
Abstract
Background
The global spread of coronavirus has caused many physical and mental health problems throughout the world. Depression and anxiety are among the issues that people are experiencing abundantly, along with other mental health disorders, during this period. Cognitive behavior therapy (CBT) is one of the approaches that is effective on improving most of the psychological issues including depression and anxiety. The objective of this systematic review and meta-analysis was to assess the effects of CBT on depression and anxiety during COVID-19 pandemic period.
Methods
English databases such as Cochrane, PubMed, Google Scholar, Web of Science and Persian databases such as SID, MagIran and IranDoc were searched with a time limit of 2019 to 2022. Two researchers independently evaluated the quality of the entered studies based on Cochrane handbook. Subgroup analysis was conducted separately on the basis of being infected with coronavirus, not being infected with coronavirus, and having a history of depression or anxiety before the intervention and internet-based CBT for depression and anxiety. Meta-analysis results were reported using standardized mean difference (SMD) and 95% confidence interval (95% CI). Heterogeneity of studies was analyzed by means of I2 index; and in the case of heterogeneity presence, random effects model was used instead of fixed effects model. Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used for evaluating the quality of evidence.
Results
Totally, 2015 articles were analyzed of which 11 articles entered meta-analysis. The overall results of meta-analysis showed that mean score of anxiety in the group receiving CBT was significantly lower than the control group (SMD: − 0.95, 95% CI − 1.29 to − 0.62; P < 0.00001, I2 = 94%). In addition, mean score of depression in the intervention group was significantly lower than the control group (SMD: − 0.58; 95% CI − 1.00 to − 0.16, P < 0.00001, I2 = 94%). In addition, the results of subgroup meta-analysis showed that internet-based CBT was effective in reducing of depression (SMD − 0.35; 95% CI − 0.50 to − 0.20; P < 0.00001; I2 = 0%) and anxiety (SMD − 0.90; 95%CI − 1.47 to − 0.33; P = 0.002; I2 = 94%). The evidence about the effectiveness of CBT on depression and anxiety compared with control group on the basis of GRADE approach had low quality.
Conclusions
Meta-analysis results showed that CBT reduced the mean scores of anxiety and depression significantly during COVID-19 pandemic period. Due to the low quality of evidence, conducting more randomized controlled trials with rigorous design is suggested.
Prospero registration This systematic review has been registered in Prospero (ID: CRD42021277213).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The worldwide outbreak of coronavirus pandemic since 2019 became a very serious crisis for all people and posed many challenges for world health community as well as research and medical committees [1]. Presently, people from all age groups including children to adults and people with any health background are at risk of coronavirus infection, so that by August 25, 2021, more than 214,000,000 people in the world were infected with the virus of whom more than 4,470,000 people lost their lives [2].
Although a lot of attention is paid to coronavirus pandemic, and its news and information are broadcasted moment by moment, the attention is just paid to the pathogenic aspect of coronavirus, while its psychological effects on society are neglected most of the time [3]. Each traumatic event may reduce people’s sense of security and affect their mental health negatively. Being exposed to coronavirus news and unanswered questions about when the pandemic ends and what its treatments are, along with decreased social relations and widespread quarantines all have negative effects on people’s mental health [3, 4]. Moreover, decline of some people’s income because of widespread lockdowns disrupts families’ well-being and affects their quality of life and consequently their mental health negatively [5]. Extremely rapid transmission and high mortality rate of this disease lead to psychological problems or worsen the former problems in people [6]. Some symptoms such as anxiety, depression, fear, stress, and insomnia are very common during coronavirus pandemic [3].
Depression is a common disorder that presently affects nearly 120 million people all over the world and its prevalence rate is between 10% and 15% in a lifetime according to epidemiological surveys [7]. Anxiety is also another common mental disorder. Mental disorders, according to WHO, account for 30% of nonfatal illnesses and it is estimated that 1 in 5 persons are exposed to anxiety and depression in critical conditions [8]. A study conducted in China showed that prevalence of depression and anxiety increased significantly among general population during COVID-19 crisis [9].
Since COVID-19 pandemic has a lot of implications for personal, social, and emotional health; emotional and social needs of people during this period should receive enough attention from providers of these services and health policy makers, in addition to medical services [10]. Cognitive behavior therapy (CBT) is a psychological therapeutic approach that is extensively used both as a prevention and a treatment method for both medical staff and general population [11]. CBT is a set of methods including cognitive restructuring and behavioral change that helps people control their stress, change their negative behavior and attitudes and, likewise, reduces the symptoms of distress and mental health problems [12].
