
Abstract
Severe asthma (SA) is a clinically and etiologically heterogeneous respiratory disease which affects among 5–10 % of asthmatic patients. Despite high-dose therapy, a large patients percentage is not fully controlled and has a poor quality of life. In this review, we describe the biomarkers actually known in scientific literature and used in clinical practice for SA assessment and management: neutrophils, eosinophils, periostin, fractional exhaled nitric oxide, exhaled breath condensate and galectins. Moreover, we give an overview on clinical and biological features characterizing severe asthma, paying special attention to the potential use of these ones as reliable markers. We finally underline the need to define different biomarkers panels to select patients affected by severe asthma for specific and personalized therapeutic approach.
Similar content being viewed by others


Background
Severe asthma (SA) is defined as ‘asthma which requires treatment with high dose inhaled corticosteroids (ICS) plus a second controller (and/or systemic corticosteroids) to prevent it from becoming ‘uncontrolled’ or which remains ‘uncontrolled’ despite this therapy’. This is the European Respiratory Society (ERS)/American Thoracic Society (ATS) definition, utilized across developed countries with general access to inhaled corticosteroid therapy [1, 2]. It is recognized that up to 50 % of patients are not well controlled and 5–10 % of patients suffer from a particularly severe disease that is often refractory to usual treatment [3, 4].
Evidence of any one of the four criteria below, while on current high-dose therapy, identifies the patient as having ‘‘severe asthma’’:
-
1.
Poor symptoms control.
-
2.
Frequent severe exacerbations, defined as two or more bursts of systemic corticosteroids in the previous year.
-
3.
Serious exacerbations, defined as at least one hospitalization, intensive care unit stay or mechanical ventilation in the previous year.
-
4.
Airflow limitation, i.e. forced expiratory volume in 1 s (FEV1), 80 % predicted (in the presence of reduced FEV1/forced vital capacity (FVC) defined as less than the lower limit of normal) following a withhold of both short- and long-acting bronchodilators.
Asthma, and severe asthma in particular, are increasingly considered as heterogeneous diseases, which may respond similarly to therapies. Recently, studies are beginning to identify different phenotypes defined by characteristic clinical manifestations, pathophysiological mechanisms and biomarkers [5].
The first studies performed in asthmatics distinguished subtypes based on inflammatory patterns obtained from bronchoalveolar lavage and endobronchial biopsies. Identifying patients with corticosteroid-naive, mild asthma who exhibited a T-helper (Th)2/Type 2 molecular signature in their epithelial cells, Woodruff et al., began the concept of molecular phenotyping, in which molecular pathways are linked to clinical and physiological characteristics [6].
A more detailed immunopathobiological picture of human SA is therefore emerging as the context of the heterogeneity of the disease, in relation to both inflammation and structural changes [7].
The identification of asthma phenotypes has given a boost to the search for biomarkers to help classifying patients, targeting therapies and predicting different pathological evolution mechanisms of the disease with strong benefits for the affected patients [8].
An ideal biomarker is easy to collect and measure, not invasive nor expensive, and can be used to identify either clinical or treatment response phenotypes, evaluate changes in disease activity, or confirm a diagnosis. This prospect provides the impetus for the research for reliable markers in SA, which are actually under intense study and are hereunder analyzed. In this review we focus the importance and the role of different known and potential biomarkers useful to define the physiopathological and clinical profiles of patients affected by severe asthma.
Neutrophils
Severe asthma is often characterized by neutrophilic inflammation, both in the presence or absence of Th2-induced eosinophilic inflammation [9, 10]. However, the functional role of these cells in disease progression remains unclear. Sputum neutrophil percentages are highly reproducible in patients with moderate to severe asthma, and can be used to assess novel anti-inflammatory therapies: targeting neutrophils has been suggested as a therapeutic option for these patients [11, 12].
Neutrophils recruitment can be mediated by Th17 cells, which are thought to have a role in asthma pathogenesis, especially in patients who do not respond to glucocorticoid therapy and show a decreased improvement in FEV1 and airway hyperresponsiveness (AHR) following treatment [13, 14]. Moreover, it has been demonstrated that, in addition to the specific antigenic components, pollens contain several intrinsic factors able to promote innate immune responses; among them, nicotinamide adenine dinucleotide phosphate oxidase (NADPH) induces the generation of reactive oxygen species (ROS) [15]. This oxidative insult induces an early wave of neutrophil recruitment in the airways and increases significantly ROS-generating activity of these cells [16]. It has been also evidenced that pollen can induce CXCL chemokine synthesis and that neutrophils can be recruited into the airways in a CXCR2-dependent manner [17].
