 25–75% (M (P 25 ~P 75)) and mean and standard deviation (SD) values, which showed the proportion of standardized scores for each domain of the guideline and the consensus. The agreement among appraisers was calculated using the intraclass correlation coefficient (ICC) [24], defined as follows: < 0.20, poor; 0.21–0.40, fair; 0.41–0.60, moderate; 0.61–0.80, good, 0.81–1.00, very good [25, 26]. ICC calculations were performed using the Statistical Package for Social Science (SPSS) software (version 18).
Results
Literature search and selection
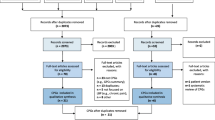
The searches retrieved 5389 hits, of which, we excluded 1065 duplicates and 4264 records after screening titles and abstracts, leaving 60 full-text articles that were screened and 49 full-text articles were assessed for eligibility. Of the 60 full texts, we excluded 11 articles for the following reasons: 1 was a systematic review of CPGs related to massage, 1 was not in English nor Chinese languages, 1 was an abstract, 1 was by consensus process, 4 were original versions, and 3 were not available as full text. The process for selecting the articles is presented in Fig. 1. The ggplot2 package of R studio (v 2022.12.0-353) was used for raincloud plotting, and the bubble plot depicting the assessment results of guidelines and CPGs concerning different disease types was processed in Bioinformatics (https://www.bioinformatics.com.cn/) [27].

Flow chart of the selection process
Characteristics of included CPGs and consensus
Forty-nine articles were included; 36 (73.5%) of them were CPGs and 13 (26.5%) were expert consensus. The included guidelines/consensus were mainly developed from organizations or societies, a majority of which were located in America (25, 51.0%). The CPGs were published between 2006 and 2022, and 20 CPGs (11.54%) were updated versions. Among these, 18 (36.7%) guidelines used Grading of Recommendations Assessment, Development, and Evaluation (GRADE) to assess the certainty of the evidence, and the other 18 (36.7%) used GRADE to assess the strength of the recommendation. The eligible CPGs and consensus characteristics are illustrated in Table 1 and Supplementary Material Appendix 2.
AGREE II quality scores
The ICC analysis showed very good agreement among the three reviewers [ICC = 0.993, 95% CI (0.992, 0.995)].
Evaluation results for the overall quality of 36 CPGs showed that 4 (11%) were “good quality”, 15 (42%) were “sufficient quality” and 17 (47%) were “lower quality”. The AGREE II quality scores of domains ranged from 0.30 to 0.75 (see Fig. 2). The domain with the highest score across the guidelines was scope and purpose, with a median of 0.75 (0.52~0.91). The stakeholder involvement domain [median: 0.39 (0.31~0.56)] and application domain [median: 0.30 (0.17~0.47] obtained lower scores. Each domain presented different results in various guidelines (see Table 2). AGREE II scores of each eligible CPG/consensus are presented in Supplementary Material Appendix 3.

AGREE II assessment by domain of 36 guidelines. The raincloud plot with Mean score ± 95% CI comprehensively depicts the distribution of the AGREE II score of the guidelines in each domain. Each dot exhibits the standard value combined assessment of three researchers concerning each guideline
Scope and purpose
The average score of the six included guidelines in terms of the scope and purpose domain was 0.73, 95% CI (52.0~92.5), ranging from 0.26 to 1.00 [28,29,30,31,32,33]. Most eligible guidelines comprehensively described the overall purpose, health questions and target populations, except for 5 guidelines [13, 34,35,36,37] that did not describe the health intents, expected benefit/outcome, or target population, three guidelines [36,37,38] that did not provide a detailed description of PICO questions, i.e., population, intervention or exposure, comparative and study outcomes, and 1 guideline [39] that did not explicitly describe the details of the target population.
Stakeholder involvement
The overall score in this domain was low; the average score was 0.44, 95% CI (31.0~56.8). All CPGs reported comprehensive member information of the guideline development group. Ten CPGs [11, 12, 33, 34, 36, 38, 40,41,42,43] did not mention the patient’s views and preferences, while the target users were not clearly defined in nine CPGs [34, 36, 39,40,41, 44,45,46,47].
