
Abstract
Background
The inhabitants of western Sudan use traditional medicine for the treatment of various ailments due to lack of medical doctors and unaffordable prices of pharmaceutical products. The present study is the first documentation of the traditional plant knowledge on medicinal uses of plants by healers in Algoz (South Kordofan), Sudan.
Method
Ethnobotanical data were collected over a period from March to November 2015 using semi-structured interviews with 30 healers (24 male and 6 female) living in the investigated area. Quantitative indices such as use categories, use value (UV) and informant consensus factor (ICF) were intended to evaluate the importance of medicinal plant species.
Results
A total of 94 medicinal plants, which belong to 45 families and 81 genera, were recorded in the study area. The most represented families are Leguminosae with 20 species followed by Combretaceae (6 species), Rubiaceae (5 species) and Asteraceae (4 species). The reported species were belonging to herbs (43%), trees (28%), shrubs (22%), climbers (4%) and parasites (3%). Root and stem (21% each) were the most plant parts used. A majority of remedies are administered orally (67%) where infusion (36%) and maceration (32%) are the most used methods. The highest ICF (0.87) was reported for poisonous animal bites followed by urinary system diseases (0.89), blood system disorders (0.88) and gynaecological diseases (0.87). Anastatica hierochuntica, Ctenolepis cerasiformis, Echinops longifolius, Cleome gynandra, Maerua pseudopetalosa, Martynia annua, Oldenlandia uniflora, Opuntia ficus-indica, Solanum dubium, Sonchus cornutus, Tribulus terrestris and Drimia maritima were reported for the first time in this study.
Conclusion
The number of medicinal plants reported in this paper reflects evidence that Algoz area had a high diversity of medicinal plants which will continue to play an important role in the healthcare system in the study area.
Similar content being viewed by others


Background
In 2011, Sudan split into two countries with one third of the country being proclaimed a new state named “Republic of South Sudan” leaving behind the remaining area retaining the older name “the Republic of Sudan” [1]. In its former integral state, Sudan was the largest country in Africa and the tenth in the world, boasting an area of 2.5 million square kilometers which spanned diverse terrains and climatic zones [1]. This did bear directly on the wide diversity of vegetation, from those in the desert and semi-desert in the north through the equatorial in the central part to the extreme of the humid equatorial in the south. Such prevailing conditions favoured diverse vegetation consisting of 3137 documented species of flowering plants belonging to 170 families and 1280 genera, 15% of which are endemic [2]. A large number of these plants have a vital contribution to human health care needs throughout the country. Medicinal and aromatic plants and their derivatives represent an integral part of life in Sudan. Communities in different regions of Sudan use traditional medicine for the treatment of various ailments due to lack of medical doctors and unaffordable prices of pharmaceutical products beside their faith on the medicinal values of traditional medicine [3]. It has been estimated that only 11% of the population has access to formal health care [1].
The geographical position of Sudan represents a multicultural melting pot of diverse traditional knowledge over large distances and facilitated the exchange of knowledge about medicinal plants with other countries from Africa to Middle East and Asia [4].
Despite the varied flora and socio-cultural diversity in Sudan, there is a far-reaching lack of written information on the traditional use of medicinal plants [4]. So, documentation of plants used as traditional medicines in Sudan is warranted. The aim of this study was to investigate the traditional plant knowledge on medicinal uses of plants by local healers in Algoz area (South Kordofan), Sudan.