The receptor for advanced glycation end-products (RAGE) is a pattern recognition receptor involved in the response to injury, infection and inflammation. Perturbations in the RAGE and its soluble forms (sRAGE) balance might be linked to neutrophilic airway inflammation in chronic airways disease [18]. A recent work from Sukkar et al. demonstrated a deficiency in lung and systemic sRAGE, in asthmatic and chronic obstructive pulmonary disease (COPD) patients with neutrophilic airway inflammation. sRAGE might be degraded by neutrophil-derived proteolytic enzymes in subjects with airway neutrophilia and might be identified as a potential biomarker for prognosis or patient management [19].
The metalloproteinase domain 8 (ADAM8) seems also to be involved in facilitating neutrophils migration into tissues [20]. It is highly expressed in bronchial biopsies from moderate and severe asthmatics and its recruitment of both eosinophils and neutrophils into airways tissue suggests a significant role in the pathogenesis of asthma [21–24].
Future therapeutic targets directed at the above mentioned proteins might significantly attenuate asthma symptoms by reducing inflammatory cells, primarily neutrophils, and having few adverse physiological consequences.
Eosinophils
Asthma is also histologically characterized by recruitment of eosinophils into the large airway wall and lumen, along with mucus plugging and epithelium denudation. Being associated with increased transforming growth factor β (TGF-β) expression and reticular basement membrane (RBM) thickness, the amount of these cells might be congruent with symptoms severity, worsened lung function, and near-fatal events [25–27].
The identification of eosinophilic inflammation is of a certain importance due to the severity of attacks which occur to these patients and to the existence of drugs, such as prednisolone, omalizumab and new biological agents, particularly active on this pattern [28].
It is known that Type-2 inflammatory pathways are involved in asthma, and many studies suggest that about 50 % of SA patients present Type-2 inflammation, as measured by eosinophilia or high levels of fractional exhaled nitric oxide (FeNO) [29, 30]. Miranda et al. distinguished early-onset severe asthma patients, characterized by allergen sensitivity, allergic symptoms, eosinophilia and higher serum immunoglobulin E (IgE) levels, and late-onset severe asthma subjects, with lower lung function than early-onset ones, despite a shorter duration of illness and significantly more symptoms if presenting persistent eosinophils at onset [27].
The need to block IgE binding to inflammatory cells and the consequent mediators release cascade concurred to the development of the unique monoclonal antibody approved for patients with severe allergic asthma: omalizumab, a recombinant humanized murine antibody against IgE antibodies. A recent study from our group investigated the effect of long-term anti-IgE treatment on the thickening of the RBM and eosinophil infiltration in bronchial biopsies from patients with severe persistent allergic asthma. Our results showed that a substantial proportion of severe asthmatics reduced the original bronchial RBM thickness and eosinophil infiltration after one-year treatment with anti-IgE, thus emphasizing the possible role of omalizumab in affecting airway remodeling in severe persistent allergic asthma [31]. Up to now, many studies have shown how the anti-IgE treatment in SA patients was effective in modulating airways remodeling and inflammation, as well as in improving lung functions and quality of life (Table 1).
Eosinophils count in induced sputum has long been the method of choice to evaluate eosinophilic lung inflammation and seems to be a reliable biomarker of airway inflammation as well as useful in adjusting corticosteroid treatments in asthma [38–40].
Newby et al. and McGrath et al. by using sputum, identified phenotypes of SA enriched for eosinophilic airway inflammation that might respond to therapies directed toward Th2 immune pathways [41, 42].
Recently, the dose ranging efficacy and safety with mepolizumab (DREAM) study correlated blood eosinophils levels, but not sputum eosinophilia, with response to mepolizumab [43]. These data are supported by many authors who evidenced that sputum eosinophils can not predict treatment response and that increased blood eosinophils are associated with higher risk for exacerbations, maybe owing to interleukin (IL)-5 levels [44, 45]. Following anti-IgE treatment, some studies found decreased blood eosinophils counts [46]. In the EXTRA study, Hanania and colleagues demonstrated that omalizumab efficacy was strongly related to the presence of airways eosinophilic inflammation and more accurately predicted by FeNO and serum periostin rather than IgE levels [47].
It is currently hypothesized that the use of blood eosinophils as biomarkers could help to personalize asthma management in patients with severe allergic asthma.
Active eosinophils recruitment is predominantly exerted by proteins secreted by epithelia, the most potent chemoattractant for these cells being eotaxin-1 (CCL11), that account for 80 % of TGF-ß expression in asthma [48–50]. A recent work evaluated CCL11 levels in bronchoalveolar lavage fluid (BALF), exhaled breath condensate (EBC), blood and sputum and evidenced a correlation between this protein in induced sputum and asthma severity [51].