Rigor of development
The mean score for this domain was 0.55, 95% CI (44.3~66.5). Twenty-four guidelines scored above 50%, and three guidelines scored below 25%. Five guidelines [35,36,37,38, 48] did not provide detailed search strategies. The inclusion/exclusion criteria were explicitly described in eight guidelines [12, 32, 40, 41, 49,50,51,52]. Most guidelines clearly described the strengths or limitations of the body of evidence and health benefits, harms or risks of side effects. Four CPGs [37,38,39, 48] did not report criteria for rating evidence, and seven CPGs [11, 34, 37, 41, 48, 49, 53] did not address the methods for formulating the recommendations. Two CPGs [38, 42] did not mention benefits, harms or the balance between them. Only 1 guideline [31] provided comprehensive updated information.
Clarity of presentation
In the clarity of presentation domain, the mean score was 0.55, 95% CI (44.0~66.5). We found that two CPGs [32, 42] lacked specific and unambiguous recommendations. In five CPGs [13, 14, 34, 42, 54], multiple options with detailed population or clinical situation descriptions were provided for each targeted question, and key recommendations were presented in unclear ways, i.e., they could not be clearly recognized in the texts of those CPGs [32, 42, 49].
Applicability
The score for the application domain was 31.9% ± 21.2%, 95% CI (17.0~48.3). The potential resource implications, details of the described facilitators, or barriers to application were not clearly defined in most CPGs, except for six CPGs [12, 13, 32, 33, 36, 47] that identified the types of facilitators and barriers. Facilitators included a wide variety of locations for therapy implementation [12, 13], supportive policy from the local government, standardized training procedures provided to the practitioners [13], etc. Several barriers mentioned in those CPGs which might impact the guideline implementation, such as lack of availability in community hospitals [33], loss of skill over time from disuse, inadequate office space [32], etc.
Four guidelines [14, 28, 33, 55] mentioned information regarding the facilitators and barriers to implementing recommendations, and five guidelines [31, 32, 39, 55, 56] provided advice and tools on how the recommendations could be put into practice. In addition, only three guidelines [56,57,58] fully considered the potential resource implications of applying the recommendations, and two guidelines [51, 57] completely presented performance monitoring indicators and auditing criteria, including advice on the frequency and interval of measurement descriptions and operational definitions of how the criteria should be measured.
Editorial independence
This domain obtained a mean score of 56.1% ± 28.2%, 95% CI (33.0~83.0). Four CPGs [12, 45, 46, 59] did not state that the views of the funding body had not influenced the content of the guidelines, 4 CPGs [11, 35, 41, 49] did not present the conflicts of interest of the guideline development group members, while 1 CPG failed to declare both [37].
The overall assessment ratings for the 13 consensuses evaluated ranged from 0.06 to 0.46. All consensus were classified as “lower quality”. For 13 consensuses the average scores of AGREE II domains 1–6 were 33.2%, 18.0%,19.4%, 9.83%, 18.0% and 26.9%, respectively (see Table 3). It shows that each domain needs to be improved. The consensus lacks recommendations, which leads to a low rating in the ‘Clarity of presentation’ domain. Comparing with consensus, the development of CPGs is more rigorous, structured and reliably organized.
Level of evidence and strength of recommendation
Thirty-four CPGs (83.33%) used 10 types of grading systems to rate the level of evidence and the strength of recommendation (see Table 4). The GRADE system with wider acceptance was adopted in the development of 16 CPGs. The grading system of evidence and recommendation was not reported in 2 guidelines [39, 48]
Recommendations for massage interventions
We included 11 massage-specific CPGs/ consensuses and 38 disease-based CPGs/ consensuses with recommendations in terms of massage.
General view of the recommendations
A total of 119 massage-related recommendations were extracted from 36 guidelines. It included “in favor” (102, 85.7%), which meant the massage was recommended for use. For instance, in the CPGs applied GRADE [13, 14], in favor was divided into “strong” or “weak” levels; and the same for “against” (9, 7.6%), which meant the massage wasn’t recommended for use. It was also divided into “strong” or “weak” based on GRADE according to CPGs [13, 14]. For those addressed “did not make recommendations” (8, 6.7%), some of the CPGs provided certain circumstances under which massage was not recommended, e.g., spinal manipulation cannot be recommended for the management of patients with episodic tension-type headache [40], though others did not mention the contents.