Methods
Study area
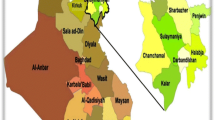
Algoz area is situated in the northern part of South Kordofan state, and its borders are Northern Kordofan state from the north and northeast, West Kordofan state from the northwest, Dellang locality from the south and Habella locality from the southeast direction (Fig. 1). It is located between latitudes 12°–12° 30 N and longitudes 29° 48–300 E and 622 m above sea level, with a total area of 35,000 km2. Short grass and short scattered trees prevail. The area is associated with exposed rocks crossing the central Sudan forming a surface water divide. The White Nile which is the main tributary of the River Nile bounds the hydrologic system to the east, while the highlands of Kordofan Plateau and the Nuba Mountains bound it to the west and the south respectively. Khor Abu Habil is a major seasonal wadi that crosses the study area and flows from the west to the east. The wadi disappears into the sand dunes a few kilometers before reaching the White Nile. The climate in the area is semi-arid with long hot summers (March–September) and short mild winters (December–February). Seasonal rainfall occurs only during summer (June–September) and varies between 200 mm/year in the north and 450 mm/year in the south [5].

a Sudan map showing the South Kordofan State (red) and b Algoz locality (red)
Algoz area has a multi-population with tribes as Dar Shungool, Gaboosh, Dar Bati, Albargo, Albarno, Flata and some Arabic nomads. They are working mainly in agriculture, animal grazing and trade [6].
Data collection and plant identification
Ethnobotanical data were collected from March to November 2015. Information about the medicinal use of plants was collected by carrying out semi-structured interviews with 30 healers (24 male and 6 female) living in the investigated area. The questionnaire was designed to collect data on (i) local names of the plants, (ii) ailments treated by the plant, (iii) plant parts used, (iv) condition of the plant material (dried or fresh) and (v) modes of preparation and administration. Some social factors like the name, age, occupation and education level of the interviewed person were also recorded. Also, the geographic locality and date of the interview were recorded. Plant specimens were collected for taxonomic identification using keys of written floras such as Broun and Massey [7], Andrews [8,9,10,11], Ross [12], Hutchinson and Dalziel [13], Maydell [14] and Elamin [15]. Voucher specimens were deposited at the Herbarium of Institute of Medicinal and Aromatic Plants, National Centre for Research, Sudan (MAPTMR-H). The botanical names and plant families are given according to the standards of the plant list (www.ipni.org/).
Ethnobotanical data analysis
Data analysis was carried out by using both the classical ethnobotanical systematic investigation and a numerical quantitative approach in order to evaluate the importance of the mentioned plant species in the investigated area. The quantitative study was carried out by calculating the following ethnobotanical indices:
Use categories
The medicinal plant uses were classified into categories following the standard developed by Cook [16]. Each time a plant was mentioned as “used” was considered as one “use report”. If one informant used a plant to treat more than one disease in the same category, it was considered as a single use report [17].
Use value (UV)
The relative importance was calculated employing the use value [18], a quantitative measure for the relative importance of species known locally:
where Ui is the number of use reports cited by each informant for a given species and n refers to the total number of informants.
Use values are high when there are many use reports for a plant, implying that the plant is important, and approach zero (0) when there are few reports related to its use. The use value, however, does not distinguish whether a plant is used for single or multiple purposes.
Informant consensus factor
To test homogeneity of knowledge, the informant consensus factor was used [19]:
where Nur refers to the number of use reports for a particular use category and Nt refers to the number of taxa used for a particular use category by all informants. Informant consensus factor (ICF) values are low (near 0) if plants are chosen randomly or if there is no exchange of information about their use among informants and approach one (1) when there is a well-defined selection criterion in the community and/or if information is exchanged between informants [20].
Results
Medicinal plant diversity
A total of 94 medicinal plants, which belong to 45 families and 81 genera, were recorded in the study area. Results provide the following information for each species: scientific name, botanical family, local common name, plant habitat, plant part used, disease treated, route of administration and use value (Table 1). The most represented families are Leguminosae with 20 species followed by Combretaceae (6 species), Rubiaceae (5 species), Asteraceae (4 species), Lamiaceae, Poaceae, Tiliaceae and Zygophyllaceae (3 species each), Apocynaceae, Asclepiadaceae, Brassicaceae, Burseraceae, Cleomaceae, Capparaceae, Malvaceae and Meliaceae (2 species each), and other families were represented with one species each. This dominance of Leguminosae plants is a characteristic of the Sudan flora. The most commonly used species is Sarcocephalus latifolius with a UV of 2.07 followed by Guiera senegalensis with a UV of 1.87, Hydnora abyssinica with a UV of 1.83 and Geigeria alata with a UV of 1.67 respectively. Plants that treat three ailments and more (86%) represent the majority, followed by plants that treat single ailments (8%) and those that treat two ailments (6%) respectively.