It has also been hypothesized that asthma severity might be linked to a relationship between TGF-ß expression and the presence of submucosal eosinophils. It was evidenced that in bronchial biopsies the majority of eosinophils is TGF-ß1-mRNA positive [25, 52], with a higher extent in SA. Moreover, TGF-ß2 isoforms are expressed by eosinophils in severe allergic asthma where this cytokine promotes fibrotic responses and regulates mucin production [53, 54].
Although still in study and source of debate, the persistent eosinophilic phenotype in adults might be a real candidate for specific therapies thus potentially interfering with the natural history of SA with high exacerbation rates.
Fractional exhaled nitric oxide
Epithelial inducible nitric oxide synthase (NOS) has been shown to be the main determinant of FeNO levels in the respiratory tract [55] due to increased nitric oxide (NO) production by activated bronchial epithelial cells in response to pro-inflammatory stimuli [56]. It is postulated that the decrease in FeNO values seen after steroid treatment might be due to an inhibitory effect of these drugs on inducible NOS activity [55], therefore the measurement of NO concentration in exhaled breath has been standardized for clinical use. It is a quantitative, non-invasive, simple, and safe method to assess airway inflammation, to monitor responsiveness to ICS therapy in adults [57] and to predict asthma control status in childhood [58]. Recently, a retrospective study was performed on 416 asthmatic patients on combined therapy (long-acting β2 agonist and ICS). The authors assessed the correlation between FEV1 and FeNO to ascertain the correct use of FeNO measurement in different asthma phenotypes with regard to disease control, severity, allergy, comorbidity, obesity, age and smoking status. No correlation was found between FeNO levels and asthma severity but it was shown a link to other parameters such as age, gender, history of emergency room visits and atopy [59]. Moreover, cross-sectional study on 100 adult asthmatic patients showed that FeNO levels were correlated primary with asthma control rather than asthma severity, confirming FeNO as reliable biomarker in asthma management [60]. Peirsman et al. performed a randomized controlled trial on 99 children with persistent allergic asthma: patients outcomes were evaluated over a 52-week timeframe and, only in FeNO group, therapeutic approach was guided by FeNO measurements. Results demonstrated that FeNO evaluation diminished asthma exacerbations rate in associated with an increased leukotriene receptor antagonist use and ICS doses administration [61]. FeNO may also be used as predictor of omalizumab treatment efficacy. Hanania et al. evaluated FeNO, serum periostin and blood eosinophilia as potential biomarkers useful to evaluate effectiveness of anti-IgE treatment on 850 adult persistent SA patients. After 48 weeks of therapy, reduction of exacerbations rate was greater in high versus low subgroup for FeNO levels (53 vs 16 %) [47]. In the Inner-City Anti-IgE therapy of asthma trial, Busse et al. confirmed a clinical benefit from omalizumab treatment in children and adolescents [62]. In a post hoc analysis of the previous study, Sorkeness et al. found that FeNO, together with blood eosinophils and body mass index, can predict omalizumab response [63]. Moreover, preliminary data indicated that elevated FeNO may be indicative of anti-IL-13/IL-4 biological response [64]. However, Haldar et al. showed that FeNO seems to be less closely associated with a response to mepolizumab (anti IL-5) than blood eosinophils count [65].
In SA, the bronchial mucosa is markedly hyperplastic, the epithelium may be susceptible to destruction, flaking and detachment from the RBM. Therefore, FeNO levels can be under-representative [66]. The ERS/ATS Task Force has published a detailed guideline on definition, evaluation and treatment of SA. The Authors defined SA phenotypes giving specific recommendations for the use of diagnostic tools like measurement of FeNO to guide therapy. Elevated FeNO value is considered as a marker of Th2 inflammation and atopy but not an effective biomarker useful in SA management [1].