Target population
Figure 3 shows that the target populations of 9 (18.4%) CPGs and consensus were children and adolescents (< 18 years), while 24 (49%) targeted middle-aged adults and elderly people (≥ 18 years) and the general population (16, 32.7%). Massage-related diseases were classified according to the International Classification of Diseases 11th Revision (ICD-11). Most (28, 57.1%) were musculoskeletal system diseases. The evaluation results showed that among the 49 eligible CPGs/consensuses, 4 (8.2%) CPGs/consensuses were considered “recommended”, 15 (30.6%) CPGs/consensuses were considered “recommended with modifications”, and 30 (61.2%) CPGs/consensuses were considered “not recommended”.

Different disease types covering massage recommendations and quality assessment of guidelines and consensus based on AGREE II. The size and color of the circle represent the number of recommendations, as the number increases, the circles become larger and darker
Intervention characteristics
Table 5 shows that massage intervention characteristics were divided into two types, including massage interventions alone, which accounted for a large proportion (84, 70.59%).
Discussion
Summary of the findings
To the best of our knowledge, this article is the first systematic and comprehensive assessment of the quality of current CPGs available for massage. We assessed the methodological quality of 49 massage-related CPGs/consensuses and extracted 119 massage-related recommendations from the included CPGs/consensuses, among which the “in favor” recommendations accounted for a large proportion of total recommendations (102, 85.7%). Developed/updated guidelines tended to have higher quality than earlier versions. Evidence-based guidelines scored consistently higher in all domains. A lack of international authoritative instruments in the appraisal of consensus might result in insufficient authenticity of evaluation.
Relation to other studies
Several previous studies have evaluated the quality of massage-related guidelines, but these studies only focused on certain forms of massage or certain diseases. For example, a previous study assessed four guidelines for spinal manipulation in a study of complementary and alternative medicine (CAM) guidelines. In overall recommendations, these four guidelines were rated “yes, with modifications” [60]. However, in our studies, more than half of the guidelines/consensus was assessed as “not recommended”. The difference in results was likely due to the focus of the CAM guidelines on spinal manipulation, which also explains their failure to provide the broad range of massage guidelines that our study describes. In another quality appraisal of CPGs regarding nonpharmacological interventions for breast cancer survivors [61], massage was rated as “recommended” to alleviate the symptoms of anxiety, depression and distress in breast cancer survivors. The level of recommendation was also inconsistent with our study, which was “not recommended”.
Strengths and limitations
Our study identified several strengths. First, the study was the latest methodological quality study that evaluated the quality of CPGS addressing massage interventions using the AGREE II instrument. Second, our study consisted of experienced clinical experts and methodologists in CPGs, to guide the guideline evaluation process. Third, we performed a systematic search of the literature to ensure the reliability of the findings.
Nevertheless, our study also had some limitations. We only assessed guidelines published in commonly used databases, which may not represent all massage guidelines. Guidelines published in other forms (i.e., books, booklets, or government documents) may have been missed. We only included guidelines published in Chinese or English, and some non-Chinese or non-English guidelines might have been missed. Thus, we may have underestimated guideline quality in some instances.
Proposals for improving the quality of massage guidelines and consensuses
From 49 included CPGs/consensuses, 28 CPGs/consensuses were musculoskeletal system diseases, of which 9 were rated “recommended” or “recommended with modifications” and 19 were “not recommended”. This indicated that the current evidence was inconsistent in supporting the efficacy of massage in treating musculoskeletal system diseases. Similarly, the quality of evidence was inconsistent or poor for some other diseases, which may lead to a lack of supporting evidence available for physicians or practitioners. Therefore, we suggest that massage CPGs/consensus developers focus on improving the quality of massage therapy recommendations.
The overall quality of guidelines related to massage was low. Development of guidelines must follow a rigorous set of procedures [62], e.g., target audience, systematic review, evidence retrieval and synthesis, formulate recommendations, convene meetings, implementation, publishing, and updating. Guideline developers should pay more attention to the clarity of presentation, rigor of development, and applicability according to our study. In addition to the low quality of the CPGs, lack of well recognized placebo/sham control or poor comparability of individualized practitioner-based therapy may directly affect the quality of the massage research.