CBT is an intervention that improves the coping skills in anxiety. This intervention help an individual how respond to stressful events in their life [13]. For mild to moderate depression, CBT even competes with antidepressant medications and a combination of CBT and antidepressant medications increases the effectiveness of treatment. Among all the psychotherapies, CBT is considered the first line of treatment for depression [14]. Thus, effectiveness and efficiency of this treatment are approved for both anxiety and depression.
Considering the increasing cases of psychological problems including anxiety and depression during the recent pandemic and the existence of various psychological therapies, we decided to meta-analysis and systematically review the effectiveness of CBT on anxiety and depression during this period.
Methods
Inclusion criteria
The studies entered in this research consist of clinical trials analyzing the effects of CBT on depression and anxiety during COVID-19 pandemic period. Other studies such as editorial studies, case studies, protocol studies, articles with insufficient data and studies with lack of control group were excluded from the present study. In addition, we included the studies just conducted during the COVID-19 pandemic. We excluded the studies which used another intervention for control groups. In this study, the researchers using the keywords they looked up in MeSH such as COVID-19, depression, anxiety and CBT launched their study by searching English databases such as PubMed, Web of Science, Google Scholar, Cochrane as well as Persian databases such as SID, MagIran and IranDoc with a time limit of 2019 to 2022. Moreover, clinical registries such as EU-CTR and IRCT were searched for relevant unpublished studies. We updated our search on 17/08/2022 for last time.
Defined PICO for this study included participants (people during COVID-19 pandemic regardless of sex and age), intervention (CBT), control group (with no intervention) and outcomes (anxiety and depression).
One of the strategies used in this study to search in PubMed database is as follows:
-
((depression [MESH Terms]) OR anxiety [MESH Terms]) AND cognitive behavior therapy [MESH Terms] at COVID-19
Quality assessment and data extraction
Two researchers (NZ and RH) independently investigated the titles and abstracts of the studies that were obtained via the search for a review study; if obtained data were not sufficient for decision making, the whole article was analyzed and any uncertainty about its suitability for being entered in the study was resolved through consulting with a third researcher (MM).
The researchers extracted the data from the relevant studies on the basis of Cochrane handbook including: first author’s name, year of publication, country, characteristics and design of intervention, age of participants, sample size, type of intervention, type of control group, measuring tools, results and consequences, and then presented the data in Table 1.
Two researchers (NZ and RH) independently assessed risk of biases and again evaluated and resolved any inconsistencies via counseling with a third researcher (MM). The studies included were analyzed on the basis of Cochrane Handbook and in regard to six domains of bias (random allocation, allocation concealment, blinding of participant and personnel, blinding of data assessor, incomplete outcome data, and selective reporting) in three levels of low-risk, unclear, and high-risk and the results are presented in Table 2. The quality of evidence was analyzed using Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach and is reported in Table 3. Likewise, for assessing publication bias, funnel plot was plotted for 10 studies that evaluated anxiety.
Data analysis
The Review Manger (RevMan) software of version 5.3 and Stata version 14.2 software (Stata crop, College Station, TX, USA) were used for meta-analysis and plotting bias forms. Because of the different tools that were used for measuring anxiety and depression, meta-analysis results were reported using standardized mean difference (SMD) and 95% confidence interval (95% CI). Heterogeneity of studies was analyzed by means of I2 index, and in cases with high heterogeneity, random effects model was used instead of fixed effects model. Subgroup analysis was conducted on the basis of being infected with coronavirus, not being infected with coronavirus, having a history of depression and anxiety before the intervention and internet-based CBT for depression and anxiety. Since the number of included studies in the meta-analysis of anxiety was more than 10 studies, publication bias was assessed with Egger’s test and funnel plot. A meta-regression analysis was performed to estimate the influence of the participants’ type (being infected with coronavirus, not being infected with coronavirus, having a history of depression and anxiety) on heterogeneity.