Exhaled breath condensate
Exhaled breath (EB) is mainly composed by aerosolized, non-volatile particles of airway lining fluid collected from the airways by airflow turbulence, water vapor condensation, inorganic (O2, N2), and organic (CO2) atmospheric volatile water-soluble gases, endogenous and exogenous volatile organic compounds [67]. EBC is the EB that has been condensed, typically by using a commercially available refrigerating device, according to ATS/ERS Guidelines [68]. It is used to investigate the composition of airway fluids and to achieve information about pulmonary alveoli, inflammation, nitrosative and oxidative stress in airways diseases such as COPD [69], asthma [70] and lung cancer [67]. Concerning SA, clinical studies identified chemical and biological characteristics that distinguish EBC of severe asthmatics from those obtained from healthy subjects and mild to moderate asthmatic patients (Fig. 1). Experimental data on EBC pH in SA are contrasting and there are still few studies about it [71, 72]. Eicosanoids as pro-inflammatory Leukotriene B4 (LTB4) and anti-inflammatory Lipoxin A4 (LXA4) are increased in asthmatics versus healthy subjects and LXA4/LTB4 ratio dramatically decreases in EBC in correlation with asthma severity [73]. Eotaxin-1 was evaluated in blood, EBC, sputum and BALF and was proposed as a tool for assessment of asthma severity [51]. High levels of nitrogen reactive species (NO, NO2−, NO3−) and endogenous ROS (superoxide, hydrogen peroxide, hydroxyl radical) provided evidence for pathologic oxidizing processes in asthma and are indicative of airways oxidative and nitrosative stress [74]. In SA, these pathologic features are exacerbated and correlated to asthma stability and corticosteroid therapy response [75]. Many studies have been published on the use of omics techniques in asthmatic children for the analysis of easy to be collected samples. Using liquid chromatography and mass spectrometry, significant differences useful to distinguish asthma severity between healthy and asthmatic children biochemical profiles were found in urine and in EBC [76–78]. Baraldi et al. proposed the use of metabolomic analysis or breathomic approach of EBC to characterize asthma phenotypes and personalize the therapeutic plan [79]. Fitzpatrick et al. found that SA children showed metabolic differences associated with oxidative stress-related pathways which may contribute to their corticosteroids refractory state [80]. General recommendations for EBC collection and exhaled biomarkers measurements are available in order to avoid a possible alteration in biomarker concentrations. Despite EBC collection remains a procedure potentially influenced by numerous endogenous and exogenous factors, in present and in future, EBC analysis can turn out as a promising, safe and non-invasive method for monitoring SA patients [68].

Changes in exhaled breath condensate mediators values in severe asthma.
Periostin
Periostin is a secreted matricellular protein with a key role in amplification and in persistence of chronic inflammation of allergic diseases [81]. Having the ability to bind fibronectin, tenascin-C, collagen I, III and V, periostin is involved in the process of subepithelial fibrosis in asthma patients [82]. Furthermore, it exerts its biological activity also by binding integrins on cell surfaces and activating intracellular signal pathways [83]. Periostin is induced by IL-4 and IL-13 in bronchial epithelial cells and in lung fibroblasts and its expression is correlated with the RBM thickness [82, 84, 85]. Moreover, this molecule is able to accelerate eosinophils tissue infiltration facilitating their adhesion to extracellular matrix proteins [86]. Serum periostin can be considered a systemic biomarker Th2-high asthma related because it is a signature molecule associated to higher AHR, serum IgE, eosinophilic inflammation, subepithelial fibrosis, compared to Th2-low asthma. It is possible to consider serum periostin a promising biomarker for two main reasons. First of all, this protein easily moves from inflamed tissues to blood circulation so its serum concentrations reflects its local production in lesions induced by Th2-type immune responses [87, 88]. Moreover, its basal serum levels are physiologically relatively low (~50 ng/ml) compared to other extracellular matrix proteins such as fibronectin or vitronectin. Jia et al. in the Bronchoscopic Exploratory Research Study of Biomarkers in Corticosteroid-refractory Asthma (BOBCAT), identified serum periostin as the single best systemic biomarker of airway luminal and tissue eosinophilia in severe, uncontrolled asthmatics. Adopting 25 ng/ml serum periostin as an arbitrary cut-off, eosinophil-low and eosinophil-high patients are effectively differentiated, with a positive predicted value of 93 %. This study evidenced the superiority of serum periostin for predicting sputum and tissue eosinophilia, compared to blood eosinophils, IgE levels, YKL-40 and FeNO [89]. More recently, Kanemitsu et al., in an observational study, found that high serum periostin concentration (≥95 ng/ml) is the unique biomarker, among several serum markers, associated with the greater annual decline in FEV1 (at least 30 ml/year) [90]. In addition to being an encouraging biomarker in predicting responders to traditional ICS therapy, periostin seems to also identify responders to new target treatments [91]. Corren et al. demonstrated that its higher serum levels might predict the response to Th2 target therapy with biologic agents such as anti-IL-13 monoclonal antibody (lebrikizumab). The Authors performed a randomized, double-blind, placebo-controlled study of lebrikizumab in 219 adults with unstable asthma despite ICS treatment. The therapy was associated with increased FEV1 values in patients with high pretreatment levels of serum periostin [92]. Similarly, analyzing the results from the EXTRA study performed with uncontrolled, severe, allergic asthmatics, Hanania et al. found that the high serum periostin group had a greater decreased exacerbation rate after omalizumab treatment compared to low serum periostin group [47]. Finally, in a recently published study, Bobolea et al. investigated the potential role of sputum periostin, more organ-targeted than serum periostin, as a biomarker of SA. The Authors found that sputum periostin levels are associated with persistent airflow limitation and eosinophilic inflammatory phenotype despite high-dose ICS therapy [93].