Habitat of the plants
Analysis of data based on their habitat showed that the reported species belong to herbs (43%), trees (28%), shrubs (22%), climbers (4%) and parasites (3%) (Fig. 2). The majority of medicinal plants are collected from the wild, and only 11% are cultivated or purchased (0.01%) from the market (Table 1).

Habitat of medicinal plants in the study area
Parts of medicinal plants used
Data on different plant parts used in traditional medicine are indicated in Fig. 3. Those that are used the most were the root and stem (21% each) followed by the fruit (15%), whole plant (14%), seed (12%), leaf (11%), gum/latex, bulb/corm and heartwood (0.02%) and flower (0.01%) respectively. There are cases where different parts of the same plant are being used for the treatment of different diseases.

Percentage of plant parts used
Method of preparation
A majority of remedies are administered orally (67%) where infusion (36%) and maceration (32%) are the most used methods. Some prescriptions can be prepared by both methods: infusion or maceration represented 13%, while decoction represented 11% of preparations. Dried powder or freshly collected plant parts are also used. Other prescriptions are used externally (33%) and applied as dry powder (29%), rub (23%), smoke (23%), poultices (20%) or as a wash (6%) (Table 2). Most of these preparations use water as a solvent extractor. Some herbalists used other adjuvants like honey, sugar, salt, milk, sour milk, yoghurt, ajeen (fermented dough), nisha (light porridge), atroon (sodium bicarbonate), bee wax, wax of goat and olive and sesame oil.
Medicinal plants used in combination
For the treatment of particular ailment, sometimes herbalists used more than one plant. For example, Allium sativum bulb is mixed with Zingiber officinale rhizome and applied to the anus for the treatment of haemorrhoids. A potion is prepared from the seed of Trigonella foenum-graecum, curcuma, Negilla sativa and bee honey for the treatment of uterus inflammation. Root of Tinospora bakis is mixed with Syzygium aromaticum (clove) for the treatment of malaria. Atroon is added to some preparations like those of Ziziphus spina-christi and Acacia oerfota for the treatment of dysentery and toothache respectively.
Quantitative analyses of ethnomedicinal data
Informant consensus factor
Fifteen ailment categories were identified. The ICF was calculated for each ailment category, and the range was from 0.50 to 0.91 (Table 3). The highest ICF (0.91) was reported for poisonous animal bites with 8 species and 77 use reports, followed by urinary system diseases (0.89) with 17 species and 156 use reports, blood system disorders (0.88) with 14 species and 116 use reports and gynaecological diseases (0.87) with 12 species and 86 use reports. The highest ICF for poisonous animal bites can be probably related to the hard and dangerous environmental conditions. The category of plants used for treatment of eye diseases has the lowest degree of consensus (0.50) where only three informants mentioned ailments in this category.
Most frequently cited plant species and medicinal uses
In this study, the most cited plants, those that had at least 20 or more citations for specific ailment, were Guiera senegalensis (57 citations) mainly used for the treatment of malaria (22 citations) and kidney disorders (20 citations). This is followed by Hydnora abyssinica (55 citations) used in the treatment of gastrointestinal system diseases (mainly for diarrhoea and dysentery (40 citations), Geigeria alata (50 citations) used mainly for the treatment of diabetes (20 citations) and hypertension (17 citations), Kigelia africana (32 citations) with 28 citations for the treatment of breast swellings and Carissa spinarum (28 citations) for envy eye.
