
Abstract
Background
The Early Childhood Oral Health Impact Scale (ECOHIS) measures the impact of dental diseases on Oral Health-Related Quality of Life both in children and their families. The aim of this study was to develop a Chilean Spanish version of the ECOHIS that is conceptually equivalent to the original and to assess its acceptability, reliability and validity in the preschool population of Chile.
Methods
The Chilean version of the ECOHIS was obtained through a process including forward and back-translation, expert panel, and cognitive debriefing interviews. To assess metric properties, a cross-sectional study was carried out in Carahue, Southern Chile (April–October 2016). Children younger than six years old without systemic diseases, disabilities or chronic medication from eleven public preschools were included. Parents were invited to complete the Chilean version of the ECOHIS, PedsQL™4.0 Generic Core and PedsQL Oral Health scales, and to answer global questions about their children’s general and oral health. A subsample was administrated ECOHIS a second time 14–21 days after. A clinical examination was performed to assess dental caries, malocclusion, and traumatic dental injuries. Reliability was evaluated using measures of internal consistency (Cronbach’s alpha) and reproducibility (Intraclass correlation coefficient - ICC). Construct validity was assessed by testing hypotheses based on available evidence about known groups and relationships between different instruments.
Results
The content comparison of the back-translation with the original ECOHIS showed that all items except one were conceptually and linguistically equivalent. The cognitive debriefing showed a suitable understanding of the Chilean version by the parents. In the total sample (n = 302), the ECOHIS total score median was 1 (IQR 6), floor effect was 41.6%, and ceiling effect 0%. Cronbach’s alpha was 0.89 and the ICC was 0.84. The correlation between ECOHIS and PedsQL™4.0 Generic Core was weak (r = 0.21), while it was strong-moderate (r = 0.64) with the PedsQL Oral Health scale. In the known groups comparison, the ECOHIS total score was statistically higher in children with poor than excellent/very good oral health (median 11.6 vs 0, p < 0.01), and in the high severity than in the caries-free group (median 8 vs 0.5, p < 0.01). No differences were found according to malocclusion and traumatic dental injuries groups.
Conclusions
These results supported the feasibility, reliability and validity of the Chilean version of ECOHIS questionnaire for preschool children through proxy.
Similar content being viewed by others


Background
Oral diseases are highly prevalent in children worldwide despite the improvement in oral health indices initiated in the last decades [1,2,3]. It is well known that their consequences on children are serious and can affect their quality of life [4,5,6,7,8]. Early childhood caries continues to be a serious public health problem in Chile, with a prevalence that can reach 80% at 4 years of age [9,10,11]. Oral Health-Related Quality of Life (OHRQoL), together with clinical indicators, can jointly provide a more comprehensive assessment of the patient’s oral health [12]. The OHRQoL has been defined as a multidimensional concept which includes a subjective evaluation of the individual’s oral health, functional well-being, expectations and satisfaction with care, and their sense of self [12].
The knowledge of the OHRQoL might help to improve the development of effective oral health programs and services because it permits the assessment of young children’s perceived needs, and treatment strategy effectiveness [13]. This can contribute to the identification of groups with a higher level of need, to prioritize public health programs for care of children and adolescents, and to improve access to care [14]. The use of OHRQoL as an outcome measure is consistent with patient-centered care, being crucial in understanding the effectiveness of treatment from the patients’ perspective [12].
Several instruments have been developed to assess the OHRQoL, yet few of them have been specifically designed for preschoolers. The first OHRQoL questionnaire for this age group was the Michigan Oral Health-Related Quality of Life (Michigan OHRQoL) in 2003 [15]. Subsequently, the Early Childhood Oral Health Impact Scale (ECOHIS) was developed in 2007 [16], the Pediatric Oral Health-Related Quality of Life (POQL) in 2011 [17] and the Scale of Oral Health Outcomes for 5-year-olds (SOHO-5) in 2012 [18]. POQL and the ECOHIS measure the OHRQoL impact of dental diseases not only on the children, but also on their families. It is important because oral health conditions have an indirect impact on parents and family members, because they result in lost workdays or in having to spend time and money on dental care [19, 20]. The ECOHIS demonstrated high reliability [21, 22], good validity [23, 24] and responsiveness [25, 26], and it has been adapted into about 10 languages and countries [21,22,23,24, 27,28,29,30,31], including Spanish for Argentina [32].
Culture is an important factor that can influence a person’s activities, thinking and behavior. As countries differ regarding public health strategies, attitudes, socioeconomic conditions and other factors, the expression of their culture can change between populations [33], and instruments to measure Health Related Quality of life (HRQoL) should go through a cultural adaptation process before being used in a different country. Therefore, even among Spanish speaking countries it is usual to develop country-specific versions of instruments measuring HRQoL [34,35,36]. Even when the translation is performed with great precision, cultural factors may not be accurately conveyed. In order to study the health care needs of people with diverse cultural backgrounds, research instruments must be reliable and valid in each culture studied [37].
The aim of this study was to develop a Chilean Spanish version of the Early Childhood Oral Health Impact Scale (ECOHIS) that is conceptually equivalent to the original and to assess the acceptability, reliability and validity of this version in the preschool population of Chile.