In accordance with AGREE II, there were two domains showed low scores based on our research, potential reasons might be few CPGs considered patients’ values/preferences or the absence of target users’ clarification/definition for “stakeholder involvement” domain; in the “application” domain, seldom implementation recommendations or applicable instruments were provided, less considerations on massage related resource implications, and inadequate detailed suggestions of massage interventions, such as frequencies or episodes for each acupoints due to different age groups, could be obtained. The high rating in the ‘scope and purpose’ domain reflected that objective(s) of the guideline, Population/Intervention/Comparison/Outcome/Study design (PICOs), and target population were comprehensively described.
In future guideline updates, the existing evidence should be reasonably adopted, the professional composition of the members of the expert group should be enriched, and patients’ values and preferences should be fully considered. It is necessary to propose recognizable recommendations and strengthen the rigor and standardization of guideline formulation to formulate clear and standard guidelines to better guide clinical practice.
Implications
The development of the CPGs involves health promotion, screening, therapy, diagnosis, or prognosis [63]. Improved quality of guidelines may benefit all stakeholders, including healthcare workers, patients, and healthy individuals [64]. The evidence-based massage CPGs provided unbiased recommendations that were effective, safe and appropriate for patients, helping avoid ineffective or potentially harmful options [63]. CPGs may transform healthcare delivery and enhance patient outcomes [65]. Therefore, efforts must be made to guarantee the improvement of the quality of the CPGs. Our study also provided an exemplary practical approach to the quality evaluation of other guidelines.
Future research directions
The findings of this article also provided some future research directions. First, the quality of the guidelines was low. On one hand, we need to focus on improving the quality of the CPGs to guide clinical practice. On the other hand, we need to conduct well-powered randomized controlled trials to improve the evidence bases. Second, through real-world study, we can obtain data on the advantageous diseases treated with massage. It will be helpful for researchers or doctors to conduct clinical trials and evaluate its clinical efficacy. Third, we may also develop some massage-specialized CPGs for the treatment of advantageous diseases, which would be valuable complementation for disease-based guidelines adopted by non-pharmacological therapies.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Dryden T, Moyer CA. Massage therapy: integrating research and practice. United States of America: Human Kinetics; 2012.
Benjamin PJ, Tappan FM. Tappan's Handbook of Healing Massage Techniques: Classic, Holistic and Emerging Methods. Upper Saddle River, N.J.: Prentice Hall; 2005.
Field TM. Massage therapy effects. Am Psychol. 1998;53:1270–81.
Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States. Natl Health Stat Report. 2007;2008:1–23.
Wang Y, Liu K, Quan R, et al. Study on disease spectrum of infantile massage therapy. J Liaoning Univ Tradit Chin Med. 2013;08:60–2.
Beider S, Mahrer NE, Gold JI. Pediatric massage therapy: an overview for clinicians. Pediatr Clin N Am. 2007;54:1025–41.
Wang G, Zhang Z, Sun J, et al. Abdominal massage: a review of clinical and experimental studies from 1990 to 2021. Complement Ther Med. 2022;70:102861.
Cordeiro Santos ML, da Silva Júnior RT, de Brito BB, et al. Non-pharmacological management of pediatric functional abdominal pain disorders: current evidence and future perspectives. World J Clin Pediatr. 2022;11:105–19.
de Britto Pereira PAD, Mendes Abdala CV, Portella CF, et al. Pediatrics massage evidence map. Complement Ther Med. 2021;61:102774.
Kopf D. Massage and touch-based therapy: Clinical evidence, neurobiology and applications in older patients with psychiatric symptoms. Z Gerontol Geriatr. 2021;54(8):753–8.
Brosseau L, Wells GA, Poitras S, et al. Ottawa Panel evidence-based clinical practice guidelines on therapeutic massage for low back pain. J Bodyw Mov Ther. 2012;16:424–55.
Greenlee H, Du Pont-Reyes MJ, Balneaves LG, et al. Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA Cancer J Clin. 2017;67:194–232.
