
Abstract
Background
Children with juvenile idiopathic arthritis (JIA) are at higher risk of decreased bone mineral density (BMD) compared with healthy children due to genetic, disease and medication-related causes. This study aims to investigate the possible effects of osteoprotegerin (OPG) gene polymorphisms and serum levels of osteoprotegerin (OPG) and receptor activator of nuclear factor κB-ligand (RANKL) and RANKL/OPG ratio on BMD in children with JIA.
Methods
OPG gene rs2073617, rs3134069, serum RANKL, OPG and RANKL/OPG ratio were evaluated in 60 JIA children and 100 matched healthy controls. BMD was evaluated by lumbar dual energy X-ray absorptiometry (DEXA) according to which patients were classified in 2 groups (DEXA z-score above and below − 2). Composite disease activity was measured using the Juvenile Arthritis Disease Activity Score (JADAS) 27-joints. Articular damage was scored using the juvenile arthritis damage index (JADI).
Results
Patients aged 12.05 ± 3.2 years, included 38 females and 31% had BMD z-score below-2. Systemic-onset JIA was the most frequent phenotype (38%). Genotypes and alleles frequencies of the 2 studied polymorphisms did not differ between patients and controls (p > 0.05 for all) while serum RANKL and RANKL/OPG ratio were significantly higher in patients compared to controls (p = < 0.001 and 0.03 respectively). Patients with BMD < -2 had significantly greater frequencies of rs2073617 TT genotype and T allele (p < 0.001), higher serum RANKL, RANKL/OPG ratio (p = 0.01, 0.002), female predominance (p = 0.02), higher articular and extra-articular damage index (p = 0.008,0.009) and more frequent steroid usage (p = 0.02) compared to patients with BMD z-score >-2. Multivariate analysis showed rs2073617 TT genotype, RANKL/OPG ratio, long disease duration (above 36 months) and use of steroid to be associated with decreased BMD (p = 0.03,0.04,0.01,0.01 respectively) in JIA children.
Conclusions
Egyptian children with JIA have decreased BMD. rs2073617 TT genotype and T allele, RANKL/OPG ratio are possible determinants of reduced BMD in JIA. Our results underline the importance of frequent monitoring of BMD in JIA children and trying to control disease activity to preserve long term bone health.
Similar content being viewed by others

Background
Children with juvenile idiopathic arthritis (JIA) are at increased risk of reduced bone mineral density (BMD) which is related to diverse factors as chronic inflammation, medications, nutrition, and decreased physical activity. It is important to detect the early changes in BMD in JIA to identify patients at risk to develop reduced bone mass [1]. Dual energy X-ray absorptiometry (DEXA) is the most frequently used method for evaluating the bone mineralization status in different ages [2] but it is technically difficult to perform and to interpret its results in children with growth retardation and hormonal disturbances. So, new more applicable markers are required [3].
Tumour necrosis factor (TNF) is considered the chief inflammatory pathogenic mediator for chronic arthritis [4]. Among the TNF family, the receptor activator of nuclear factor-κB (RANK),RANK ligand (RANKL), and osteoprotegerin (OPG) are involved in many immunological and skeletal diseases characterized by bone resorption including inflammatory arthritis[5]. Expression of the RANKL by osteoblasts is crucial to osteoclastogenesis. OPG is a soluble receptor for RANKL that prevents RANK/RANKL interaction [6, 7]. Therefore, the RANKL/OPG ratio is critical for guiding bone resorption. Altered RANKL/ OPG ratio has been described in multiple autoimmune diseases and has been linked to decreased BMD [8, 9]. As genetic background has a pivotal role in determining peak bone mass [10], and OPG protect from bone resorption and cartilage damage [11, 12], the OPG gene may be a good contestant to identify subjects with high risk of compromised BMD.
Understanding the impact of JIA on children’s bone health may help enhanced prevention and treatment of these complications in children. In the current work, we aimed to assess the RANKL/OPG balance in JIA patients compared with healthy controls and correlate serum levels of RANKL, OPG and RANKL/OPG ratio with clinical phenotypes, BMD, disease activity and damage indices. In addition, 2 polymorphisms of OPG gene (rs2073617 and rs3134069) have been studied and correlated to BMD. To the best of our knowledge these 2 polymorphisms were not studied before in JIA despite their reported role in impaired BMD in Egyptian childhood systemic lupus erythematosus (SLE) [13], and in adults with rheumatoid arthritis (RA) [14].
Methods
Study participants
Sixty patients with JIA diagnosed according to the International League of Associations for Rheumatology (ILAR) criteria [15] were recruited from paediatric Rheumatology clinic, Mansoura University Children’s Hospital. One hundred age and sex matched children, apparently healthy and with no features suggestive or family history of rheumatic disorders were recruited as controls (all control group have been included before in previous research [13]).
All patients had normal renal function (at time of sampling) defined as normal estimated glomerular filtration rate (eGFR) for their age (as renal clearance plays an important role in the excretion of OPG). Exclusion criteria included patients with reduced eGFR and patients with associated autoimmune disorders or mixed connective-tissue diseases and other disorders affecting bone status as rickets, thyroid and parathyroids disorders.