Medicinal plants and the associated knowledge
Thirty healers (24 male and 6 female) were interviewed and divided into five different age groups (20–30, 31–40, 41–50, 51–60 and > 60). Analysis of the result on ages of healers revealed that the most dominant age of men is 41–50 while for women which were few in number is > 60 (Figs. 3 and 4).

Age group distribution of the traditional healers interviewed
Discussion
In this study, the most cited plants, Guiera senegalensis, Hydnora abyssinica, Geigeria alata, Kigelia africana and Carissa spinarum, were previously reported with the same traditional uses in ethnobotanical studies from other regions of Sudan. For example, Guiera senegalensis was reported by EL-Kamali [3] and Suleiman [21] for the treatment of malaria. Hydnora abyssinica (H. johannis) for the treatment of diarrhoea and dysentery and Kigelia africana for the treatment of breast swellings were also reported by Musa et al. [22]. Geigeria alata for the treatment of diabetes was reported by EL-Kamali [3] and Suleiman [21]. Carissa spinarum (C. edulis) was reported by EL-Kamali [3] for charm and the treatment of madness. Kigelia africana was reported by Doka and Yagi [23] for swollen mastitis.
The high frequency of citations of medicinal plants can be explained by the fact that these plants are the best known and have long been used by the majority of informants, representing a source of reliability. In fact, many biological activity and phytochemical evaluation were carried out for these plants. For example, Traore-Keita et al. [24] reported that the chloroform extract of roots of Guiera senegalensis exhibited a pronounced antimalarial activity. They isolated two alkaloids, namely, harman and tetrahydroharman, that displayed high antimalarial activity (IC50 (50% inhibition) lower than 4 μg/mL) and low toxicity against human leukemia monocytic cell line (THP1). Yagi et al. [25] found that Hydnora johannis roots have no activity against bacteria spp. that are mainly responsible of diarrhoea but are rich in phenols. They suggested that the curing potency of the roots of H. johannis was not mainly associated with the presence of antibacterial activity agent(s) against bacterial species responsible of dysentery or diarrhoea but might be attributed to the role of tannins in reducing the effect through denaturing the proteins by the formation of protein tannate, thereby causing the intestinal mucosa to become more resistant, reducing the intestinal transit and by acting as a barrier against toxin exerted by bacteria. The antidiabetic potential of Geigeria alata root was evaluated, and diabetic rats dosed with 250 mg/kg of aqueous methanolic extract were found to have significantly (p < 0.05) decreased blood glucose level closer to that of non-diabetic rats and improved β-cell function and antioxidant status [26]. Kigelia africana was found to suppress the breast MCF7 [27], human colon adenocarcinoma (Caco-2), human embryonic kidney (HEK-293) [28] and HeLa cervical cancer cell proliferation [29].