Ge L, Cao X, Zhang Q, et al. Tuina for children with acute diarrhea: an evidence-based clinical guideline. Chin J Evid Based Med. 2021;21:745–53.
Ge L, Cao X, Wu R. Evidence-based clinical practice guidelines on Tuina for children with anorexia (2021 edition). J Tradit Chin Med. 2022;63:1295–300.
Wang J, Li Y, Tian K, et al. Systematic review on methodological quality of domestic traditional Chinese medicine oncology guidelines and expert consensu. World Science and Technology-Modernization of Traditional Chinese Medicine. 2021;23:4735–43.
Ng JY, Bhatt HA, Raja M. Complementary and alternative medicine mention and recommendations in pancreatic cancer clinical practice guidelines: a systematic review and quality assessment. Integr Med Res. 2023;1:100921.
Johnston A, Kelly SE, Hsieh SC, et al. Systematic reviews of clinical practice guidelines: a methodological guide. J Clin Epidemiol. 2019;108:64–76.
Brouwers MC, Kho ME, Browman GP, et al. AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting, and evaluation in health care. Prev Med. 2010;182:E839–E42.
Brouwers MC, Kho ME, Browman GP, et al. AGREE Next Steps Consortium. Development of the AGREE II, part 1: performance, usefulness and areas for improvement. CMAJ. 2010;182:1045–52.
Brouwers MC, Kho ME, Browman GP, et al. AGREE Next Steps Consortium. Development of the AGREE II, part 2: assessment of validity of items and tools to support application. CMAJ. 2010;182:E472-E8.
Xie M, Wang Y. A brief introduction to Appraisal of Guidelines for Research and Evaluation II. Journal of Chinese Integrative Medicine. 2012;10:160–5.
Andrade R, Pereira R, van Cingel R, et al. How should clinicians rehabilitate patients after ACL reconstruction? A systematic review of clinical practice guidelines (CPGs) with a focus on quality appraisal (AGREE II). Br J Sports Med. 2020;54:512–9.
Li X, Yu X, Xie Y, et al. Critical appraisal of the quality of clinical practice guidelines for idiopathic pulmonary fibrosis. Ann Transl Med. 2020;8:1405.
Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979;86:420–8.
Armstrong JJ, Rodrigues IB, Wasiuta T, et al. Quality assessment of osteoporosis clinical practice guidelines for physical activity and safe movement: an AGREE II appraisal. Arch Osteoporos. 2016;11:6.
Messina C, Bignotti B, Bazzocchi A, et al. A critical appraisal of the quality of adult dual-energy X-ray absorptiometry guidelines in osteoporosis using the AGREE II tool: An Euro AIM initiative. Insights Imaging. 2017;8:311–7.
Wickham H. Ggplot2: Elegant Graphics for Data Analysis. New York: Springer-Verlag; 2016. [J]
Bussières AE, Stewart G, Al-Zoubi F, et al. Spinal manipulative therapy and other conservative treatments for low back pain: a guideline from the Canadian Chiropractic Guideline Initiative. J Manip Physiol Ther. 2018;41:265–93.
Côté P, Yu H, Shearer HM, et al. Non-pharmacological management of persistent headaches associated with neck pain: a clinical practice guideline from the Ontario protocol for traffic injury management (OPTIMa) collaboration. Eur J Pain. 2019;23:1051–70.
Côté P, Wong JJ, Sutton D, et al. Management of neck pain and associated disorders: A clinical practice guideline from the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Eur Spine J. 2016;25:2000–22.
Bussières AE, Stewart G, Al-Zoubi F, et al. The Treatment of Neck Pain–Associated Disorders and Whiplash-Associated Disorders: A Clinical Practice Guideline. J Manipulative Physiol Ther. 2016;39(8):523–64.e27.
Task Force on the Low Back Pain Clinical Practice Guidelines. American Osteopathic Association Guidelines for Osteopathic Manipulative Treatment (OMT) for Patients With Low Back Pain. J Am Osteopath Assoc .2016;110:653-666.