For follow up of our patients; when the criteria for inactive disease [16, 17] are met for a minimum of six consecutive months while the patient is receiving anti-rheumatic medications, the patient is classified as being in the state of clinical remission with medication. When the criteria for inactive disease are met for a minimum of 12 consecutive months after the patient has discontinued all anti-rheumatic medications, the patient is classified as being in the state of clinical remission without medication. However, as we did not follow up our patients for the required period, Composite disease activity was measured (at time of sampling) by the Juvenile Arthritis Disease Activity Score (JADAS) 27-joints (range 0–57) [18]. Long term damage (articular and extra-articular) was scored using the Juvenile Arthritis Damage Index (JADI) [19].
None of the included 60 patients received bisphosphonates up to the time of sampling and BMD assessment in the study. Unfortunately, Data regarding calcium and vitamin D consumption were not included in the analysis because of patients’ inconstant interrupted undocumented doses and intake durations.
Sample collection and serum RANKL /OPG measurement
A total of 5ml blood samples were collected from all subjects by venepuncture. Two ml of blood were added to Ethylene Di-amine Tetra-acetic Acid (EDTA) containing tube and stored at -20 °C until extraction of DNA. The remaining three ml blood were delivered in a dry tube, allowed to clot at room temperature for about half an hour and then centrifuged at 3000 round per minute (rpm) for 15 min to obtain the serum. The serum was stored at − 80 °C until further use by enzyme-linked immune sorbent assay (ELISA) technique. Both protocols were performed according to the manufacturer’s instructions. The unit of the standards in the two ELISA kits used in the study was ng per L. The RANKL/OPG ratio was calculated and included in the statistical analysis.
Single nucleotide polymorphism genotyping
For the control group, we used the results of genotyping of the 100 controls included in our previous research [13]. While for cases, DNA was extracted from peripheral blood samples using Quick-DNA (Zymo research, Orange, CA, USA, Cat. No D3024) according to standard procedures and screened for the T950C and T245G, OPG gene polymorphisms using polymerase chain reaction (PCR)-based restriction fragment length polymorphism technique.
Rs2073617
A 570-bp fragment around the T950C polymorphism (rs2073617) was amplified as described by Soufi et al. [20]. The PCR products were digested with HincII restriction endonuclease (Fermentas, Burlington, ON, Canada) and digestion products were separated on 2.5% agarose gels. In the presence of a C nucleotide at position 950, the 570 bp PCR product is cleaved into 288 bp and 282 bp fragments (Fig. 1A).

(A) Electrophoresis pattern of T950C (rs2073617) polymorphism resolved on 2.5% agarose gel. Lane 1, 2, 4, 5: TT homozygote (570 bp); Lane 3, 8, 9: TC heterozygote (570, 282 and 288 bp); lane 7: CC homozygote (288 bp and 282 bp fragments ”appear as one band”); Lane 6: 50 bp DNA ladder. (B) Electrophoresis pattern of T245G (rs3134069) polymorphism resolved on 3% agarose gel. Lane 2, 5, 7: GG homozygote (271 bp); Lane 1, 4, 8: TT homozygote (202 bp and 69 bp fragments); lane 3, 6: TG heterozygote (271, 202 and 69 bp); Lane 9: 50 bp DNA ladder
Rs3134069
The PCR products for T245G (rs3134069) (271 bp fragment) were amplified as described by Pitocco et al. [21], then they were digested with HinfI restriction endonuclease (Fermentas) and separated on 3% agarose gels. The 271 bp PCR product was cleaved into 202 bp and 69 bp fragments only in the presence of a T nucleotide at position 245 (Fig. 1B).
BMD assessment
Lumbar (L2–L4) BMD (g/cm2) was performed on all patients using a Lunar DPX IQ-USA, software version 4.5. All scans were performed by the same technician, and evaluation was conducted by a single expert observer. The results of the BMD were compared with 352 healthy age- and sex-matched Egyptian controls [22, 23]and z-score was calculated. Patients with a BMD z-score <–2 was diagnosed as having low bone mass, whereas others were considered normal [24].
Radiographic examination
Conventional film screen radiographs of all affected joints were obtained. The features evaluated as absent or present.
Study power
The G*Power 3.1.9.7 was used to estimate the sample size using the following parameters; Effect size – 0.5, α err prob = 0.05, Power (1-β err prob) = 0.80, Allocation ratio N2/N1 = 0.7, Output: Non-centrality parameter δ = 2.8244066, Critical t = 1.9783804, Df = 130, Sample size group 1 = 78, Sample size group 2 = 54, Total sample size = 132, Actual power = 0.8005319. According to the The G*Power 3.1.9.7, the estimated sample size is 132 (78 cases and 54 controls). However, only 60 cases included as only available cases at our centre that fulfilled inclusion criteria while controls increased to 100 to enable more comparison between groups.