Comparative review of traditional usages of reported species with previous studies from Sudan
A comparative review with previous reports [3, 21,22,23, 30,31,32,33] from different parts of Sudan was performed to identify the new medicinal plants and new uses reported in this study (Table 4). The plants reported by Suleiman [21] for traditional plants used by communities of Northern Kordofan region included a total of 44 plant species with 22 species with same traditional uses which were reported also in this study, while 2 species, Blepharis linariifolia and Catunaregam nilotica (Xeromphis nilotica, Randia nilotica), were reported with different uses. EL-Kamali [3] reported 48 plant species for traditional plant uses in North Kordofan too with 15 species with same traditional uses which were reported also in this study and 5 species, Acacia nilotica subsp. adstringens, Aristolochia bracteolate, Cissus quadrangularis, Dichrostachys cinerea and Sarcocephalus latifolius (Nauclea latifolia), with different uses. Doka and Yagi [23] reported 49 plant species for traditional plant uses in West Kordofan with 16 species with same traditional uses which were reported also in this study, and 9 species were reported in this study with different uses; these included Acacia senegal, Acacia seyal, Arachis hypogaea, Balanites aegyptiaca, Cissus quadrangularis, Combretum aculeatum, Grewia flavescens, Tamarindus indica and Catunaregam nilotica. Musa et al. [22] reported 53 plant species for traditional plant uses in the Blue Nile State, southeastern Sudan, with 18 species with same traditional uses which were reported in this study and 13 species with different uses: Acacia senegal, Acacia seyal, Anogeissus leiocarpus, Carissa spinarum (C. edulis), Cissus quadrangularis, Grewia villosa, Lannea fruticose, Piliostigma reticulatum, Senna occidentalis, Strychnos spinose, Tephrosia uniflora, Terminalia laxiflora and Ximenia americana. Moreover, El Ghazali et al. [30,31,32,33] in their books of Sudanese medicinal plants documented some of these plants for the same or very similar usages. In fact, there are 99 new traditional uses for some previously reported medicinal plants. For example, the whole plant of Striga hermonthica was previously reported to treat diabetes, but in this study, it is used also for menstrual cramps. The fruit of Senna occidentalis is reported to treat eczema beside its common use as a laxative. Plicosepalus acaciae is commonly used to enhance wound healing and as a lactagogue, but in this study, the smoke fumigant of the seeds is reported to repel insect from ear.
New species and new uses for species are reported for the first time in this study. For example, Anastatica hierochuntica, Ctenolepis cerasiformis, Echinops longifolius, Cleome gynandra, Maerua pseudopetalosa, Martynia annua, Oldenlandia uniflora, Opuntia ficus-indica, Solanum dubium, Sonchus cornutus, Tribulus terrestris and Drimia maritima were not being mentioned in any previous study for the traditional Sudanese medicine. Acanthorrhinum ramosissimum, Cleome viscosa and Setaria acromelaena which were used for evil eye were also reported for the first time.
The majorities of the healers declared that they had learned about medicinal plants from their parents or grandparents. The lack of systematic documentation for medicinal plant knowledge which appears to occur in many parts of the world may contribute to the loss of this knowledge, particularly for plants that are neglected or non-preferred [34,35,36].
Conclusion
The number of medicinal plants reported in this paper reflects evidence that the Algoz area harbours a high diversity of medicinal plants that will continue to play an important role in the healthcare system in the study area. Evaluation of their claimed pharmacological potential efficacy and toxicity profile is essential. Moreover, the present study could contribute in conserving such rich heritage and providing precious information as a contribution through writing the Sudanese pharmacopeia.
Conservation of this traditional knowledge is very important. The progressing mass destruction of wild vegetation for various purposes may accelerate the disappearance of medicinal plants. This in turn may have profound consequences on the roles of traditional medicine on human health. Furthermore, the drop in the availability of raw materials due to the depletion of natural resources affects the discovery of potential drugs [37]. Thus, raising community awareness about conservation and sustainable utilization of the traditional medicinal plants is a vital part for the entire plant biodiversity [22]. Modern biotechnical approaches like genetic engineering, micropropagation via tissue encapsulation of propagules, tissue culture and fermentation should be applied to improve yield and modify the potency of medicinal plants [38].
Abbreviations
- ICF:
-
Informant consensus factor
- UV:
-
Use value
References
Mohammed AMA. Research advances in Sudanese traditional medicine: opportunities, constrains and challenges. Altern Integ Med. 2013;2:10.
Khalid H, Abdalla WE, Abdelgadir H. Gems from traditional north-African medicine: medicinal and aromatic plants from Sudan. Nat Prod Bioprospect. 2012;2:92–103.
EL-Kamali HH. Ethnopharmacology of medicinal plants used in north Kordofan (western Sudan). Ethnobot Leaflets. 2009;13:89–97.
Saeed MEM, Abdelgadir H, Sugimoto Y, Khalid HE, Efferth T. Cytotoxicity of 35 medicinal plants from Sudan towards sensitive and multidrug-resistant cancer cells. J Ethnopharmacol. 2015;174:644–58.