Results
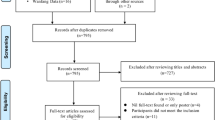
A total of 2015 articles were obtained from the search in different databases of which 1987 articles were excluded due to duplicates or the irrelevancy of their titles or after reviewing their abstracts. Of 28 remaining articles, 14 of the articles did not enter the systematic review due to the following reasons: Mohammadi et al. [15] and Norred et al. [16] articles were excluded from the study because of its editorial type. Hosseinzade et al. [17] article did not include to the study, because it was a study protocol. Kalvin et al. study [18] was a commentary study. Likewise, Mahoney et al. study [19], Zhang et al. study [20], Araghi et al. study [21] and Uysal et al. study [22], Green et al. study [23] were excluded from the study due to lack of the control group. Johnco et al. study [24] and Sharrock et al. study [25] did not enter the study, because the studies were conducted previously and the follow-up was conducted again in the coronavirus period. Fadhli et al. study [26] was excluded, since the mean and standard deviation of results before and after the intervention were reported as a single value together and the effects of the intervention were not properly stated. Likewise, Perri et al. study [27] and Hamed et al. study [28] were excluded from the study, because its control group had received another type of intervention. Of the 14 remaining articles, one article was not retrieved, because the full text of Barve et. al [29] study was not available, we emailed the authors but we did not receive any response; so this article was not included in the present study. In addition, two of the articles including Oehler et al. study [30] due to lack of anxiety scores before and after the intervention and LV et al. study [31] because of presenting insufficient data were excluded from the study. Finally, 11 articles were entered into the study (Fig. 1).

PRISMA flow diagram (2020) of screening, selection process and inclusion study
The risks of biases of the entered studies are presented in Table 2. Most of the studies did not provide sufficient data on how randomization was done and so are placed at unclear risk level; likewise, most of the studies are put at low risk level regarding allocation concealment bias. All of the studies are high risk in terms of performance bias. All studies except one [32] are at high-risk level in terms of detection bias. Moreover, all studies are low risk in terms of reporting bias and attrition bias (Figs. 2 and 3).

Risk of bias graph: review authors judgments about each risk of bias item presented as percentages across all included studies

Risk of bias summary: review authors judgment about each risk of bias item for each included study
The specifications of included studies are as follows
Three of the studies were conducted in China [1, 33, 34], four of them in Iran [35,36,37,38], one of them was the common study between Australia and United Kingdom [39], two of them in Sweden [32, 40] and one of them in Saudi Arabia [41]. All of the studies were clinical trial but one of them was a pilot study [38]. All of the studies were conducted during the COVID-19 pandemic. The largest and smallest sample sizes were 670 [32] and 30 [35, 38]. Five studies were conducted face to face [1, 34,35,36, 38] but the others were internet-based. In 4 studies, there was no information about the gender of participants [33, 36,37,38]. One study was conducted just on girls [35] and others were on both gender. Most of the studies were conducted on adults above 18 years, just in one of the studies, participants were adolescents [35] and two of them had no age limitation [1, 34]. The scales used in the studies were different such as Hamilton Depression Scale (HAMD), Hamilton Anxiety Scale (HAMA), Self-related Depression Scale (SDS), Depression Anxiety Stress Scale (DASS-21), Patient Health Questionnaire (PHQ-9), Generalized Anxiety Depression (GAD-7), Short Health Anxiety Inventory (SHAI), COVID-19 Anxiety Questionnaire (CVAQ), Anxiety Sensitivity Inventory (ASI), Beck Depression Inventory (BDI), and Montgomery Asberg Depression Rating Scale (MADRS-S). Most of the articles examined both outcomes (depression and anxiety) but two of them examined just anxiety [38, 41].
Meta-analysis
Random-effects meta-analysis on 6 studies and 1269 participants showed that the mean score of depression in the intervention group was significantly lower than the control group (SMD − 0.58; 95% CI − 1.00 to − 0.16; P < 0.00001) and heterogeneity level of I2 = 94% were obtained. Subgroup analysis results on the basis of being or not being infected with coronavirus or having a history of depression were as follows.
In terms of depression variable, just one study was performed on people not infected with coronavirus and meta-analysis results showed that CBT had a positive effect on lowering the mean score of depression among the patients not infected with coronavirus (MD − 0.36; 95% CI − 0.51 to − 0.21; P < 0.00001). However, there was no statistically significant difference between two groups for those infected with coronavirus (SMD − 1.00; 95% CI − 2.87 to 0.87; P < 0.00001; I2 = 98%) and people with a history of depression (SMD − 0.52; 95% CI − 1.22 to 0.17; P = 0.005; I2 = 81%). There were two studies that implemented CBT via the internet for depression. Subgroup analysis was conducted on these studies. The results of the meta-analysis showed that internet-based CBT was effective in reducing of depression (SMD − 0.35; 95% CI − 0.50 to − 0.20; P < 0.00001; I2 = 0%) (Fig. 4).