Methods
The study was performed in two phases. In the first phase, the scale was translated into Spanish and adapted to the Chilean culture. In the second phase, the psychometric properties were tested among a sample of parents of preschool children. The Ethics Committee of the Universidad de La Frontera approved the study protocol (resolution n° 061/2015).
Early childhood Oral Health impact scale (ECOHIS)
The ECOHIS is a proxy-reported questionnaire developed in USA for measuring the OHRQoL of preschool children and their families [16]. It comprises of 13 items, covering six domains in two sections. The child’s impacts section contains 4 domains: symptom (1 item), function (4 items), psychology (2 items) and self-image and social interaction (2 items). The family’s impacts section contains 2 domains: parental distress (2 items) and family function (2 items). Response categories for each question are rated on a 5-point Likert scale to record how often an event has occurred during the child’s life: 0 = never, 1 = hardly ever, 2 = occasionally, 3 = often, 4 = very often, and 5 = don’t know. ECOHIS scores are calculated as a simple sum of the response codes for the child and family sections separately and also a total score, after recoding all “Don’t know” responses as “missing”. In cases with up to 2 missing responses in the child section or 1 missing response in the parent section, they were ascribed the average score of the rest of the items for that section. Parents missing responses to more than two child items and one family item were excluded from the analysis. Thus, the total score ranges between 0 and 52, with higher scores indicating a greater impact of oral problems and therefore worse OHRQoL [16].
Linguistic and cultural adaptation
Standard methods were used to translate and culturally adapt the instrument [38, 39]. The Spanish translation of the ECOHIS was carried out independently by two professional linguists, both native Chilean Spanish speakers, with a high level of fluency in English. The focus of these forward translations was achieving a conceptual, rather than literal, equivalence. In addition each translator scored the difficulty in finding the conceptual equivalence in translation of each of the items from 1 (least difficulty) to 10 (maximum difficulty). To obtain a first consensual version, a joint revision of the two Chilean Spanish translations was undertaken by a panel composed of two experts in OHRQoL assessment, two pediatric dentists and the two translators. Then this first Chilean version was reviewed by a panel of parents of pre-school children (3 fathers and 4 mothers) to check its understanding and clarity. This pre-final version was translated back into English by two native American-English speakers. The difficulty in finding the linguistic equivalence in back-translation was also evaluated by translators. The equivalence between the original version and back-translation was evaluated by the expert panel who rated the items as: A (conceptually and linguistically equivalent to the original item), B (functionally equivalent, but with grammatical differences), or C (equivalence is not obvious). The report on equivalence between original and back-translated versions was sent to the authors of the original ECOHIS for evaluation.
As a last step, cognitive debriefing interviews were carried out on 15 parents (2 fathers and 13 mothers, aged 24 to 37 years old) of children between 2 and 5 years of age to evaluate the understandability and clarity of this preliminary version. Cognitive debriefing interviews included: first, asking parents to complete the questionnaire independently; and second, performing additional open questions in an effort to assess the content of the adaptation. This technique allowed assessing what the parents understood in the adapted version. For this purpose, we developed a set of questions to be used during the interview to obtain standardized information, such as: “In your own words, what do you think this question is asking? What does this item mean to you?” (Supplementary data). We recorded the conversations and took notes during the cognitive interviews. Then, we transcribed the audiotapes to prepare an item-by-item summary of each section of the questionnaire and modification recommendations if necessary.
Study of the metric properties
A cross-sectional study was carried out in the city of Carahue, Southern Chile, from April 2016 through October 2016 to test the psychometric properties of the Chilean version of ECOHIS. Eleven public preschools were included, which are funded by the Chilean government for children younger than six years old.
Two- to 5-year-old children without any systemic diseases, disabilities or chronic medication were included. A written consent from the parents was obtained and the children gave their verbal consent for considering their participation in the study. The parents were invited to a meeting in the school, during which a dental examination of the participating children was performed and parents were asked to self-complete three questionnaires on their child: one measuring general HRQoL (PedsQL™4.0 Generic Core scale for toddlers), and two on OHRQoL (ECOHIS and PedsQL Oral Health). In addition, the parents completed a structured questionnaire to compile information on the child’s age, gender, socioeconomic status, history of oral hygiene habits, as well as their overall and dental health status. We sent by regular mail the questionnaires to parents who did not attend the meeting.
Three experienced researchers performed the dental examinations in the classroom. After cleaning the tooth surfaces with a toothbrush, a visual inspection of the oral cavity was performed under artificial light. The examiners were blinded to the questionnaire responses. The diagnosis of caries was based on the criteria proposed by the World Health Organization in the Oral Health Survey Basic Methods for Epidemiological Studies [40]. The types of traumatic dental injury were classified according to Andreasen & Andreasen [41] and the malocclusion was assessed according to the presence or absence of at least one of the following: anterior open bite, overjet > 4 mm and anterior cross-over bite [4].