Statistical analysis
Results were reported as means and medians for continuous or proportions for categoric variables. sRANKL and OPG levels and sRANKL/OPG ratio, OPG gene genotypes and alleles frequencies were compared between JIA patients and healthy controls. Genotypes and alleles frequencies, serum RANKL/OPG levels and other clinical features were compared between patients with BMD z-score below and above − 2 using univariate followed by multivariable linear regression analyses. All studied variables in univariate analyses at a p value < 0.05 were considered potential determinants and entered multivariable linear regression models. Hardy-Weinberg equilibrium was assessed with the Chi-square test or Fisher’s exact test, as appropriate. Statistical calculations were performed using Statistical Package for the Social Sciences (SPSS) Statistics Software, v.25.0 (SPSS Inc, Chicago, IL, USA), and a p value less than 0.05 was considered significant.
Results
Baseline clinical, laboratory and radiological characteristics of the patients
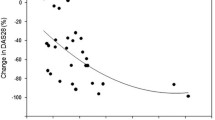
Sixty JIA patients were included in the study. Clinical, laboratory and radiological data of the patients are presented in Table 1. Systemic onset was the most frequent phenotype of the disease, rheumatoid factor (RF) was positive in 19 patients, narrow joint space was the most frequent radiological finding and methotrexate the most frequently used medication. Serum RANKL, RANKL/OPG ratio were significantly higher while serum OPG significantly lower in patients compared to controls. Serum RANKL, OPG and RANKL/OPG ratio in different patients’ phenotypes are presented as scatter plots in Fig. 2.

Scatter plots of RANKL, OPG and RANKL/OPG ratio in different patients’ groups
Genotypes and alleles distribution of the participants
The genotype frequencies of rs2073617 and rs3134069 of controls were within Hardy–Weinberg equilibrium (p = 0.9). OPG gene genotypes and alleles frequencies of the 2 studied SNPs did not show significant difference between patients and controls (Table 2) or between different disease phenotypes. Serum RANKL, OPG and RANKL/OPG ratio were significantly higher in patients with TT genotype of rs2073617 compared to other patients, while no significant difference in RANKL, OPG or RANKL/OPG between different genotypes of rs3134069 (Table 3). Serum RANKL, OPG and RANKL/OPG ratio distribution in control group is also presented in Table 3.
Univariate and multivariate analysis of factors correlated to reduced BMD
Univariate analysis showed that rs2073617 TT genotype and T allele confer significant risk for developing low BMD in children with JIA. Serum RANKL, RANKL/OPG ratio, articular and extra articular damage index score were all significantly higher in patients with BMD z-score below − 2 compared to those with BMD z-score above − 2 and systemic-onset disease was more frequent in patients with BMD z-score < -2 (Table 4). Multivariate analysis showed rs2073617 TT genotype (p = 0.03, OR: 6.8, 95% CI:(3.1–18.2), RANKL/OPG ratio (p = 0.04, OR: 2.6,CI:(3.9-22.08), long disease duration (above 36 months) (p = 0.01, OR:5.2, 95%CI:(2.2–11.3) and the use of steroids (p = 0.01, OR: 4.5, 95%CI:(2.5–19.7) to be associated with decreased BMD in children with JIA.
Other clinical correlations
Serum OPG significantly correlated to composite disease activity (JADAS-27) (r = 0.3, p = 0.02), RANKL/OPG ratio was significantly higher in patients versus those without bony erosions (26.3 ± 27.6 vs. 10.1 ± 11.3, p = 0.002). Cumulative steroid dose showed negative significant correlation to BMD (p = 0.01, r=-0.38). No significant difference in RANKL/OPG ratio was spotted between different disease phenotypes. Also, no significant correlation reported between RANKL/OPG and articular (p = 0.09, r = 0.2) and extraarticular damage scores (p = 0.2, r = 0.2).
Given the distinct pathophysiology and differences in treatment exposures (use of steroids, different biologics, etc.), a supplementary table (Supplementary Table 1) was added detailing the systemic JIA patients’ data, genotypes and BMD status classified into good disease control and active disease based on cut-off points of JADAS-27 as defined by Consolaro et al., 2016 [25].
Discussion
Globally, nearly 3 million children and young adults are suffering from JIA. The region of Africa and Middle East constitute a diverse group of ethnicities, socioeconomic conditions, and climates which influence the prevalence of JIA [26] which is noted to be lower than the range of the global estimate (3.8–400 per 100,000) [27]. Consistent with previous reports from Africa and around the world, female predominance was observed in the current work, but higher age of onset was reported [28,29,30]. Oligoarticular type is reported to be the most frequent followed by polyarticular and systemic phenotypes in different studies [31, 32] which is against our current report in which systemic phenotypes was the most prevalent (38%) while oligoarticular type was reported only in 18% of the cases. Uveitis was not reported in our current cohort. This is consistent with two studies from Oman which did not report any cases of uveitis from their cohorts [33, 34] and with Saurenman et al., who reported a lower risk of uveitis in Arab and Asian JIA patients compared to European or North American ethnicities [35].
Reduced BMD in children with JIA have been replicated in many studies and correlated to wide range of clinical, laboratory and radiological parameters of the disease [36, 37] with the lowest BMD Z-scores reported to be in systemic onset, polyarticular involvement, high steroid doses, and longer disease duration [38, 39]. Low BMD was also reported in adults with history of JIA [40]. In the current work low BMD was reported in 31% of the patients which is against a recent report by Charuvanij et al., who reported no low lumbar BMD and only 5% low total BMD in their cohort of 38 JIA subjects [41] while El Badri et al., reported low BMD in 50% of the studied Moroccan children with JIA [42]. This difference may be related to different sample size, disease duration, characteristics of included subjects and definition of low BMD or osteoporosis.