Meta-analysis of effect of CBT on depression during COVID-19 pandemic
Random-effects meta-analysis on 11 studies and 1859 participants showed that the mean score of anxiety in the intervention group was significantly lower than the control group (SMD − 0.95; 95% CI − 1.29 to − 0.62; P < 0.00001; I2 = 94%). Subgroup analysis results on the basis of being or not being infected with coronavirus or having a history of anxiety were as follows.
In terms of anxiety variable, subgroup analysis results showed that CBT had significant effect just on lowering anxiety score for those people with a history of anxiety (SMD − 1.24; 95% CI − 1.84 to − 0.63; P < 0.00001, I2 = 90%) but for people infected (SMD − 0.98; 95% CI − 2.41 to 0.45; P = 0.18, I2 = 97%) and not infected with coronavirus (SMD − 0.28; 95% CI − 0.68 to 0.12; P = 0.17; I2 = 82%) there were no statistically significant difference between the intervention and control groups. There were 6 studies that assessed the effect of internet-based CBT on anxiety. Subgroup analysis was conducted on these studies. The meta-analysis results showed that internet-based CBT had a significant effect on anxiety (SMD − 0.90; 95% CI − 1.47 to − 0.33; P = 0.002; I2 = 94%) (Fig. 5).

Meta-analysis of effect of CBT on anxiety during COVID-19 pandemic
The asymmetrical appearance of the funnel plot indicates the probable presence of publication bias in the anxiety-related studies (Fig. 6). This was confirmed by the results of an Egger regression that showed significant publication bias (P = 0.024).

Funnel plot of the effect of CBT on anxiety during COVID-19 pandemic
The results of meta-regression model indicated that in both variables of anxiety and depression, none of the two groups (participants with corona and participants with anxiety) did not show significant difference compared to the participants without corona.
The evidence about the effectiveness of CBT on depression and anxiety compared with control group on the basis of GRADE approach had low quality, so the results were close to reality with low reliability. The results of evaluation of evidence utilizing GRADE are shown in Table 3.
Discussion
According to most of the studies, COVID-19 pandemic has a negative impact on individual mental health so different psychological approaches should have been used to improve society’s well-being. CBT is one of the effective approaches for psychological disorders. In the present study, the effects of CBT on people’s depression and anxiety in COVID-19 pandemic period were analyzed. Based on the overall results of meta-analysis, CBT had a significant effect on reducing anxiety and depression. Since we did not find systematic review studies on the effects of CBT on anxiety and depression in coronavirus period, we reviewed similar studies. No study was found that examined both outcomes so we have reviewed outcomes separately. There were some studies that evaluated the effect of CBT on the anxiety.
Hall et al. [42] evaluated the effects of CBT on the anxiety disorder. Meta-analysis results in the study were similar to the present study and showed that CBT was significantly effective on reducing anxiety in the intervention group. Unlike the present study, in the Hall et al. study, control groups have received different interventions, such as supportive therapy, acceptance and commitment therapy, discussion group and etc. In a systematic review and meta-analysis, Sigurvinsdóttir et al. [43] studied the effects of CBT on anxiety. Meta-analysis results showed that CBT was significantly effective. Sigurvinsdóttir study was conducted just on children and adolescents, and so its results could not be generalized to other age groups but the present study has no age limitation in inclusion criteria.
There are a number of articles that evaluated the effect of CBT on depression. In a systematic review, Lopez-Lopez et al. [44] investigated the effects of CBT on depression. This study conducted just on adults above 18. In the present study, we have no age limitation. In a systematic review and meta-analysis, Santoft et al. [45] studied the effect of CBT on depression. This study has reviewed more articles than the present study (34 articles) and control groups have received different interventions, such as placebo pill, psychotherapy and etc. The results of Santoft et al. study similar to the results of the present study showed that CBT significantly reduced symptoms of depression in the intervention group. All of these studies were conducted before COVID-19 pandemic.
CBT is a therapeutic approach that is suggested for the treatment of depression and anxiety by Aaron beck. CBT helps the patients change their thoughts and through which leads to better feelings in them [46]. Since negative thoughts have a detrimental influence on developing emotional disorders such as anxiety and depression, CBT alleviates anxiety and depression symptoms through recognizing, challenging, and changing negative thoughts and replacing them with logical thoughts [47]. Moreover, CBT improves many mental health disorders such as anxiety and depression through developing capabilities necessary for coping with everyday life events [48], and since many studies approve that CBT is one of the valid therapeutic methods, it is extensively used. Most of the studies detected changes in the brain (such as prefrontal hyperactivity) during psychological disorders, such as anxiety and depression. Findings of studies showed that the abnormal hyperactivities of the prefrontal decrease following treatment. In addition, results showed that CBT can enhance the prefrontal control structures [49, 50]. In some of the studies, researchers used internet-based CBT instead of face to face CBT due to COVID-19 pandemic.