Prior to beginning the study, the researchers were trained in dental examination to increase the degree of inter-examiner agreement. The training consisted of a stage in which the examination teams, each composed of an examiner and a recorder, received theoretical training on the study protocol and diagnostic criteria, as well as on how to complete a clinical record and a systematic dental examination. A group of 15 children were then examined to test the inter-examiner agreement on caries and malocclusions traits, with kappa coefficients of 0.83 and 0.70, respectively. A series of 20 pictures were used to assess reliability on traumatic dental injury (kappa = 0.79).
Sample size
According to sample size recommendations to assess construct validity, ceiling/floor effects, internal consistency and factorial analysis, 2 to 20 participants per item are required, with an absolute minimum of 100 to 250 subjects [42,43,44]. Considering that the highest number of participants recommended per item is 20, and assuming a 15% of potential missing answers, the sample size required was of 300 children.
Statistical analysis
A descriptive analysis of the sociodemographic characteristics and the results of the oral examination was performed. Mean, standard deviations, score range, and percentage of patients with the lowest (floor effect) and highest theoretical scores (ceiling effect) were calculated in order to examine the scores’ distribution of the ECOHIS. Reliability was assessed following two approaches: internal consistency was evaluated using Cronbach’s alpha; and test-retest reproducibility was assessed using the intraclass correlation coefficient (ICC) calculated by two-way random effects analysis of variance. Test-retest subsample was selected by randomization of 50% of the participants at each school, who received the questionnaires by mail 2–4 weeks after the school meeting. Parents who reported change in their child’s oral health status were excluded of this analysis.
Confirmatory Factor Analysis (CFA) was performed to assess the measurement model of the ECOHIS. To test the structure in two sections proposed by developers of ECOHIS (Child and Family impact sections), as well as for the existence of a general factor (the ECOHIS total score), a 2nd order model structure was imposed in the CFA. The CFA was performed using the robust unweighted least squares (ULSMV), and its goodness of fit was assessed using the Confirmatory Fit Index (CFI) and the Tucker-Lewis Index (TLI), which should be above 0.95, and the Root Mean Square Error of Approximation (RMSEA), which indicates an adequate fit below 0.08. The CFA was conducted with MPlus 5 [45].
Construct validity evaluation was based on known groups defined by results of dental examination (caries, traumatic dental injuries and malocclusion) and by responses from the parents about the child’s overall and dental health with a 5-Likert scale (Excellent, Very Good, Good, Fair, and Poor). We hypothesized worse child OHRQL (higher scores on the two sections of the ECOHIS) among children with some dental disease identified in the dental examination and among those whose overall and dental health was rated as fair or poor. Given the clearly skewed distribution of the ECOHIS score, we decided to use nonparametric analysis and Kruskal-Wallis or Mann Whitney tests were used to assess ECOHIS differences among these groups. To quantify the magnitude of the difference, effect size was calculated as the difference between means divided by the standard deviation pooled from the two groups. Effect sizes of 0.2, 0.5 and 0.8 were defined as small, moderate and large, respectively [46].
Additionally, to examine convergent and discriminant validity, correlations of ECOHIS scores with the PedsQL™4.0 Generic Core and PedsQL Oral Health scales were calculated using Spearman correlation coefficients, interpreted as follows: negligible relationship when r is < 0.20; weak when 0.20–0.40; moderate when 0.40–0.60; strong-moderate when 0.60–0.80; and strong relationship when > 0.80 [47]. Convergent validity involves demonstrating that different instruments measuring a similar concept inter-correlate at least moderately. We hypothesized moderate to strong correlation coefficients between ECOHIS and PedsQL Oral Health, since both were designed to measure OHRQoL. In contrast, discriminant validity is the extent to which a measure does not correlate too strongly with those measures intended to assess different traits. Therefore, we hypothesized that correlations between ECOHIS and PedsQL™4.0 Generic Core is low, due to differences between OHRQoL and HRQoL. The data analyses were performed using Stata 13 (Stata Corp, College Station, TX, USA).
Results
Cross-cultural adaptation process
The average difficulty for the forward translation of the items into Chilean Spanish was < 2.5. Regarding the back-translation, the average difficulty was of 7.5 for item 13, 6 for item 8, 5.5 for item 12 and below or equal to 4.5 for the rest (Fig. 1). For content comparison between back-translation and the original version, the expert panel rated all items as A (conceptually and linguistically equivalent), except item 13 which was rated as C (equivalence is not obvious). This was due to the replacement of the term “financial impact” by “important economic cost” after members of the panel of pre-school children parents claimed they did not understand the first expression. The author of the original ECOHIS reviewed the Spanish and the English back-translated versions without identifying any lack of equivalence regarding the original.

Average difficulty to find the conceptual equivalence, as reported by translators in the forward and back-translations
Finally, the cognitive debriefing showed that the instructions, items and response choice were easy to understand by parents. The parents thought about the whole vital cycle of their child when answering the questions. Some parents had difficulty defining in their own words the terms “frustrated” and “irritable”, however they were able to differentiate between them. None of the parents had problems to differentiate among the different response options. All parents agreed that the questions are intended to evaluate OHRQoL. No modification was necessary as a result of the cognitive debriefing interviews.