A high RANKL/OPG ratio in patients compared with controls has been reported in children with nephrotic syndrome [3], children with type 1 diabetes milletus,[43] and juvenile SLE [8] whereas Ozkaya et al. found an increased OPG/RANKL ratio in children with CKD representing a compensatory mechanism to the negative balance of bone remodeling in this disease [44]. However, the role of RANKL/OPG homeostasis in BMD in JIA children explored in few studies [45,46,47,48,49,50,51] with OPG gene polymorphism in children with JIA studied once [47] [to the best of our knowledge]. Main findings of the current study and previous literature on RANKL-OPG axis and OPG gene polymorphism in JIA patients are presented in Table 5.
Decreased BMD in JIA is multifactorial. Lien et al.; reported that JIA patients with oligo- or polyarthritis phenotypes had significantly lower levels of OPG early in the disease course compared to controls and that baseline RANKL was a significant negative predictor of total body lean mass [1]. These findings are consistent with Geusens et al.; findings in newly diagnosed RA patients as the first year OPG:RANKL ratio, as measured at baseline, independently predicted 5-year radiographic progression of joint damage as progression of radiographic damage was greatest in patients with a low OPG:RANKL ratio and was lowest in patients with a high OPG:RANKL ratio. [52]. Shunle et al. studied 45 recent-onset untreated SLE patients and reported that the expressions of the RANKL and OPG genes were significantly reduced in initial SLE compared with normal controls and that initial SLE patients had significantly lower BMD compared to controls [53]. This explains the importance of concomitantly studying serum levels of RANKL/OPG and OPG gene polymorphisms for better recognize bone loss and the clinical significance of the balance between OPG and RANKL in children with JIA.
The correlation of steroids to BMD in different disorders and even between different studies on the same disease is controversial. In the current work we reported a negative significant correlation between cumulative steroid dose and BMD. Sušić et al., reported similar association to cumulative steroid dose in their cohort of 75 children with JIA [36] as well as El Badri et al., [42]. However, Zhizho et al.; reported no significant correlation between cumulative dose of steroids and BMD [54]. Methotrexate has been consistently associated with reduced BMD in children treated for childhood cancer [55], however in the current work the use of methotrexate did not correlate to BMD, which is consistent to previous published reports [42]. This difference may be related to smaller dose of methotrexate used in rheumatic diseases compared to malignancies.
In the current work, no difference reported in BMD in those who received versus those who did not receive biological treatment. Biological treatment with infliximab and etanercept in children with JIA is associated with decrease in disease activity [56]. The positive influence of treatment with TNFα antibodies was also documented upon the skeleton. Simonini was the first to demostrate increased bone mass after 1-year etanercept treatment in children with JIA; reduction of bone loss was associated with therapeutic response with decreased disease activity [57]. Etanercept also improves the linear growth in children with JIA [58].
Based on the concept that increased local or systemic RANKL/OPG may favour increased osteoclastic bone resorption in different metabolic bone disorders, exogenous injection of recombinant OPG has been efficaciously used in various animal models of bone diseases to modulate bone and mineral abnormalities caused by inadequate osteoclast activity [11]. OPG administration exerted a brisk and marked effect and had no adverse effects [59, 60]. A controlled clinical study has confirmed the antiresorptive effect of recombinant human OPG therapy in postmenopausal women as monthly injection of OPG significantly decreased the concentrations of deoxypyridinoline indicating that the data obtained in animals could be replicated in humans [61].
Limitations and strength
The current study was limited by the cross-sectional design, the sample-size that hinders determining a cause–effect relationship between the studied OPG gene SNPs and the risk of osteoporosis in children with JIA and not assessing synovial RANKL levels. However, this study is the first to explore the potential role of the OPG gene rs2073617 and rs3134069 polymorphisms with concomitant evaluation of serum RANKL/OPG levels in susceptibility to reduced BMD in Egyptian children with JIA.
Conclusions
Egyptian children with JIA have decreased BMD. rs2073617 TT genotype and T allele, RANKL/OPG ratio are associated with reduced BMD in patients with JIA. Our results underline the importance of frequent monitoring of BMD in JIA children and trying to control disease activity to preserve long term bone health.
Data Availability
Relevant, de-identified data can be made available on request.
Change history
26 June 2023
This article has been updated to correct an affiliation.