The results of the subgroup meta-analysis showed that ICBT (internet-based CBT) is effective in reducing depression and anxiety. In the Farrer et al. study [51], ICBT was effective in reducing depression, although they used weekly telephone tracking too. In Herman et al. study [52], ICBT was effective in reducing anxiety. They followed up the participants for 5 years. The results of Etzelmueller et al. [53] and Lau et al. [54] studies were similar to the present study too and ICBT was effective in reducing depression and anxiety. However, Etzelmueller et al. study has reviewed more articles than the present study (19 articles) and they included adults and older adolescents in their study. In the present study, we have no age limit. In addition, the participants of the Lau et al. study were postpartum women. All of these studies were conducted before COVID-19 pandemic.
Strength and limitation
This systematic review and meta-analysis has a number of weaknesses and strengths. One of the limitations was the small sample size of the included studies. In addition, we had just 11 studies which also limited our sub-group analyses. The other limitations of the present study were different study designs, participant’s ages and outcome measures. In addition, the most of the included studies did not clearly stated their methods of randomization and so were placed in unclear risk level in terms of randomization bias, just one study [39] was low risk in this regard. In none of the studies blinding was performed, however, in just one study [31], analyzer’s blinding was done. Of other weaknesses of the included studies was their different inclusion criteria, for instance, some of the studies were conducted on people infected with coronavirus, some on people having a history of depression and anxiety, and some on people not infected with coronavirus. Likewise, in most of the studies duration of follow-up was not stated. In most of the studies, because of coronavirus pandemic and the necessity of quarantine and observing social distance, CBT counseling sessions were performed online and via internet that is one of the weaknesses of these studies, because there was no possibility of face to face meetings between counselors and clients; however, this was the best decision in the pandemic period and provided people with the opportunity to benefit from counseling and the results also showed the effectiveness of the method.
One the strengths of the present study is that all of the included studies are at low-risk level in terms of reporting bias and attrition bias. Likewise, in the present systematic review, all age groups regardless of their sex entered the study, so the results are generalizable to all age groups and both sexes. Of other strengths of this study, we can refer to subgroup analysis.
Conclusions
Meta-analysis shows that CBT is significantly effective on reducing depression and anxiety scores in COVID-19 pandemic period. Therefore, extensive use of this method during coronavirus pandemic and other similar pandemics is recommended. It is suggested that the effectiveness of other psychological approaches on the problems developed during the pandemic to be analyzed in other studies. Moreover, since the need for counseling and psychological interventions is inevitable due to psychological and mental disorders people experience during different kinds of crises such as natural or social crises or pandemics etc., it is recommended that governments and communities put paying enough attention to these methods on their agenda.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- CBT:
-
Cognitive behavior therapy
- SMD:
-
Standardized mean difference
- MeSH:
-
Medical subject heading
- EU-CTR:
-
European Union Clinical Trials Register
- IRCT:
-
Iranian Registry of Clinical Trial
- CI:
-
Confidence interval
- WHO:
-
World Health Organization
- RCT:
-
Randomized controlled trial
- GRADE:
-
Grading of recommendations assessment, development and evaluation
- HAMD:
-
Hamilton depression scale
- HAMA:
-
Hamilton anxiety scale
- SDS:
-
Self-relating depression scale
- DASS:
-
Depression anxiety stress scale
- PHQ:
-
Patient health questionnaire
- GAD:
-
Generalized anxiety depression
- SHAI:
-
Short health anxiety inventory
- CVAQ:
-
COVID-19 anxiety questionnaire
- ASI:
-
Anxiety sensitivity inventory
- BDI-II:
-
Beck depression inventory-II
- MADRS-S:
-
Montgomery-Asberg depression rating scale
References
Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020;382(13):1199–207.
COVID-19 Coronavirus pandemic 2021. https://www.worldometers.info/coronavirus/. Accessed 25 Aug 2021.
Torales J, O’Higgins M, Castaldelli-Maia JM, Ventriglio A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int J Soc Psychiatry. 2020;66(4):3120–7.
Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395(10227):912–20.