Psychometric study
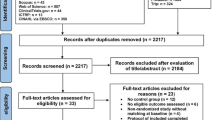
The population of Carahue preschools included a total of 435 children, two of them were excluded for presenting special health care needs, twelve because their parents did not sign the informed consent, and 93 children were absent at the time of dental examination. Of the 328 parents included, 26 did not return the questionnaires (response rate = 92.1%). In total, 302 children were fully evaluated (Table 1), comprising 163 boys and 139 girls, with an average age of 4.0 (SD = 1.1) years. Most were of low socioeconomic status, 40.9% of the parents reported that their children have good general health and 36.5% good oral health. The prevalence of dental caries, malocclusion and traumatic dental injuries was 53.6, 39.4 and 14.5% respectively.
Table 2 shows the children’s parents extreme ECOHIS responses and reliability coefficients. All items were rated as “never” by over 60% of parents. The two items most frequently rated as “never” were in the child section: “avoided smiling or laughing” (92.4%) and “avoided talking” (93.7%). The two items most frequently rated as “very often” were in the family section, parents or family members having “been upset” (1.9%) and “feel guilty” (3.6%). The Cronbach’s alpha coefficient was 0.89 for the total score showing a good correlation within items. Among the subsample of 84 parents who completed the ECOHIS twice, the Intraclass Correlation Coefficient was 0.84 for the total score. Both reliability coefficients were above the recommended standard of 0.7 in the child and the family sections.
The measurement model consisted of two specific factors and a general factor (Fig. 2). Factor 1 includes the nine items composing the Child Impact Section; factor 2 includes the 4 items composing the Family Impact Section; and the latent construct for the total score includes both factors (Child and Family Impact). This CFA model presented excellent goodness of fit coefficients: CFI = 0.978, TLI = 0.988 and RMSEA = 0.065.

Confirmatory factor analysis to assess the measurement model of the ECOHIS
Distributions of the ECOHIS scores are presented in Table 3. The median of the total ECOHIS score was 1 (IQR 6), for child impact it was 1 (IQR 3) and 0 (IQR 2) for the family impact section. In the child impact section, 5.0% of the parents answered “Don’t Know” in at least one item and 1.7% in the family impact section. The floor effect was 41.6% and ceiling effect was negligible for the total score.
Table 4 shows the results of the construct validity of ECOHIS based on known groups. As the child’s general health and oral health was rated worse by parents, the ECOHIS median total score was higher, but differences among groups were only statistically significant for oral health: from 0 when excellent/very good to 11.6 when poor (p < 0.01). Finally, regarding dental diseases, ECOHIS scores presented statistically significant differences among groups defined by dental caries (median 0.5, 2, and 8, p < 0.01), but differences between presence or absence of malocclusion or type of traumatic dental injuries were not significant. Effect sizes indicate large differences between groups defined by child’s oral health and dental caries.
Table 5 shows that the correlation of the total score of ECOHIS with the PedsQL™4.0 was strong-moderate with the Oral Health scale (r = 0.64), weak with the Generic Core scale (r = 0.21), and also when both scales were considered (r = 0.35). Finally, the correlation between the child and the family impact sections of ECOHIS was moderate (r = 0.57; p ≤ 0.001).
Discussion
We used a standard cross-cultural adaptation process to develop the Chilean version of the ECOHIS, which demonstrated good acceptability by parents; high reliability and good construct validity. The results are consistent with those obtained for the original ECOHIS and suggest that the Chilean version is conceptually and metrically equivalent.
“Don’t know” and/or missing responses may reflect comprehensibility problems [24]. In our sample, only one parent left some missing items and only 19 (6.3%) responded “Don’t know”, similarly to the original ECOHIS study (7%) [16]. However, other studies have shown higher “Don’t know” percentages [19,20,21,22]. The low percentage of “Don’t know” supports that the mode of administration (proxy-report) is not a limitation for the ECOHIS Chilean version. According to the ECOHIS proxy-report design [16], in our study most parents completed it during the school meeting, and those who did not attend it completed the questionnaire at home. No interview administration was needed, and no one required assistance to self-complete the questionnaire. Self-administration presents advantages, such as lower cost, preservation of participant’s anonymity, and reduction of interviewer bias [48]. Furthermore, studies with other OHRQoL instruments showed that administration mode (interview versus self-administered) does not influence the instruments’ scores [48,49,50]. On the other hand, evidence shows that parents underestimate the impact of children’s oral health problems, since they have a different perspective and limited knowledge, particularly related to social and emotional well-being [51]. Indeed, oral health problems directly observable by parents, such as physical complaints and functionality, concur better with children’s perceptions [52, 53]. However, in this age group due to their cognitive immaturity, limited social experience and continued dependency, parents are the best source of their child’s oral health [54]. As in the original version, we included parents with “Don’t know” responses in the analysis because a “Don’t know” response reflects an essential characteristic of the phenomenon under evaluation, rather than errors by the respondents [55].