Mao JJ, Ismaila N, Bao T, et al. Integrative Medicine for Pain Management in Oncology: Society for Integrative Oncology-ASCO Guideline. J Clin Oncol. 2022;34:3998–4024.
Deng GE, Rausch SM, Jones LW, et al. Complementary therapies and integrative medicine in lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143:e420S–e36S.
Burnett M, Lemyre M. 345-Primary Dysmenorrhea Consensus Guideline. J Obstet Gynaecol Can. 2017;39:585–95.
Guy SD, Mehta S, Casalino A, et al. The can pain SCI clinical practice guidelines for rehabilitation management of neuropathic pain after spinal cord: recommendations for treatment. Spinal Cord. 2016;54:S14–23.
Professional Committee of Spine Medicine of Chinese Association of Integrated Traditional and Western Medicine, Tan MS, Atul G, Kuniyoshi A, et al. Clinical practice guideline of integrated traditional Chinese and western medicine:atlantoaxial dislocation (AAD) (2019). Zhongguo Gu Shang. 2020;33:27–37. Chinese
Orthopedics and Traumatology Branch, China Association of Chinese Medicine. Clinical guidelines for diagnosis and treatment of scapulohumeral periarthritis in traditional Chinese medicine orthopedics and traumatology:T/CACM 1179—2019. Shanghai J Tradit Chin Med. 2022;56:1–5. Chinese
Globe G, Farabaugh RJ, Hawk C, et al. Clinical practice guideline: chiropractic care for low back pain. J Manip Physiol Ther. 2016;39:1–22.
Bryans R, Descarreaux M, Duranleau M, et al. Evidence-based guidelines for the chiropractic treatment of adults with headache. J Manip Physiol Ther. 2011;34:274–89.
Brosseau L, Wells GA, Tugwell P, et al. Ottawa Panel evidence-based clinical practice guidelines on therapeutic massage for neck pain. J Bodyw Mov Ther. 2012;16:300–25.
Chen Z, Wu C, Wang J. Practical guideline for preventive treatment of disease in traditional Chinese medicine·infantile constitution of spleen insufficiency intervened by Tuina ( formulation). Hebei J TCM. 2017;39:339–42. Chinese
Hawk C, Whalen W, Farabaugh RJ, et al. Best practices for chiropractic management of patients with chronic musculoskeletal pain: a clinical practice guideline. J Altern Complement Med. 2020;26:884–901.
Bryans R, Decina P, Descarreaux M, et al. Evidence-based guidelines for the chiropractic treatment of adults with neck pain. J Manip Physiol Ther. 2014;37:42–63.
National Institute for Health and Care Excellence. Liposuction for chronic lymphoedema. Available from:www.nice.org.uk/guidance/ipg723.
National Institute for Health and Care Excellence. Liposuction for chronic lipoedema. Available from: https://www.nice.org.uk/guidance/ipg721.
Devlin J, Duprey M, Skrobik Y, et al. ICU sleep management practices across 6 states prior to 2018 SCCM PADIS practice guideline release. Crit Care Med. 2019;47(1 Supplement):1.
Jfa B, Ntac D, Mfc E, et al. A clinician's guide to the management of geriatric musculoskeletal disease: part 1 - osteoporosis. Int J Osteopath Med. 2022;43:53–62.
Abdulla A, Adams N, Bone M, et al. British Geriatric Society. Guidance on the management of pain in older people. Age Ageing. 2013;42(Suppl 1):i1–57.
Shirado O, Arai Y, Iguchi T, et al. Structured abstract preparation team. Formulation of Japanese Orthopaedic Association (JOA) clinical practice guideline for the management of low back pain- the revised 2019 edition. J Orthop Sci. 2022;(27):3–30.
National Institute for Health and Care Excellence. Otitis media with effusion in under 12s: surgery. Available from: www.nice.org.uk/guidance/cg60.
National Institute for Health and Care Excellence. Low back pain and sciatica in over 16s: assessment and management. Available from: www.nice.org.uk/guidance/ng59.
Qaseem A, Mc Lean RM, O’Gurek D, et al. Clinical Guidelines Committee of the American College of Physicians; Commission on Health of the Public and Science of the American Academy of Family Physicians; Cooney TG, Forciea MA, Crandall CJ, et al. Nonpharmacologic and Pharmacologic Management of Acute Pain From Non-Low Back, Musculoskeletal Injuries in Adults: A Clinical Guideline From the American College of Physicians and American Academy of Family Physicians. Ann Intern Med .2020;173:739-748.