Abbreviations
- ANA:
-
Anti-nuclear antibodies
- BMD:
-
Bone mineral density
- BMI:
-
Body mass index
- CRP:
-
C-reactive protein
- DEXA:
-
Dual energy X-ray absorptiometry
- ERA:
-
Enthesitis-related arthropathy
- ESR:
-
Erythrocyte sedimentation rate
- ILAR:
-
International League of Associations for Rheumatology
- JADAS:
-
Juvenile arthritis disease activity score
- JADI:
-
Juvenile arthritis damage index
- JIA:
-
Juvenile idiopathic arthritis
- OPG:
-
Osteoprotegerin
- PCR-RFLP:
-
Polymerase chain reaction - restriction fragment length polymorphism
- RANKL:
-
Receptor activator of nuclear factor κB-ligand
- RA:
-
Rheumatoid arthritis
- RF:
-
Rheumatoid factor
- SNP:
-
Single nucleotide polymorphism
- SLE:
-
Systemic lupus erythematosus
- TNF:
-
Tumour necrosis factor
References
Lien G, Ueland T, Godang K, Selvaag AM, Førre OT, Flatø B. Serum levels of osteoprotegerin and receptor activator of nuclear factor -kB ligand in children with early juvenile idiopathic arthritis: a 2-year prospective controlled study. Pediatr Rheumatol Online J. 2010;8:30. https://doi.org/10.1186/1546-0096-8-30.
Bachrach LK. Measuring bone mass in children: can we really do it? Horm Res. 2006;65:11–6. https://doi.org/10.1159/000091749.
Wasilewska A, Rybi-Szuminska A, Zoch-Zwierz W, Serum RANKL. Osteoprotegerin (OPG), and RANKL/OPG ratio in nephrotic children. Pediatr Nephrol. 2010;25:2067–75. https://doi.org/10.1007/s00467-010-1583-1.
Levälampi T, Honkanen V, Lahdenne P, Nieminen R, Hakala M, Moilanen E. Effects of infliximab on cytokines, myeloperoxidase, and soluble adhesion molecules in patients with juvenile idiopathic arthritis. Scand J Rheumatol. 2007;36(3):189–93. https://doi.org/10.1080/03009740601089234.
Lerner UH. New molecules in the tumor necrosis factor ligand and receptor superfamilies with importance for physiological and pathologic bone resorption. Crit Rev Oral Biol Med. 2004;15(2):64–81. https://doi.org/10.1177/154411130401500202.
Alkady EA, Rashad SM, Khedr TM, Mossad E, Abdel-Wahab N. Early predictors of increased bone resorption in juvenile idiopathic arthritis: OPG/RANKL ratio, as a key regulator of bone metabolism. Egypt Rheumatologist. 2011;33:217–23. https://doi.org/10.1016/j.ejr.2011.08.001.
Panopalis P, Yazdany J. Bone health in systemic lupus erythematosus. Curr Rheumatol Rep. 2009;11:177–84. https://doi.org/10.1007/s11926-009-0024-2.
Ali R, Hammad A, El-Nahrery E, Hamdy N, Elhawary AK, Eid R, Serum RANKL. Osteoprotegerin (OPG) and RANKL/OPG ratio in children with systemic lupus erythematosus. Lupus. 2019;28(10):1233–42. https://doi.org/10.1177/0961203319867129.
Rouster-Stevens KA, Langman CB, Price HE, Seshadri R, Shore RM, Abbott K, et al. RANKL: osteoprotegerin ratio and bone mineral density in children with untreated juvenile dermatomyositis. Arthritis Rheum. 2007;56(3):977–83. https://doi.org/10.1002/art.22433.
Pocock NA, Eisman JA, Hopper JL, Yeates MG, Sambrook PN, Eberl S. Genetic determinants of bone mass in adults: a twin study. J Clin Invest. 1987;80(3):706–10. https://doi.org/10.1172/JCI113125.
Hofbauer LC, Heufelder AE. The role of osteoprotegerin and receptor activator of nuclear factor κB ligand in the pathogenesis and treatment of rheumatoid arthritis. Arthritis Rheum. 2001;44:253–9. https://doi.org/10.1002/1529-0131(200102)44:2<253::AID-ANR41>3.0.CO;2-S.
Itonaga I, Fujikawa Y, Sabokbar A, Murray DW, Athanasou NA. Rheumatoid arthritis synovial macrophage-osteoclast differentiation is osteoprotegerin ligand-dependent. J Pathol. 2000;192(1):97–104. https://doi.org/10.1002/1096-9896(2000)9999:9999<::AID-PATH672>3.0.CO;2-W.
Eid R, Abdelsalam M, Fathy AA, Abd-El Ghaffar DM, Elmarghany EB, El-Hanafy AA, et al. Predictors of decreased bone mineral density in childhood systemic lupus erythematosus: possible role of osteoprotegerin gene polymorphisms. J Pediatr Endocrinol Metab. 2021;35(1):79–87. https://doi.org/10.1515/jpem-2021-0496. PMID: 34787382.
Zavala-Cerna MG, Moran-Moguel MC, Cornejo-Toledo JA, Gonzalez-Montoya NG, Sanchez-Corona J, Salazar-Paramo M et al. Osteoprotegerin Polymorphisms in a Mexican Population with Rheumatoid Arthritis and Generalized Osteoporosis: A Preliminary Report. J Immunol Res. 2015; 2015:376197. https://doi.org/10.1155/2015/376197.
Petty RE, Southwood TR, Manners P, Baum J, Glass DN, Goldenberg J, et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31:390–2. PMID: 14760812.