Taken together, these results show that periostin can be a useful biomarker to apply stratified medicine for SA and to yield better outcomes in asthma management. More evaluations are required to validate and clarify the potential utility of periostin in research and before this measurement can be applied in everyday clinical practice. Future studies should better evaluate this biomarker because it was demonstrated that its high levels could be detected in several conditions associated with increased cellular proliferation, angiogenesis, stress, tissues injury not necessarily dependent on a Th2 immune response, as shown in Table 2. We should also remember that periostin is not specific to asthma or the airway epithelium [81, 109, 123, 124]. These considerations should lead clinicians to use an integrative approach which links clinical features and molecular mechanisms and should encourage to better investigate analysis of sputum periostin. It will also be necessary to establish and validate cut-off values to define high and low periostin levels. Furthermore, additional carefully designed studies are needed to evaluate if periostin, alone or in combination with other more conventional biomarkers, can be utilized in better redefining current asthma phenotypes and selecting patients for emerging asthma therapeutics targeting Th2 inflammation.
Galectins
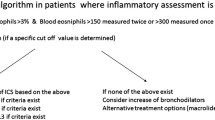
Galectins are a family of animal lectins with different cellular and extracellular localizations. These proteins bind the cell-surface and extracellular matrix (ECM) glycans and, thereby, affect a variety of cellular processes and biological activities. To date, 15 galectins having a role in physiological and pathobiological processes like cancer, heart failure, tissue repair and platelets aggregation have been found in mammals [125–128]. Regarding airway diseases, the effects of these proteins on the inflammatory process were analyzed for the first time in murine models. Galectin-9 role is still unclear because it was identified as a possible recruiter of eosinophil granulocytes and promoter of Th2 dominance [129], but also as a IgE binding protein with anti-allergic effects able to prevent acute asthma exacerbations [130, 131]. Another galectin with a demonstrated role in asthma is Galectin-3, the only chimera galectin found in Vertebrates, with biological activities in numerous cellular functions like cellular adhesion, growth, chemoattraction, differentiation, apoptosis and cellular cycle as well as an IgE binding protein activity [132–134]. Evaluation of Galectin-3 expression in deficient and wild-type gal-3 mice with OVA-induced asthma, evidenced that OVA-sensitized gal-3 (−/−) mice developed fewer eosinophils, lower goblet cell metaplasia and significantly less AHR after airway OVA challenge compared to similarly treated gal-3 (+/+) mice [135]. Moreover, studies on Gal-3 gene therapy confirmed how it is possible to reduce eosinophils airway infiltration, AHR and tissue remodeling [136]. The involvement of Galectin-3 in human airways inflammatory process has been ascertained for COPD [137], lung fibrosis [138] and asthma. In asthma, Gal-3 expression seems to be related to the development of a specific inflammatory pattern and biological therapy outcome. Recently, Gao et al. found a significantly reduced sputum Gal-3 in patients with neutrophilic asthma [139]. Moreover, evaluating bronchial biopsies of SA patients treated with omalizumab using proteomic technique, we observed that proteomic profile of bronchial tissue before omalizumab treatment presents a typical pattern indicative of anti-IgE treatment response. Galectin-3 was expressed only in subjects with a positive bronchial morphometric analysis response to anti-IgE treatment. In our opinion Galectin-3, having the ability to bind IgE proteins, can be considered a reliable biomarker to predict the modulation of airway remodeling and the improvement of pulmonary function in SA patients before they begin omalizumab therapy (Fig. 2) [37].

Possible clinical meaning of Galectin 3 in severe asthma.
Conclusions
The need in finding biomarkers useful to monitor treatment response is evident in clinical practice, however their discovery is made difficulty by the huge number of proteins involved in severe asthma pathogenesis, only a part of which has been cited in this work. Recently, advances have been obtained by data analysis from genomic and proteomic profiling studies but the application of these methods in clinical practice is difficult. One of the main problems is the cost of many techniques, which require specific instrumentation and skills not easy to achieve. Moreover, protein concentrations may change depending on the inflammatory condition of the patient, disease-associated processes and the sample collecting/analysis method. Nonetheless, each of candidate biomarkers is involved in different biological aspects and gives us information that can be largely overlapping. All these reasons make clear that the road to the identification and the daily use of defined biomarkers in SA is still long and winding. Development of novel serum/sputum-based biomarker panels with improved sensitivity and specificity over the ones currently available, will lead to promising future in the diagnosis of SA [140–142]. Accordingly with Gustafson et al., the more suitable reality in clinical practice will be: a definition of different panels composed by different biomarkers leading to the eligibility of the patients to a certain therapeutic treatment [143].