Li J, Tang L, Ma X. Chinese rehabilitation guidelines for cerebral palsy (2022):introduction. Chinese Journal of Applied Clinical Pediatrics. 2022;37:885–6.
Hui D, Bohlke K, Bao T, et al. Management of Dyspnea in Advanced Cancer: ASCO Guideline. J Clin Oncol. 2021;39:1389–411.
2018 surveillance of otitis media with effusion in under 12s: surgery (NICE guideline CG60) [Internet]. London: National Institute for Health and Care Excellence (NICE); 2018.
National Institute for Health and Care Excellence. Atopic eczema in under 12s: diagnosis and management. Available from: www.nice.org.uk/guidance/cg57.
National Guideline Centre (UK). Low back pain and sciatica in over 16s: assessment and management. London: National Institute for Health and Care Excellence (NICE); 2016.
Airaksinen O, Brox JI, Cedraschi C, et al. COST B13 Working Group on Guidelines for Chronic Low Back Pain. Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006;15:S192–300.
Ng JY, Liang L, Gagliardi AR. The quantity and quality of complementary and alternative medicine clinical practice guidelines on herbal medicines, acupuncture and spinal manipulation: systematic review and assessment using AGREE II. BMC Complement Altern Med. 2016;16:425.
Tan JB, Zhai J, Wang T, et al. Self-managed non-pharmacological interventions for breast cancer survivors: systematic quality appraisal and content analysis of clinical practice guidelines. Front Oncol. 2022;12:866284.
Would Health Organization. WHO handbook for guideline development:second edition [EB/OL].(2014-12-18, 2022-02-22]. Available from: https://apps.who.int/medicinedocs/en/m/abstract/Js22083en/.
Brouwers MC, Florez ID, McNair SA, et al. Clinical Practice Guidelines: Tools to Support High Quality Patient Care. Semin Nucl Med. 2019;49(2):145–52.
Abdellatif HM, Al-Muallem A, Almansoof AS, et al. Clinical Practice Guidelines in an Era of Accountability, Saudi Arabia: A Call for Action. J Epidemiol Glob Health. 2023;13(3):391–6.
Amri MM, Abed SA. The Data-Driven Future of Healthcare: A Review. Mesopotamian Journal of Big Data. 2023:68–74.
Acknowledgements
None.
Funding
This study was supported by the State Key Laboratory of Dampness Syndrome of Chinese Medicine (No. SZ2021ZZ30/SZ2021ZZ3004); the Guangdong Provincial Key Laboratory of Clinical Research on Traditional Chinese Medicine Syndrome (No. ZH2019ZZ04); Wang Lixin Academic Experience Inheritance Studio of Guangdong Provincial Hospital of Chinese Medicine.
Author information
Authors and Affiliations
Contributions
Mingyue Fan and Darong Wu contributed to the conception and designed the work. Mingyue Fan developed search strategy. Mingyue Fan, Aolin Liu, and Bingqing Liu selected the massage-related CPGs/consensus. Xiaowen Zhou, Mingyue Fan, and Chen Tian assessed for Guideline quality. Aolin Liu conducted the data analysis. Mingyue Fan and Xiaowen Zhou drafted the initial manuscript. Darong Wu and Taoying Lu critically revised the manuscript. Long Ge, Qianwen Xie, Jianxiong Cai, and Lingjia Yin provided the technical support for the study. All the authors participated in the study and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no financial interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix 1.
Detailed construction of CPGs/consensus search strategies.
Additional file 2: Appendix 2.
Characteristics of guidelines concerning the contents of rigor of development.
Additional file 3: Appendix 3.
The AGREE II scores of each eligible CPGs/consensus.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fan, M., Liu, A., Lu, T. et al. Quality appraisal of clinical practice guidelines addressing massage interventions using the AGREE II instrument. Syst Rev 13, 83 (2024). https://doi.org/10.1186/s13643-024-02503-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-024-02503-6