Tran BX, Nguyen HT, Le HT, Latkin CA, Pham HQ, Vu LG, et al. Impact of COVID-19 on economic well-being and quality of life of the Vietnamese during the national social distancing. Front Psychol. 2020. https://doi.org/10.3389/fpsyg.2020.565153.
Yang Y, Li W, Zhang Q, Zhang L, Cheung T, Xiang Y-T. Mental health services for older adults in China during the COVID-19 outbreak. Lancet Psychiatry. 2020;7(4): e19.
Consortium WWMHS. Prevalence, severity, and unmet need for treatment of mental disorders in the World Health Organization world mental health surveys. JAMA. 2004;291(21):2581–90.
WHO. Investing in treatment for depression and anxiety leads to fourfold return USA 2016. https://www.who.int/news/item/13-04-2016-investing-in-treatment-for-depression-and-anxiety-leads-to-fourfold-return. Accessed 13 April 2016.
Li J, Yang Z, Qiu H, Wang Y, Jian L, Ji J, et al. Anxiety and depression among general population in China at the peak of the COVID-19 epidemic. World Psychiatry. 2020;19(2):249.
Pfefferbaum B, North CS. Mental health and the COVID-19 pandemic. N Engl J Med. 2020;383(6):510–2.
Schure MB, Lindow JC, Greist JH, Nakonezny PA, Bailey SJ, Bryan WL, et al. Use of a fully automated internet-based cognitive behavior therapy intervention in a community population of adults with depression symptoms: randomized controlled trial. J Med Internet Res. 2019;21(11): e14754.
Ólason M, Andrason RH, Jónsdóttir IH, Kristbergsdóttir H, Jensen MP. Cognitive behavioral therapy for depression and anxiety in an interdisciplinary rehabilitation program for chronic pain: a randomized controlled trial with a 3-year follow-up. Int J Behav Med. 2018;25(1):55–66.
Chu BC, Harrison TL. Disorder-specific effects of CBT for anxious and depressed youth: a meta-analysis of candidate mediators of change. Clin Child Fam Psychol Rev. 2007;10(4):352–72. https://doi.org/10.1007/s10567-007-0028-2.
Flynn HA, Warren R. Using CBT effectively for treating depression and anxiety. Curr Psychiatry. 2014;13(6):45–53.
Mohammadi A, Cummings J. How CBT can be protective against anxiety disorders during COVID-19 era. Iran J Psychiatry Behav Sci. 2020;14(3): e106601.
Norred MA, Haselden LC, Sahlem GL, Wilkerson AK, Short EB, McTeague LM, George MS. TMS and CBT-I for comorbid depression and insomnia. Exploring feasibility and tolerability of transcranial magnetic stimulation (TMS) and cognitive behavioral therapy for insomnia (CBT-I) for comorbid major depressive disorder and insomnia during the COVID-19 pandemic. Brain Stimul. 2021;6:1508–10.
Hoseininezhad N, Rezaeian FH. The effectiveness of the cognitive-behavioral treatment on the experience of grief, depression and anxiety by bereft families of Covid-19 victims. J Psychol Stud. 2022. https://doi.org/10.22051/psy.2022.39774.2589.
Kalvin CB, Jordan RP, Rowley SN, Weis A, Wood KS, Wood JJ, et al. Conducting CBT for anxiety in children with autism spectrum disorder during COVID-19 pandemic. J Autism Dev Disord. 2021. https://doi.org/10.1007/s10803-020-04845-1.
Mahoney A, Li I, Haskelberg H, Millard M, Newby JM. The uptake and effectiveness of online cognitive behaviour therapy for symptoms of anxiety and depression during COVID-19. J Affect Disord. 2021. https://doi.org/10.1016/j.jad.2021.05.116.
Zhang C, Yang L, Liu S, Xu Y, Zheng H, Zhang B. One-week self-guided internet cognitive behavioral treatments for insomnia in adults with situational insomnia during the COVID-19 outbreak. Front Neurosci. 2021;14: 622749.
Araghi NM, Zarei MA, Saei S, Yousefi Nodeh HR, Mahmoudi E. The effect of online cognitive behavioral therapy on depressive symptoms in recovered patients with COVID-19. J Educ Health Promot. 2022;11:70. https://doi.org/10.4103/jehp.jehp_727_21.
Uysal B, Morgul E, Tastekne F, et al. Videoconferencing-based cognitive behavioral therapy for youth with anxiety and depression during COVID-19 pandemic. Sch Psychol Int. 2022;43(4):420–39.