Wallace CA, Ruperto N, Giannini E. Preliminary criteria for clinical remission for select categories of juvenile idiopathic arthritis. J Rheumatol. 2004;31:2290–4. PMID: 15517647.
Wallace CA, Giannini EH, Huang B, Itert L, Ruperto N. American College of Rheumatology provisional criteria for defining clinical inactive disease in select categories of juvenile idiopathic arthritis. Arthritis Care Res (Hoboken). 2011;63:929–36.
Consolaro A, Ruperto N, Bazso A, Pistorio A, Magni-Manzoni S, Filocamo G, et al. Paediatric Rheumatology International trials Organisation. Development and validation of a composite disease activity score for juvenile idiopathic arthritis. Arthritis Rheum. 2009;61(5):658–66. https://doi.org/10.1002/art.24516.
Viola S, Felici E, Magni-Manzoni S, Pistorio A, Buoncompagni A, Ruperto N et al. Development and validation of a clinical index for assessment of long-term damage in juvenile idiopathic arthritis. Arthritis Rheum.2005; 52:2092–102. https://doi.org/10.1002/art.21119. PMID: 15986372.
Soufi M, Schoppet M, Sattler AM, Herzum M, Maisch B, Hofbauer LC, et al. Osteoprotegerin gene polymorphisms in men with coronary artery disease. J Clin Endocrinol Metab. 2004;89:3764–8. https://doi.org/10.1210/jc.2003-032054.
Pitocco D, Zelano G, Gioffre G, Di Stasio E, Zaccardi F, Martini F et al. Association between osteoprotegerin G1181C and T245G polymorphisms and diabetic charcot neuroarthropathy: Acase-control study. Diabetes Care 209; 32:1694–7. https://doi.org/10.2337/dc09-0243.
El-Ziny MA, Al-Tonbary YA, Salama OS, Bakr AA, Al-Marsafawy H, Elsharkawy AA. Low turnover bone disease in egyptian children with acute leukemia. Hematology. 2005;10:327–33. https://doi.org/10.1080/10245330500155598.
El-Ziny MA, Al-Tonbary YA, Salama OS, Bakr AA, Al-Marsafawy H, Elsharkawy AA. Low bone mass in children with malignant lymphoma. Pediatr Hematol Oncol. 2007;24:577–85. https://doi.org/10.1080/08880010701640275.
Binkley N, Bilezikian JP, Kendler DL, Leib ES, Lewiecki EM, Petak SM, International Society for Clinical Densitometry. Official positions of the International Society for Clinical Densitometry and Executive Summary of the 2005 Position Development Conference. J Clin Densitom. 2006;9(1):4–14. https://doi.org/10.1016/j.jocd.2006.05.002.
Consolaro A, Giancane G, Schiappapietra B, Davì S, Calandra S, Lanni S, Ravelli A. Clinical outcome measures in juvenile idiopathic arthritis. Pediatr Rheumatol Online J. 2016;14(1):23. https://doi.org/10.1186/s12969-016-0085-5.
Al-Mayouf SM, Al Mutairi M, Bouayed K, Habjoka S, Hadef D, Lotfy HM et al. Epidemiology and demographics of juvenile idiopathic arthritis in Africa and Middle East. Pediatr Rheumatol Online J. 2021 Dec 2;19(1):166. https://doi.org/10.1186/s12969-021-00650-x.
Thierry S, Fautrel B, Lemelle I, Guillemin F. Prevalence and incidence of juvenile idiopathic arthritis: a systematic review. Joint Bone Spine. 2014;81(2):112–7. https://doi.org/10.1016/j.jbspin.2013.09.003.
Dagher R, Assi S. Juvenile idiopathic arthritis: a single center lebanese study. Pediatr Rheumatol. 2014;12:179. https://doi.org/10.1016/j.jbspin.2013.09.003.
Demirkaya E, Ozen S, Bilginer Y, Ayaz NA, Makay BB, Unsal E, et al. The distribution of juvenile idiopathic arthritis in the eastern Mediterranean: results from the registry of the turkish Paediatric Rheumatology Association. Clin Exp Rheumatol. 2011;29(1):111–6. PMID: 21269582.
Hussein ZM, Wagdy R, Shawki M, Zohni S, Shehawy I. The pattern of juvenile idiopathic arthritis; a retrospective egyptian study. Egypt J Pediatr Allergy Immunol. 2018;16(1):7–14. https://doi.org/10.21608/ejpa.2018.10417.
Consolaro A, Giancane G, Alongi A, van Dijkhuizen EHP, Aggarwal A, Al-Mayouf SM, et al. Phenotypic variability and disparities in treatment and outcomes of childhood arthritis throughout the world: an observational cohort study. Lancet Child Adolesc Health. 2019;3(4):255–63. https://doi.org/10.1016/S2352-4642(19)30027-6.
Al-Mayouf SM, Hashad S, Khawaja K, Alrasheedi A, Abdwani R, Abushhaiwia A, et al. Cumulative damage in juvenile idiopathic arthritis: a Multicenter Study from the Pediatric Rheumatology Arab Group. Arthritis Care Res (Hoboken). 2021;73(4):586–92. https://doi.org/10.1002/acr.24436.