The high floor effect observed in the total score (41.6%) and domain or section scores (ranging 49–92%) is congruent with the clinical characteristics of our participants, since over 40% of the sample was free of oral conditions. Although these results are similar to those obtained in other studies, which have also shown a strong floor effect for ECOHIS total score (ranging 20–54%) [16, 24, 29] they could indicate a limitation of the instrument. The ECOHIS Chilean version needs to be tested in a population with more oral problems to assess adequately the instrument’s more severe response levels. The ECOHIS has shown an excellent reliability, both in its internal consistency and its reproducibility, since its coefficient values were over 0.8 allowing to use its scores for the comparison between groups [56]. Our result of internal consistency for the child section (Cronbach’s alpha coefficient = 0.88) was similar to the 0.91 reported by the original English questionnaire, but it was lower for the family impact section (0.80 vs. 0.95). However, with exception of the original version, the family section usually shows a lower internal consistency (Cronbach’s alpha ranging 0.59–0.85) than the child impact section (ranging 0.74–0.92) [21, 22, 29], which may be due to the lower number of items rather than a lower consistency. In the test-retest reliability, the ICC for total score was the same as reported in the original version (0.84), but lower than reported in the French (0.95) [24] and Brazilian versions (ranging 0.94–0.99) [22, 57]. Despite this, the ICC value shows that the Chilean version of ECOHIS has an excellent test-retest reliability in which it is able to produce reproducible scores when it is administered at two different times [43].
The good results on equivalence with the original ECOHIS shown by its comparison with the back-translation of the Chilean-adapted version support the content validity of this new country version. The higher difficulty of the back-translation compared to the forward one, observed in our adaptation process, has been also described for other adapted instruments [58, 59]. As the first translation seeks conceptual equivalence, and the second one seeks a literal translation of the expressions, this back-translation can often be harder to carry out.
To the best of our knowledge, there is no previous publication describing the factor structure of the ECOHIS. Our results confirm the two- section structure proposed by the developers (child and family impact sections), as well as that correlations between them can be explained by the second order model representing the global OHRQoL. The confirmation of this measurement model in other country versions of the ECOHIS would be recommendable.
For construct validity, the Chilean version of the ECOHIS scale showed significant differences among groups defined by the children’s dental health status as reported by parents. These findings were consistent with previous studies where parents who perceived their child’s oral health as poor had significantly higher mean ECOHIS scores [16, 21, 24, 27]. Our results showed higher ECOHIS scores among those with more than 6 decayed teeth, compared to those who had 1–5 decayed teeth or to those who were caries-free. The large effect size in children with poor oral health status reported by parents and who have high severity of caries supports the parents’ recognition of oral health problems when they become evident, or when it manifests in the form of pain [60]. However, the ECOHIS was not able to discriminate presence or absence of malocclusion or type of traumatic dental injuries. Although the ECOHIS was originally developed to assess the impact of dental caries, it has been widely used to evaluate several oral pathologies [4, 61], but only few studies have validated this application: Peker et al. only found a moderate correlation with gingival index [21], and Scarpelli et al. showed a statistically significant association with discolored upper anterior teeth [22]. This is important because the ECOHIS has been used to measure OHRQoL in patients with traumatic dental injuries or malocclusion, not detecting any impact on the children [4, 62]. Further research is needed to explore whether this absence of impact can be due to the inability of the instrument to discriminate between certain degrees of these pathologies.
The poor correlation between ECOHIS and PedsQL™4.0 Generic Core scale suggests that ECOHIS captures additional information, which is not covered by instruments measuring HRQoL. This is in line with results reported by Lee et al., showing that the ECOHIS is more sensitive than PedsQL™4.0 measuring the impact of oral problems on preschool children [63]. As expected, a high correlation was found with the Oral Health scale of PedsQL™4.0 because it also could be considered specific for measuring OHRQoL [64, 65]. The moderate correlation between the child and the family impact sections of the scale found in our sample (r = 0.57) was similar to results reported in previous studies ranging 0.36–0.68 [16, 21, 27]. The correlation in the original English questionnaire between both sections was the lowest (Spearman’s r = 0.36, p ≤ 0.001), and the Turkish version the strongest (Spearman’s r = 0.68, p ≤ 0.001). Although child and family sections assess different aspects of child’s OHRQoL, both sections are related with the underlying construct.
The main limitation of this study was the homogeneity of the sample studied, since only preschoolers from public schools were included. Nonetheless, our sample is representative of children between 2 and 5 years old attending public preschools, and these children are the main target of Oral Health Policies in Chile. Another limitation was that information regarding the parents, such as age, gender, and educational level, was not registered. Finally, the responsiveness was not assessed; therefore, future studies are necessary to evaluate the capacity of the ECOHIS Chilean version to detect changes over time in a clinical or public health intervention.
Conclusions
The Chilean version of the Early Childhood Oral Health Impact Scale was valid and reliable for assessing the OHRQoL in preschool children through proxy. The comparison with the original U.S. version shows similar results in reliability and validity, suggesting that the cross-cultural adaptation method followed has yielded an equivalent Chilean version.
Researchers and clinicians now have at their disposal an OHRQoL instrument for use in Chilean preschool children to assess the impact of oral disorders on them and their families, and also to facilitate the identification of groups at a higher risk of dental health inequity to improve their access to oral health care services.