GREEN Sheryl M, et al. Evaluation of an augmented cognitive behavioural group therapy for perinatal generalized anxiety disorder (GAD) during the COVID-19 pandemic. J Clin Med. 2021;11(1):209.
Johnco CJ, Chen JT, Muir C, Strutt P, Dawes P, Siette J, et al. Long-term relapse rates after cognitive behaviour therapy for anxiety and depressive disorders among older adults: a follow-up study during COVID-19. Australas J Ageing. 2021. https://doi.org/10.1111/ajag.12928.
SHARROCK Maria J, et al. The uptake and outcomes of internet-based cognitive behavioural therapy for health anxiety symptoms during the COVID-19 pandemic. J Anxiety Disord. 2021;84:102494.
Fadhli T, Situmorang DDB. Implementation of cognitive behavioral therapy with cognitive restructuring technique to reduce psychosocial anxiety in the COVID-19 outbreak. Addict Disord Their Treat. 2021;20(4):268–77.
Perri RL, Castelli P, La Rosa C, Zucchi T, Onofri A. COVID-19, Isolation, quarantine: on the efficacy of internet-based eye movement desensitization and reprocessing (emdr) and cognitive-behavioral therapy (CBT) for ongoing trauma. Brain Sci. 2021;11(5):579.
Hamed NS, et al. The effect of aerobic training versus cognitive behavioral therapy in management of anxiety, depression and stress related to COVID 19 pandemic among university students: a randomized controlled trial. Med Sci. 2021;25(115):2233–46.
Barve SR, Kadam G. Combined telephonic and online CBT with performing artist suffering from pandemic induced depression with anxious distress. Indian J Health Wellbeing. 2021;12(3):391–3.
Oehler C, Scholze K, Reich H, Sander C, Hegerl U. Intervention use and symptom change with unguided internet-based cognitive behavioral therapy for depression during the COVID-19 pandemic: log data analysis of a convenience sample. JMIR Mental Health. 2021;8(7): e28321.
Lv Z, Li J, Zhang B, Zhang N, Wang C. The effect of computerized cognitive behavioral therapy on people’s anxiety and depression during the 6 months of Wuhan’s lockdown of COVID-19 epidemic: a pilot study. Front Psychol. 2021;12: 687165.
Wahlund T, Mataix-Cols D, Lauri KO, de Schipper E, Ljótsson B, Aspvall K, et al. Brief online cognitive behavioural intervention for dysfunctional worry related to the COVID-19 pandemic: a randomised controlled trial. Psychother Psychosom. 2021;90(3):191–9.
Song J, Jiang R, Chen N, Qu W, Liu D, Zhang M, et al. Self-help cognitive behavioral therapy application for COVID-19-related mental health problems: a longitudinal trial. Asian J Psychiatr. 2021;60: 102656.
Liu Z, Qiao D, Xu Y, Zhao W, Yang Y, Wen D, et al. The efficacy of computerized cognitive behavioral therapy for depressive and anxiety symptoms in patients with COVID-19: randomized controlled trial. J Med Internet Res. 2021;23(5): e26883.
Heyrat A, Aghajani Fesharaki Z, Safara M. The effectiveness of cognitive-behavioral education with a focus on religious principles on depression and anxiety in adolescent girls in corona crisis. Quran Med. 2021;5:58–62.
Shabahang R. Cognitive behavioural intervention for health anxiety, somatosensory amplification, and depression in coronavirus disease 2019 anxiety: an interventional study in Iran. Psychiatr Psychol Klin. 2020;20:87–93.
Shabahang R, Aruguete MS, McCutcheon L. Video-based cognitive-behavioral intervention for COVID-19 anxiety: a randomized controlled trial. Trends Psychiatry Psychother. 2021;43(2):141–50. https://doi.org/10.47626/2237-6089-2020-0056.
Dinarvand F, Bakhtiarpour S, Heydarei A. Comparison of the effectiveness of cognitive behavioral therapy (CBT) and acceptance and commitment therapy (ACT) on reduction of anxiety symptoms in patients with generalized anxiety disorder during the outbreak of Covid-19. J Res Behav Sci. 2022;19(4):590–600.
Egan SJ, McEvoy P, Wade TD, Ure S, Johnson AR, Gill C, et al. Unguided low intensity cognitive behaviour therapy for anxiety and depression during the COVID-19 pandemic: a randomised trial. Behav Res Ther. 2021. https://doi.org/10.1016/j.brat.2021.103902.