Abdwani R, Abdalla E, Al Abrawi S, Al-Zakwani I. Epidemiology of juvenile idiopathic arthritis in Oman. Pediatr Rheumatol Online J. 2015;13:33. https://doi.org/10.1186/s12969-015-0030-z.
Al-Abrawi S, Al-Mayouf SM, Abdwani R, Abdalla E, Consolaro A, Bovis F, et al. The Omani Arabic version of the Juvenile Arthritis Multidimensional Assessment Report (JAMAR). Rheumatol Int. 2018;38(1):299–306. https://doi.org/10.1007/s00296-018-3965-9.
Saurenmann RK, Rose JB, Tyrrell P, Feldman BM, Laxer RM, Schneider R, et al. Epidemiology of juvenile idiopathic arthritis in a multi-ethnic cohort: ethnicity as a risk factor. Arthritis Rheum. 2007;56(6):1974–84. https://doi.org/10.1002/art.22709.
Sušić G, Pilipović N, Stojanović R. Bone Mineral density in patients with juvenile idiopathic arthritis. Srp Arh Celok Lek. 2009;137(7–8):396–401. https://doi.org/10.2298/sarh0908396s.
Galindo Zavala R, Núñez Cuadros E, Martín Pedraz L, Díaz-Cordovés Rego G, Sierra Salinas C, Urda Cardona A. Low bone mineral density in juvenile idiopathic arthritis: prevalence and related factors. An Pediatr (Barc). 2017;87(4):218–25. https://doi.org/10.1016/j.anpedi.2016.12.005.
Stagi S, Cavalli L, Signorini C, Bertini F, Cerinic MM, Brandi ML, et al. Bone mass and quality in patients with juvenile idiopathic arthritis: longitudinal evaluation of bone-mass determinants by using dual-energy x-ray absorptiometry, peripheral quantitative computed tomography, and quantitative ultrasonography. Arthritis Res Ther. 2014;16(2):R83. https://doi.org/10.1186/ar4525.
Islam MF, Islam MI, Talukdar MK, Rahman SA. Bone mineral density in children with juvenile idiopathic arthritis: a hospital-based study. Bangladesh J Child Health. 2013;37:18–21. https://doi.org/10.3329/bjch.v37i1.15347.
Thornton J, Pye SR, O’Neill TW, Rawlings D, Francis RM, Symmons DP, et al. Bone health in adult men and women with a history of juvenile idiopathic arthritis. J Rheumatol. 2011;38(8):1689–93. https://doi.org/10.3899/jrheum.101232.
Charuvanij S, Malakorn H, Densupsoontorn N, Nakavachara P. Bone Mineral density and serum 25OHD in children and adolescents with juvenile idiopathic arthritis. Clin Pediatr (Phila). 2022 Nov 10:99228221136982. https://doi.org/10.1177/00099228221136982. Epub ahead of print.
El Badri D, Rostom S, Bouaddi I, Hassani A, Chkirate B, Amine B, et al. Bone Mineral density in moroccan patients with juvenile idiopathic arthritis. J Arthritis. 2014;3:131. https://doi.org/10.11604/pamj.2014.17.115.1838.
Tsentidis C, Gourgiotis D, Kossiva L, Doulgeraki A, Marmarinos A, Galli-Tsinopoulou A, et al. Higher levels of s-RANKL and osteoprotegerin in children and adolescents with type 1 diabetes mellitus may indicate increased osteoclast signalling and predisposition to lower bone mass: a multivariate cross-sectional analysis. Osteoporos Int. 2016;27(4):1631–43. https://doi.org/10.1007/s00198-015-3422-5.
Ozkaya O, Buyan N, Bideci A, Gonen S, Ortac E, Fidan K, et al. Osteoprotegerin and RANKL serum levels and their relationship with serum ghrelin in children with chronic renal failure and on dialysis. Nephron Clin Pract. 2007;105(4):c153–8. https://doi.org/10.1159/000099005.
Spelling P, Bonfa ́ E, Caparbo VF, Pereira RM. Osteoprotegerin/ RANKL system imbalance in active polyarticular-onset juvenile idiopathic arthritis: a bone damage biomarker? Scand J Rheumatol. 2008;37:439–44. https://doi.org/10.1080/03009740802116224.
Buzi F, Maccarinelli G, Guaragni B, Ruggeri F, Radetti G, Meini A, et al. Serum osteoprotegerin and receptor activator of nuclear factors kB (RANKL) concentrations in normal children and in children with pubertal precocity, Turner’s syndrome and rheumatoid arthritis. Clin Endocrinol (Oxf). 2004;60(1):87–91. https://doi.org/10.1111/j.1365-2265.2004.01951.x.
Masi L, Simonini G, Piscitelli E, Del Monte F, Giani T, Cimaz R, et al. Osteoprotegerin (OPG)/RANK-L system in juvenile idiopathic arthritis: is there a potential modulating role for OPG/RANK-L in bone injury? J Rheumatol. 2004;31(5):986–91. PMID: 15124262.