Abbreviations
- dmft:
-
Decayed, missing and filled teeth index
- ECOHIS:
-
Early Childhood Oral Health Impact Scale
- HRQoL:
-
Health-Related Quality of Life
- ICC:
-
Intraclass correlation coefficient
- OHRQoL:
-
Oral Health-Related Quality of Life
- PedsQL™4.0:
-
Pediatric Quality of life Generic Core scale
References
Aldrigui JM, Jabbar NS, Bonecker M, Braga MM, Wanderley MT. Trends and associated factors in prevalence of dental trauma in Latin America and Caribbean: a systematic review and meta-analysis. Community Dent Oral Epidemiol. 2014;42:30–42.
Do LG. Distribution of caries in children: variations between and within populations. J Dent Res. 2012;91:536–43.
Kassebaum NJS, Smith AGC, Bernabé E, Fleming TD, Reynolds AE, Vos T, Murray CJL, Marcenes W, GBD 2015 Oral Health Collaborators. Global, regional, and National Prevalence, incidence, and disability-adjusted life years for Oral conditions for 195 countries, 1990–2015: a systematic analysis for the global burden of diseases, injuries, and risk factors. J Dent Res. 2017;96:380–7.
Abanto J, Carvalho TS, Mendes FM, Wanderley MT, Bonecker M, Raggio DP. Impact of oral diseases and disorders on oral health-related quality of life of preschool children. Community Dent Oral Epidemiol. 2011;39:105–14.
Antonarakis GS, Patel RN, Tompson B. Oral health-related quality of life in non-syndromic cleft lip and/or palate patients: a systematic review. Community Dent Health. 2013;30:189–95.
Kragt L, Dhamo B, Wolvius EB, Ongkosuwito EM. The impact of malocclusions on oral health-related quality of life in children-a systematic review and meta-analysis. Clin Oral Investig. 2016;20:1881–94.
Zaror C, Martinez-Zapata MJ, Abarca J, Diaz J, Pardo Y, Pont A, Ferrer M. Impact of traumatic dental injuries on quality of life in preschoolers and schoolchildren: a systematic review and meta-analysis. Community Dent Oral Epidemiol. 2017;46:88–101.
Zhou Y, Wang Y, Wang X, Voliere G, Hu R. The impact of orthodontic treatment on the quality of life a systematic review. BMC Oral Health. 2014;14:66.
Espinoza-Espinoza G, Muñoz-Millán P, Vergara-González C, Atala-Acevedo C, Zaror C. Prevalence of early childhood caries in rural non-fluoridated areas of Chile. J Oral Res. 2016;5:307–13.
Hoffmeister L, Moya P, Vidal C, Benadof D. Factors associated with early childhood caries in Chile. Gac Sanit. 2016;30:59–62.
Zaror C, Pineda P, Orellana JJ. Prevalencia de caries temprana de la infancia y sus factores asociados en Chilenos de 2 y 4 años. Int J of Odontostomatol. 2011;5:171–7.
Sischo L, Broder HL. Oral health-related quality of life: what, why, how, and future implications. J Dent Res. 2011;90:1264–70.
Allen PF. Assessment of oral health related quality of life. Health Qual Life Outcomes. 2003;1:40.
McGrath C, Broder H, Wilson-Genderson M. Assessing the impact of oral health on the life quality of children: implications for research and practice. Community Dent Oral Epidemiol. 2004;32:81–5.
Filstrup SL, Briskie D, da Fonseca M, Lawrence L, Wandera A, Inglehart MR. Early childhood caries and quality of life: child and parent perspectives. Pediatr Dent. 2003;25:431–40.
Pahel BT, Rozier RG, Slade GD. Parental perceptions of children's Oral health: the early childhood Oral Health impact scale (ECOHIS). Health Qual Life Outcomes. 2007;5:6.
Huntington NL, Spetter D, Jones JA, Rich SE, Garcia RI, Spiro A 3rd. Development and validation of a measure of pediatric oral health-related quality of life: the POQL. J public Health Dent. 2011;71:185–93.
Tsakos G, Blair YI, Yusuf H, Wright W, Watt RG, Macpherson LM. Developing a new self-reported scale of oral health outcomes for 5-year-old children (SOHO-5). Health Qual Life Outcomes. 2012;10:62.
Borum MK, Andreasen JO. Therapeutic and economic implications of traumatic dental injuries in Denmark: an estimate based on 7549 patients treated at a major trauma Centre. Int J Paediatr Dent. 2001;11:249–58.
Ribeiro GL, Gomes MC, de Lima KC, Martins CC, Paiva SM, Granville-Garcia AF. The potential financial impact of oral health problems in the families of preschool children. Cien Saude Colet. 2016;21:1217–26.
Peker K, Uysal O, Bermek G. Cross - cultural adaptation and preliminary validation of the Turkish version of the early childhood oral health impact scale among 5-6-year-old children. Health Qual Life Outcomes. 2011;9:118.
Scarpelli AC, Oliveira BH, Tesch FC, Leao AT, Pordeus IA, Paiva SM. Psychometric properties of the Brazilian version of the early childhood Oral Health impact scale (B-ECOHIS). BMC Oral Health. 2011;11:19.
Hashim AN, Yusof ZY, Esa R. The Malay version of the early childhood Oral Health impact scale (Malay-ECOHIS)--assessing validity and reliability. Health Qual Life Outcomes. 2015;13:190.