Aminoff V, Sellén M, Sörliden E, Ludvigsson M, Berg M, Andersson G. Internet-based cognitive behavioral therapy for psychological distress associated with the COVID-19 pandemic: a pilot randomized controlled trial. Front Psychol. 2021;14(12): 684540. https://doi.org/10.3389/fpsyg.2021.684540.
Ahmed Ali HA, al-Zubaidi MH, Esa MMO. The effect of cognitive behavioral therapy on the internet in reducing anxiety caused by the emerging COVID-19 virus in taif governorate. Multicult Edu. 2021;7(3):373–8.
Hall J, Kellett S, Berrios R, Bains MK, Scott S. Efficacy of cognitive behavioral therapy for generalized anxiety disorder in older adults: systematic review, meta-analysis, and meta-regression. Am J Geriatr Psychiatry. 2016;24(11):1063–73.
Sigurvinsdóttir AL, Jensínudóttir KB, Baldvinsdóttir KD, Smárason O, Skarphedinsson G. Effectiveness of cognitive behavioral therapy (CBT) for child and adolescent anxiety disorders across different CBT modalities and comparisons: a systematic review and meta-analysis. Nord J Psychiatry. 2020;74(3):168–80.
López-López JA, Davies SR, Caldwell DM, Churchill R, Peters TJ, Tallon D, Welton NJ. The process and delivery of CBT for depression in adults: a systematic review and network meta-analysis. Psychol Med. 2019;49(12):1937–47.
Santoft F, Axelsson E, Öst LG, Hedman-Lagerlöf M, Fust J, Hedman-Lagerlöf E. Cognitive behaviour therapy for depression in primary care: systematic review and meta-analysis. Psychol Med. 2019;49(8):1266–74.
Holmes L. Cognitive-behavioral therapy for depression and anxiety 2020 [cited 2021]. https://www.verywellmind.com/cognitive-therapy-for-depression-and-anxiety-2330690. Accessed 22 Sep 2020.
Cherry K. What is cognitive behavioral therapy (CBT)? 2021. https://www.verywellmind.com/what-is-cognitive-behavior-therapy-2796747. Accessed 7 May 2021.
Butler AC, Chapman JE, Forman EM, Beck AT. The empirical status of cognitive-behavioral therapy: a review of meta-analyses. Clin Psychol Rev. 2006;26(1):17–31.
Marwood L, Wise T, Perkins AM, Cleare AJ. Meta-analyses of the neural mechanisms and predictors of response to psychotherapy in depression and anxiety. Neurosci Biobehav Rev. 2018;95:61–72.
Lueken U, Hahn T. Functional neuroimaging of psychotherapeutic processes in anxiety and depression: From mechanisms to predictions. Curr Opin Psychiatry. 2016;29(1):25–31.
Farrer L, Christensen H, Griffiths KM, Mackinnon A. Internet-based CBT for depression with and without telephone tracking in a national helpline: randomized controlled trial. PLoS ONE. 2011;6(11): e28099. https://doi.org/10.1371/journal.pone.0028099.
Erik H, et al. A 5-year follow-up of internet-based cognitive behavior therapy for social anxiety disorder. J Med Internet Res. 2011;13(2):e1776.
Etzelmueller A, Vis C, Karyotaki E, Baumeister H, Titov N, Berking M, Cuijpers P, Riper H, Ebert D. Effects of internet-based cognitive behavioral therapy in routine care for adults in treatment for depression and anxiety: systematic review and meta-analysis. J Med Internet Res. 2020;22(8):e18100. https://doi.org/10.2196/18100.
Lau Y, Htun T, Wong S, Tam W, Klainin-Yobas P. Therapist-supported internet-based cognitive behavior therapy for stress, anxiety, and depressive symptoms among postpartum women: a systematic review and meta-analysi. J Med Internet Res. 2017;19(4):e138. https://doi.org/10.2196/jmir.6712.
Acknowledgements
No acknowledgements.
Funding
No financial support.
Author information
Authors and Affiliations
Contributions
NZ and RH have been designed the study, collected the data, checked the biases, and wrote the draft of manuscript. MM have been designed the study, controlled the data, analysed the data and revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zamiri-Miandoab, N., Hassanzade, R. & Mirghafourvand, M. The effect of cognitive behavior therapy on anxiety and depression during COVID-19 pandemic: a systematic review and meta-analysis. Ann Gen Psychiatry 21, 40 (2022). https://doi.org/10.1186/s12991-022-00417-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12991-022-00417-y