Abdalla OAE. Aquifer systems in Kordofan, Sudan: subsurface lithological model. S Afr J Geol. 2006;109:585–98.
Anonym. South Kordofan State, Sudan Ministry of the Cabinet Affairs, 2016 (In Arabic).
Broun AF, Massey RE. Flora of the Sudan. Thomas Murby and Co 1. Fleet Lane, London, E.C. 4. El, 1929.
Andrews FW. The vegetation of the Sudan. In: Tot till JD, editor. Agriculture in the Sudan. UK: Oxford University Press; 1948.
Andrews FW. The flowering plants of the Anglo-Egyptian Sudan, vol. 1. Arbroath: Buncle Co. Ltd.; 1950.
Andrews FW. The flowering plants of the Anglo-Egyptian Sudan, vol. 2. Arbroath: Buncle Co. Ltd.; 1952.
Andrews FW. The flowering plants of the Anglo-Egyptian Sudan, vol. 3. Arbroath: Buncle Co. Ltd.; 1956.
Ross JH. Flora of South Africa. In: Part I. The government printer Pretoria, vol. 16; 1975.
Hutchinson J, Dalziel JM. Flora of west tropical Africa. 1st ed. Millbank: Crown Agents for Overseas Governments and Administration; 1968.
Maydell HJV. Trees and shrubs of the Sahel, their characteristics and uses. Germany: GTZ; 1990.
Elamin HM. Trees and shrubs of the Sudan. U.K: Ithaca Press Exeter; 1990.
Cook FEM. Economic botany data collection standard. Kew: Royal Botanic Gardens; 1995.
Treyvaud AV, Arnason JT, Maquin P, Cal V, Vindas PS, Poveda L. A consensus ethnobotany of the Q‘eqchi’ Maya of southern Belize. Econ Bot. 2005;59:29–42.
Phillips O, Gentry AH, Reynel C, Wilkin P, Galvez DBC. Quantitative ethnobotany and Amazonian conservation. Conserv Biol. 1994;8:225–48.
Trotter RT, Logan MH. Informant consensus: a new approach for identifying potentially effective medicinal plants. In: Etkin NL, editor. Plants in indigenous medicine and diet. Bedford Hills: Redgrave Publishing Company; 1986.
Gazzaneo LRS, Lucena RFP, Albuquerque UP. Knowledge and use of medicinal plants by local specialists in a region of Atlantic Forest in the state of Pernambuco (Northeastern Brazil). J Ethnobiol Ethnomed. 2005;1:9.
Suleiman MHA. An ethnobotanical survey of medicinal plants used by communities of Northern Kordofan region, Sudan. J Ethnopharmacol. 2015;176:232–42.
Musa MS, Abdelrasoo FE, Elsheikh EA, Ahmed LAMN, Mahmoud AE, Yagi SM. Ethnobotanical study of medicinal plants in the Blue Nile State, south-eastern Sudan. J Med Plant Res. 2011;5(17):4287–97.
Doka IG, Yagi SM. Ethnobotanical survey of medicinal plants in west Kordofan (western Sudan). Ethnobot Leaflets. 2009;13:1409–16.
Traore-Keita F, Gasquet M, Di Giorgio C, Ollivier E, Delmas F, Keita A, Doumbo O, Balansard G, Timon-David P. Antimalarial activity of extracts and alkaloids isolated from six plants used in traditional medicine in Mali and Sao Tome. Phytother Res. 2002;16(7):646–9.
Yagi S, Chrétien F, Duval RE, Fontanay S, Maldini M, Henry M, Chapleur Y, Laurain-Mattar D. Antibacterial activity, cytotoxicity property and chemical constituents of Hydnora johannis roots. South Afr J Bot. 2012;78:228–34.