Li S, Veronneau J, Allison PJ. Validation of a French language version of the early childhood Oral Health impact scale (ECOHIS). Health Qual Life Outcomes. 2008;6:9.
Abanto J, Paiva SM, Sheiham A, Tsakos G, Mendes FM, Cordeschi T, Vidigal EA, Bonecker M. Changes in preschool children's OHRQoL after treatment of dental caries: responsiveness of the B-ECOHIS. Int J Paediatr Dent. 2016;26:259–65.
Arrow P. Responsiveness and sensitivity of the early childhood Oral Health impact scale to primary dental care for early childhood caries. Community Dent Oral Epidemiol. 2016;44:1–10.
Jabarifar SE, Golkari A, Ijadi MH, Jafarzadeh M, Khadem P. Validation of a Farsi version of the early childhood oral health impact scale (F-ECOHIS). BMC Oral Health. 2010;10:4.
Jankauskiene B, Narbutaite J, Kubilius R, Gleiznys A. Adaptation and validation of the early childhood oral health impact scale in Lithuania. Stomatologija. 2012;14:108–13.
Lee GH, McGrath C, Yiu CK, King NM. Translation and validation of a Chinese language version of the early childhood Oral Health impact scale (ECOHIS). Int J Paediatr Dent. 2009;19:399–405.
Hadžipašić-Nazdrajić NA. Translation and validation of the instrument for the oral health-related quality of life assessment in 3 to 5 years old children in Bosnia-Herzegovina. J Health Sci. 2012;2:201–2016.
Pani SC, Badea L, Mirza S, Elbaage N. Differences in perceptions of early childhood oral health-related quality of life between fathers and mothers in Saudi Arabia. Int J Paediatr Dent. 2012;22:244–9.
Bordoni N, Ciaravino O, Zambrano O, Villena R, Beltran-Aguilar E, Squassi A. Early childhood Oral Health impact scale (ECOHIS). Translation and validation in Spanish language. Acta Odontol Latinoam. 2012;25:270–8.
Sperber AD. Translation and validation of study instruments for cross-cultural research. Gastroenterology. 2004;126:S124–8.
Abanto J, Albites U, Bönecker M, Martins-Paiva S, Castillo JL, Aguilar-Gálvez D. Cross-cultural adaptation and psychometric properties of the child perceptions questionnaire 11-14 (CPQ11-14) for the Peruvian Spanish language. Med Oral Patol Oral Cir Bucal. 2013;18:e832–8.
Núñez L, Rey R, Bravo-Cavicchioli D, Jiménez P, Fernández C, Adaptation MG. Validation of the Spanish version of child perception questionnaire CPQ-Spn11-14 in a Chilean community population. Rev Esp Salud Publica. 2015;89:585–95.
Varni J. The PedsQL™ measurement model for the Peadiatric quality of life inventory™. 2018. http://www.pedsql.org/PedsQL-Translation-Tables.pdf. Accessed 8 Aug 2018.
Maneesriwongul W, Dixon JK. Instrument translation process: a methods review. J Adv Nurs. 2004;48:175–86.
Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol. 1993;46:1417–32.
Wild D, Grove A, Martin M, Eremenco S, McElroy S, Verjee-Lorenz A, Erikson P, ITFf T, Cultural A. Principles of good practice for the translation and Cultural Adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and Cultural Adaptation. Value Health. 2005;8:94–104.
World Health Organization. Oral Health surveys: basic methods. 5th ed. Geneve: World Health Organization; 1997.
Andreasen J, Andreasen F. Classification, etiology adn epidemiology. Texbook and color atlas of traumatic injuries to the teeht. 3rd ed. Copenhagen: Munksgaard; 1994.
Streiner D, Kottner J. Recommendations for reporting the results of studies of instrument and scale development and testing. J Adv Nurs. 2014;70:1970–9.
Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL, Dekker J, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60:34–42.
Anthoine E, Moret L, Regnault A, Sébille V, Hardouin JB. Sample size used to validate a scale: a review of publications on newly-developed patient reported outcomes measures. Health Qual of Life Outcomes. 2014;12:176.
Muthén LK, Muthén BO. Mplus User’s Guide. Eighth Edition. Los Angeles: Muthén & Muthén. 2017. https://www.statmodel.com/download/usersguide/MplusUserGuideVer_8.pdf. Accessed 15 July 2018.
Kazis LE, Anderson JJ, Meenan RF. Effect sizes for interpreting changes in health status. Med Care. 1989;27:S178–89.
Franzblau A. Correlation coefficients. In: A primer of statisitics for non-statisticians. New York: Harcourt; 1958.
Malter S, Hirsch C, Reissmann DR, Schierz O, Bekes K. Effects of method of administration on oral health-related quality of life assessment using the child perceptions questionnaire (CPQ-G11-14). Clin Oral Investig. 2015;19:1939–45.
Desai R, Durham J, Wassell RW, Preshaw PM. Does the mode of administration of the Oral Health impact Profile-49 affect the outcome score? J Dent. 2014;42:84–9.