Abbreviations
- SA:
-
severe asthma
- ICS:
-
inhaled corticosteroids
- ERS:
-
European Respiratory Society
- ATS:
-
American Thoracic Society
- FEV1:
-
forced expiratory volume in 1 second
- FVC:
-
forced vital capacity
- Th:
-
T helper lymphocyte
- AHR:
-
airway hyperresponsiveness
- NADPH:
-
nicotinamide adenine dinucleotide phosphate oxidase
- ROS:
-
reactive oxygen species
- RAGE:
-
receptor for advanced glycation end-products
- sRAGE:
-
soluble form of receptor for advanced glycation end-products
- COPD:
-
chronic obstructive pulmonary disease
- ADAM8:
-
metalloproteinase domain 8
- TGF-β:
-
trasforming growth factor β
- RBM:
-
reticular basement membrane
- FeNO:
-
fractional exhaled nitric oxide
- IgE:
-
immunoglobulin E
- IL:
-
interleukin
- CCL11:
-
eotaxin-1
- BALF:
-
bronchoalveolar lavage fluid
- EBC:
-
exhaled breath condensate
- NOS:
-
nitric oxide synthase
- NO:
-
nitric oxide
- EB:
-
exhaled breath
- LTB4:
-
leukotriene B4
- LXA4:
-
lipoxin A4
- ECM:
-
extracellular matrix
References
Chung KF, Wenzel SE, Brozek JL, Bush A, Castro M, Sterk PJ et al (2014) International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J 43:343–373
American Thoracic Society (2000) Proceedings of the ATS workshop on refractory asthma: current understanding, recommendations, and unanswered questions. Am J Respir Crit Care Med 162:2341–2351
Moore WC, Bleecker ER, Curran-Everett D, Erzurum SC, Ameredes BT, Bacharier L et al (2007) Characterization of the severe asthma phenotype by the National Heart, Lung, and Blood Institute’s Severe Asthma Research Program. J Allergy Clin Immunol 119:405–413
Chen H, Blanc PD, Hayden ML, Bleecker ER, Chawla A, Lee JH et al (2008) Assessing productivity loss and activity impairment in severe or difficult-to-treat asthma. Value Health 11:231–239
Wenzel SE (2012) Asthma phenotypes: the evolution from clinical to molecular approaches. Nat Med 18:716–725
Woodruff PG, Modrek B, Choy DF, Jia G, Abbas AR, Ellwanger A et al (2009) T-helper type 2-driven inflammation defines major subphenptypes of asthma. Am J Respir Crit Care Med 180:388–395
Trejo Bittar HE, Yousem SA, Wenzel SE (2015) Pathobiology of severe asthma. Ann Rev Pathol 10:511–545
Moore WC, Meyers DA, Wenzel SE, Teague WG, Li H, Li X et al (2010) Identification of asthma phenotypes using cluster analysis in the severe asthma research program. Am J Respir Crit Care Med 181:315–323
Jatakanon A, Uasuf C, Maziak W, Lim S, Chung KF, Barnes PJ (1999) Neutrophilic inflammation in severe persistent asthma. Am J Respir Crit Care Med 160:1532–1539
Gibson PG, Simpson JL, Saltos N (2001) Heterogeneity of airway inflammation in persistent asthma: evidence of neutrophilic inflammation and increased sputum interleukin-8. Chest 119:1329–1336
Rossall MRW, Cadden PA, Molphy SD, Plumb J, Singh D (2014) Repeatability of induced sputum measurements in moderate to severe asthma. Respir Med 108:1566–1568
Nair P, Gaga M, Zervas E, Alagha K, Hargreave FE, O’Byrne PM et al (2012) Safety and efficacy of a CXCR2 antagonist in patients with severe asthma and sputum neutrophils: a randomized, placebo-controlled clinical trial. Clin Exp Allergy 42:1097–1103
Schleimer RP (2004) Glucocorticoids suppress inflammation but spare innate immune responses in airway epithelium. Proc Am Thorac Soc 1:222–230
Barnes PJ, Adcock IM (2009) Glucocorticoid resistance in inflammatory diseases. Lancet 373:1905–1917
Hosoki K, Boldogh I, Sur S (2015) Innate responses to pollen allergens. Curr Opin Allergy Clin Immunol 15:79–88
Boldogh I, Bacsi A, Choudhury BK, Dharajiya N, Alam R, Hazra TK (2005) ROS generated by pollen NADPH oxidase provide a signal that augments antigen-induced allergic airway inflammation. J Clin Invest 115:2169–2179
Hosoki K, Aguilera-Aguirre L, Brasier AR, Kurosky A, Boldogh I, Sur S (2015) Pollen-induced innate recruitment of neutrophils facilitates induction of allergic sensitization and airway inflammation. Am J Respir Cell Mol Biol. doi:10.1165/rcmb.2015-0044OC