Sarma PK, Misra R, Aggarwal A. Elevated serum receptor activator of NFkappaB ligand (RANKL), osteoprotegerin (OPG), matrix metalloproteinase (MMP)3, and ProMMP1 in patients with juvenile idiopathic arthritis. Clin Rheumatol. 2008;27(3):289–94. https://doi.org/10.1007/s10067-007-0701-3.
Varsani H, Patel A, van Kooyk Y, Woo P, Wedderburn LR. Synovial dendritic cells in juvenile idiopathic arthritis (JIA) express receptor activator of NF-kappaB (RANK). Rheumatol Oxf. 2003;42:583–90. PMID: 12649407.
Agarwal S, Misra R, Aggarwal A. Synovial fluid RANKL and matrix metalloproteinase levels in enthesitis related arthritis subtype of juvenile idiopathic arthritis. Rheumatol Int. 2009;29:907–11. https://doi.org/10.1007/s00296-008-0805-3.
Shalaby RH, Kassem EM, El-Gazzar NM, Hammoudah SAF, El-Barbary AM. P013 serum osteoprotegerin and RANKL in patients with juvenile idiopathic arthritis and their correlation with bone mineral density. Rheumatology. 2021;60(5). https://doi.org/10.1093/rheumatology/keab722.005.
Geusens PP, Landewé RB, Garnero P, Chen D, Dunstan CR, Lems WF, et al. The ratio of circulating osteoprotegerin to RANKL in early rheumatoid arthritis predicts later joint destruction. Arthritis Rheum. 2006;54(6):1772–7. https://doi.org/10.1002/art.21896.
Shunle C. The significance of the RANKL and OPG gene expression in the initial systemic lupus erythematosus patients. Chin J Osteoporos. 2009;1:36–9.
Zhizho Y, Bo L, Jianso L, Fenlia G, Junhan Z. Bone mineral density in patients with juvenile rheumatoid arthritis. Pediatr Rheumatol Online J. 2008;6(1):P80. https://doi.org/10.1186/1546-0096-6-S1-P80.
Davies JH, Evans BA, Jenney ME, Gregory JW. Skeletal morbidity in childhood acute lymphoblastic leukaemia. Clin Endocrinol (Oxf). 2005;63(1):1–9. https://doi.org/10.1111/j.1365-2265.2005.02263.x.
Lahdenne P, Vähäsalo P, Honkanen V. Infliximab or etanercept in the treatment of children with refractory juvenile idiopathic arthritis: an open label study. Ann Rheum Dis. 2003;62(3):245–7. https://doi.org/10.1136/ard.62.3.245.
Simonini G, Giani T, Stagi S, de Martino M, Falcini F. Bone status over 1 year of etanercept treatment in juvenile idiopathic arthritis. Rheumatology (Oxford). 2005;44:777–80. https://doi.org/10.1093/rheumatology/keh592.
Vojvodich PF, Hansen JB, Andersson U, Sävendahl L, Hagelberg S. Etanercept treatment improves longitudinal growth in prepubertal children with juvenile idiopathic arthritis. J Rheumatol. 2007;34(12):2481-5. PMID: 18050366.
Honore P, Luger NM, Sabino MA, Schwei MJ, Rogers SD, Mach DB et al. Osteoprotegerin blocks bone cancer-induced skeletal destruction, skeletal pain and pain-related neurochemical reorganization of the spinal cord. Nat Med. 2000;6(5):521-8. https://doi.org/10.1038/74999. Erratum in: Nat Med 2000;6(7):838.
Bateman TA, Dunstan CR, Ferguson VL, Lacey DL, Ayers RA, Simske SJ. Osteoprotegerin mitigates tail suspension-induced osteopenia. Bone. 2000;26:443–9. https://doi.org/10.1016/S8756-3282(00)00256-8.
Bekker PJ, Holloway D, Nakanishi A, Arrighi M, Leese PT, Dunstan CR. The effect of a single dose of osteoprotegerin in postmenopausal women. J Bone Miner Res. 2001;16(2):348–60. https://doi.org/10.1359/jbmr.2001.16.2.348.
Acknowledgements
N/A
Funding
No funding received.
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Contributions
RE: research hypothesis and protocol, statistical analysis, wrote the initial draft, revised, and approved the final manuscript. HMA: BMD assessment to all subjects, provided medical care to some patients, revised and approved the final manuscript. NH, DSA: revised, approved the final manuscript, and provided medical care to some patients.DMA, EBE: provided medical care to all patients, collected clinical data of all subjects, revised and approved the final manuscript.MA, AAE: performed al laboratory workup, interpretation of the results, revised, and approved the final manuscript. AAF, NAN: shared in statistical analysis, revised and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
The study was reviewed and approved by Mansoura Faculty of Medicine Institutional Research Board (MFM-IRB) (R.23.01.2019.R1).
Consent to participate
Informed consent was obtained from legal guardians for all study participants.
Consent for publication
N/A.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Eid, R., Abdelsalam, M., Fathy, A.A. et al. Bone mineral density in egyptian children with juvenile idiopathic arthritis: possible correlation to serum RANKL / osteoprotegerin (OPG) ratio and OPG gene polymorphisms. Pediatr Rheumatol 21, 58 (2023). https://doi.org/10.1186/s12969-023-00843-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12969-023-00843-6