Hafizur RM, Babiker R, Yagi S, Chishti S, Kabir N, Choudhary MI. The antidiabetic effect of Geigeria alata is mediated by enhanced insulin secretion, modulation of β-cell function, and improvement of antioxidant activity in streptozotocin-induced diabetic rats. J Endocrinol. 2012;214:329–35.
Fouche G, Cragg GM, Pillay P, Kolesnikova N, Maharaj VJ, Senabe J. In vitro anticancer screening of South African plants. J Ethnopharmacol. 2008;119(3):455–61.
Chivandi E, Cave E, Davidson BC, Eriwanger KH, Mayo D, Madziva MT. Suppression of Caco-2 and HEK-293 cell proliferation by Kigelia africana, Mimusops zeyheri and Ximenia caffra seed oils. In Vivo. 2012;26(1):99–105.
Arkhipov A, Sirdaarta J, Rayan P, McDonnell PA, Cock IE. An examination of the antibacterial, antifungal, antigiardial and anticancer properties of Kigelia africana fruit extracts. Pharmacognosy Commun. 2014;4(3):62–76.
El Ghazali GB. Medicinal plants of the Sudan. Part I. Medicinal plants of Arkawit. Sudan: Khartoum University Press; 1987.
El Ghazali GB, El Tohami MS, El Egami AB. Medicinal plants of the Sudan. Part III. Medicinal plants of the White Nile Province. Sudan: Khartoum University Press; 1994.
El Ghazali GB, El Tohami MS, El Egami AB, Abdalla WS, Mohamed MG. Medicinal plants of the Sudan. Part IV. Medicinal plants of Northern Kordofan. Khartoum: Omdurman Islamic University Press; 1997.
El Ghazali GE, Aballa WE, Khalid HE, Khalafalla MM, Hamad AD. Medicinal plants of the Sudan, Part V. Medicinal plants of Ingessana. Khartoum: Sudan Currency Printing Press; 2003.
Fekadu F. Ethiopian traditional medicine, common medicinal plants in perspective, Sioux City, IA, (2001).
Brouwer N, Liu Q, Harrington D, Kohen J, Vemulpad S, Jamie J, Randall M, Randall D. An ethnopharmacological study of medicinal plants in New South Wales. Molecules. 2005;10:1252–62.
Bussmann RW, Sharon D. Traditional medicinal plant use in Loja province, southern Ecuador. J Ethnobiol Ethnomed. 2006;2:44.
Chivian E. Biodiversity: its importance to human health center for health and the global environment. USA: Harvard Medical School; 2002.
Chen S-L, Yu H, Luo H-M, Wu Q, Li C-F, Steinmetz A. Conservation and sustainable use of medicinal plants: problems, progress, and prospects. Chin Med. 2016;11:37.
Acknowledgements
We would like to thank all the traditional healers and local people of the study area for sharing their knowledge, cooperation and hospitality. The authors are grateful to Dr. Migdad Elsir Shuaib (Department of Geology, Faculty of Science, University of Khartoum) for the geographical and geological information.
Funding
This study was financed by the University of Bahri, Sudan, Code No: U of B-1-2015.
Availability of data and materials
We have already included all data in the manuscript collected during the field surveys.
Author information
Authors and Affiliations
Contributions
TOI and YS conducted the field survey and collected the data, SY did the analysis and wrote the first draft of the manuscript, RHA and TMN provided support in sampling and plant species identification, AMM provided technical support and helped in the write-up and revision and TOK designed the study and supervised the project. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
The present study is purely based on filed survey instead of human or animal trails.
Ethical guidelines of the International Society of Ethnobiology (http://www.ethnobiology.net/) were strictly followed.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Issa, T.O., Mohamed, Y.S., Yagi, S. et al. Ethnobotanical investigation on medicinal plants in Algoz area (South Kordofan), Sudan. J Ethnobiology Ethnomedicine 14, 31 (2018). https://doi.org/10.1186/s13002-018-0230-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13002-018-0230-y