Sims GP, Rowe DC, Rietdijk ST, Herbst R, Coyle AJ (2010) HMGB1 and RAGE in inflammation and cancer. Ann Rev Immunol 28:367–388
Sukkar MB, Wood LG, Tooze M, Simpson JL, McDonald VM, Gibson PG et al (2012) Soluble RAGE is deficient in neutrophilic asthma and COPD. Eur Respir J 39:721–729
Gómez-Gaviro M, Domínguez-Luis M, Canchado J, Calafat J, Janssen H, Lara-Pezzi E et al (2007) Expression and regulation of the metalloproteinase ADAM-8 during human neutrophil pathophysiological activation and its catalytic activity on L-selectin shedding. J Immunol 178:8053–8063
Johansson MW, Lye MH, Barthel SR, Duffy AK, Annis DS, Mosher DF (2004) Eosinophils adhere to vascular cell adhesion molecule-1 via podosomes. Am J Respir Cell Mol Biol 31:413–422
Paulissen G, Rocks N, Quesada-Calvo F, Gosset P, Foidart JM, Noel A et al (2006) Expression of ADAMs and their inhibitors in sputum from patients with asthma. Mol Med 12:171–179
Foley SC, Mogas AK, Olivenstein R, Fiset PO, Chakir J, Bourbeau J et al (2007) Increased expression of ADAM-33 and ADAM-8 with disease progression in asthma. J Allergy Clin Immunol 119:863–871
Oreo KM, Gibson PG, Simpson JL, Wood LG, McDonald VM, Baines KJ (2013) Sputum ADAM-8 expression in increased in severe asthma and COPD. Clin Exp Allergy 44:342–352
Flood-Page P, Menzies-Gow A, Phipps S, Ying S, Wangoo A, Ludwig MS et al (2003) Anti-IL-5 treatment reduces deposition of ECM proteins in the bronchial subepithelial basement membrane of mild atopic asthmatics. J Clin Investig 112:1029–1036
Green RH, Brightling CE, Woltmann G, Parker D, Wardlaw AJ, Pavord ID (2002) Analysis of induced sputum in adults with asthma: identification of subgroup with isolated sputum neutrophilia and poor response to inhaled corticosteroids. Thorax 57:875–879
Miranda C, Busacker A, Balzar S, Trudeau J, Wenzel SE (2004) Distinguishing severe asthma phenotypes: role of age at onset and eosinophilic inflammation. J Allergy Clin Immunol 113:101–108
Hilvering B, Pavord ID (2015) What goes up must come down: biomarkers and novel biologicals in severe asthma. Clin Exp Allergy 45:1162–1169
Wenzel SE, Schwartz LB, Langmack EL, Halliday JL, Trudeau JB, Gibbs RL et al (1999) Evidence that severe asthma can be divided pathologically into two inflammatory subtypes with distinct physiologic and clinical characteristics. Am J Respir Crit Care Med 160:1001–1008
Dweik RA, Sorkness RL, Wenzel S, Hammel J, Curran-Everett D, Comhair SA et al (2010) Use of exhaled nitric oxide measurement to identify a reactive, at risk phenotype among patients with asthma. Am J Respir Crit Care Med 181:1033–1041
Riccio AM, Dal Negro RW, Micheletto C, De Ferrari L, Folli C, Chiappori A et al (2012) Omalizumab modulates bronchial reticular basement membrane thickness and eosinophil infiltration in severe persistent allergic asthma patients. Int J Immunopathol Pharmacol 25:475–484
Zietkowski Z, Skiepko R, Tomasiak-Lozowska MM, Bodzenta-Lukaszyk A (2010) Anti-IgE therapy with omalizumab decreases endothelin-1 in exhaled breath condensate of patients with severe persistent allergic asthma. Respiration 80:534–542
Zietkowski Z, Skiepko R, Tomasiak-Lozowska MM, Lenczewska D, Bodzenta-Lukaszyk A (2011) RANTES in exhaled breath condensate of patients with severe persistent allergic asthma during omalizumab therapy. Int Arch Allergy Immunol 154:25–32
Skiepko R, Ziętkowski Z, Lukaszyk M, Budny W, Skiepko U, Milewski R et al (2014) Changes in blood eosinophilia during omalizumab therapy as a predictor of asthma exacerbation. Postepy Dermatol Alergol 31:305–309
Tajiri T, Niimi A, Matsumoto H, Ito I, Oguma T, Otsuka K et al (2014) Comprehensive efficacy of omalizumab for severe refractory asthma: a time-series observational study. Ann Allergy Asthma Immunol 113(470–5):e2
Gouder C, West LM, Montefort S (2015) The real-life clinical effects of 52 weeks of omalizumab therapy for severe persistent allergic asthma. Int J Clin Pharm 37:36–43