Tsakos G, Bernabé E, O'Brien K, Sheiham A, de Oliveira C. Comparison of the self-administered and interviewer-administered modes of the child-OIDP. Health Qual Life Outcomes. 2008;6:40.
Barbosa TS, Gaviao MB. Oral health-related quality of life in children: part III. Is there agreement between parents in rating their children’s oral health-related quality of life? A systematic review. Int J Dent Hyg. 2008;6:108–13.
Theunissen NCM, Vogels TGC, Koopman HM, Verrips GH, Zwinderman KA, Verloove-Vanhorick SP, et al. The proxy problem: child report versus parent report in health-related quality of life research. Qual Life Res. 1998;7:387–97.
Reissmann DR, John MT, Sagheri D, Sierwald I. Diagnostic accuracy of parents’ ratings of their child’s oral health-related quality of life. Qual Life Res. 2016;26:881–91.
Eiser C, Mohay H, Morse R. The measurement of quality of life in young children. Child Care Health Dev. 2000;26:401–13.
Jokovic A, Locker D, Stephens M, Kenny D, Tompson B, Guyatt G. Measuring parental perceptions of child oral health-related quality of life. J Public Health Dent. 2003;63:67–72.
Cronbach L. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16:297–334.
Martins-Júnior PA, Ramos-Jorge J, Paiva SM, Marques LS, Ramos-Jorge ML. Validations of the Brazilian version of the early childhood Oral Health impact scale (ECOHIS). Cad Saude Publica. 2012;28:367–74.
Sanjuàs C, Alonso J, Sanchís J, Casan P, Broquetas JM, Ferrie PJ, et al. The quality-of-life questionnaire with asthma patients: the Spanish version of the asthma quality of life questionnaire. Arch Bronconeumol. 1995;31:219–26.
Alonso J, Prieto L, Anto JM. La versión española del SF-36 Health Survey (Cuestionario de Salud SF-36): un instrumento para la medida de los resultados clínicos. Med Clin (Barc). 1995;104:771–6.
Bönecker M, Abanto J, Tello G, Oliveira LB. Impact of dental caries on preschool children's quality of life: an update. Braz Oral Res. 2012;26(Suppl 1):103–7.
Gomes MC, Pinto-Sarmento TC, Costa EM, Martins CC, Granville-Garcia AF, Paiva SM. Impact of oral health conditions on the quality of life of preschool children and their families: a cross-sectional study. Health Qual Life Outcomes. 2014;12:55.
Correa-Faria P, Paixao-Goncalves S, Paiva SM, Martins-Junior PA, Vieira-Andrade RG, Marques LS, Ramos-Jorge ML. Dental caries, but not malocclusion or developmental defects, negatively impacts preschoolers' quality of life. Int J Paediatr Dent. 2016;26:211–9.
Lee GH, McGrath C, Yiu CK, King NM. A comparison of a generic and oral health-specific measure in assessing the impact of early childhood caries on quality of life. Community Dent Oral Epidemiol. 2010;38:333–9.
Guyatt GH, Bombardier C, Tugwell PX. Measuring disease-specific quality of life in clinical trials. CMAJ. 1986;134:889–95.
Yilmaz F, Dogu B, Sahin F, Sirzai H, Kuran B. Investigation of responsiveness indices of generic and specific measures of health related quality of life in patients with osteoporosis. J Back Musculoskelet Rehabil. 2014;27:391–7.
Acknowledgements
The authors are especially grateful to Bhavna Pahel for providing the original ECOHIS questionnaire. We also thank the MAPI Research Trust and the author of PedsQL™4.0, Dr. J. W. Varni, for providing us with the copyright permission.
Carlos Zaror is a PhD candidate in Methodology of Biomedical Research and Public Health program, Universitat Autònoma de Barcelona, Barcelona, Spain.
Mª José Martínez is funded by a Miguel Servet research contract from the Instituto de Salud Carlos III and European Social Fund (CP15/00116).
Montse Ferrer is partially funded by the Departament d’Innovació, Universitats i Empresa, Generalitat de Catalunya (2014 SGR 748).
We would like to acknowledge Aurea Martin for her help in the English proofreading and editing process and in the figures edition of this manuscript.
Funding
This project was funded by a grant from the Convenio de Desempeño Regional, FRO 1301, Universidad de La Frontera N° UNT15–0012, and from DIUE of Generalitat de Catalunya (2017 SGR 452).
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Author information
Authors and Affiliations
Contributions
All authors have actively participated in the study and have made a substantial contribution to (1) either conception and design, or acquisition of data, or analysis and interpretation of data; as well as (2) the drafting of the article or its critical revision for important intellectual content; and (3) to the final approval of the version to be published. Each author believes that the manuscript represents honest work.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of the Universidad de La Frontera, Temuco, Chile with resolution number 061/2015. Informed consent from all parents and verbal assent from children was obtained to consider their participation in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Zaror, C., Atala-Acevedo, C., Espinoza-Espinoza, G. et al. Cross-cultural adaptation and psychometric evaluation of the early childhood oral health impact scale (ECOHIS) in chilean population. Health Qual Life Outcomes 16, 232 (2018). https://doi.org/10.1186/s12955-018-1057-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12955-018-1057-x