Mauri P, Riccio AM, Rossi R, DiSilvestre D, Benazzi L, DeFerrari L et al (2014) Proteomics of bronchial biopsies: galectin-3 as a predictive biomarker of airway remodelling modulation in omalizumab-treated severe asthma patients. Immunol Lett 162(1 Pt A):2–10
Wadsworth S, Sin D, Dorscheid D (2011) Clinical update on the use of biomarkers of airway inflammation in the management of asthma. J Asthma Allergy 4:77–86
Eltboli O, Brightling CE (2013) Eosinophils as diagnostic tools in chronic lung disease. Expert Rev Respir Med 7:33–42
Szefler SJ, Wenzel S, Brown R, Erzurum SC, Fahy JV, Hamilton RG et al (2012) Asthma outcomes: biomarkers. J Allergy Clin Immunol 129(Suppl):9–23
Newby C, Agbetile J, Hargadon B, Monteiro W, Green R, Pavord I et al (2014) Lung function decline and variable airway inflammatory pattern: longitudinal analysis of severe asthma. J Allergy Clin Immunol 134:287–294
McGrath KW, Icitovic N, Boushey HA, Lazarus SC, Sutherland ER, Chinchilli VM et al (2012) A large subgroup of mild-to-moderate asthma is persistently noneosinophilic. Am J Respir Crit Care Med 185:612–619
Pavord ID, Korn S, Howarth P, Bleecker ER, Buhl R, Keene ON et al (2012) Mepolizumab for severe eosinophilic asthma (DREAM): a multicentre, double-blind, placebo-controlled trial. Lancet 380:651–659
Malinovschi A, Fonseca JA, Jacinto T, Alving K, Janson C (2013) Exhaled nitric oxide levels and blood eosinophil counts independently associate with wheeze and asthma events in National Health and Nutrition Examination Survey subjects. J Allergy Clin Immunol 132:821–827
Katz LE, Gleich GJ, Hartley BF, Yancey SW, Ortega HG (2014) Blood eosinophil count is a useful biomarker to identify patients with severe eosinophilic asthma. Ann Am Thorac Soc 11:531–536
Djukanović R, Wilson SJ, Kraft M, Jarjour NN, Steel M, Chung KF et al (2004) Effects of treatment with anti-immunoglobulin E antibody omalizumab on airway inflammation in allergic asthma. Am J Respir Crit Care Med 170:583–593
Hanania NA, Wenzel S, Rosen K, Hsieh HJ, Mosesova S, Choy DF et al (2013) Exploring the effects of Omalizumab in allergic asthma. An analysis of biomarkers in the EXTRA study. Am J Respir Crit Care Med 187:804–811
Conroy DM, Williams TJ (2001) Eotaxin and the attraction of eosinophils to the asthmatic lung. Respir Res 2:150–156
Zietowski Z, Tomasiek-Lozowska MM, Skiepko R, Zietowska E, Bodzenta-Lukaszyk A (2010) Eotaxin-1 in exhaled breath condensate of stable and unstable asthma patients. Respir Res 11:110
Kim CK, Kita H, Callaway Z, Kim HB, Choi J, Fujisawa T et al (2010) The roles of a Th2 cytokine and CC chemokine in children with stable asthma: potential implication in eosinophil degranulation. Pediatr Allergy Immunol 21:e697–e704
Wu D, Zhou J, Bi H, Li L, Gao W, Huang M et al (2014) CCL-11 as a potential diagnostic marker for asthma? J Asthma 51:847–854
Minshall EM, Leung DY, Martin RJ, Song LY, Cameron L, Ernst P et al (1997) Eosinophil-associated TGF-β1 mRNA expression and airways fibrosis in bronchial asthma. Am J Respir Cell Mol Biol 17:326–333
Harrop CA, Gore RB, Evans CM, Thornton DJ, Herrick SE (2013) TGF-ß2 decreases baseline and IL-13-stimulated mucin production by primary human bronchial epithelial cell. Exp Lung Res 39:39–47
Al-Alawi M, Hassan T, Chotirmall SH (2014) Transforming growth factor ß and severe asthma: a perfect storm. Respir Med 108:1409–1423
Lane C, Knight D, Burgess S, Franklin P, Horak F, Legg J et al (2004) Epithelial inducible nitric oxide synthase activity is the major determinant of nitric oxide concentration in exhaled breath. Thorax 59:757–760
Van Den Toorn LM, Overbeek SE, De Jongste JC, Leman K, Hoogsteden HC, Prins JB (2001) Airway inflammation is present during clinical remission of atopic asthma. Am J Respir Crit Care Med 164:2107–2113
Dweik RA, Boggs PB, Erzurum SC, Irvin CG, Leigh MW, Lundberg JO et al (2011) on behalf of the American Thoracic Society Committee on Interpretation of Exhaled Nitric Oxide Levels (FeNO) for Clinical Applications. An Official ATS Clinical Practice Guideline: Interpretation of Exhaled Nitric Oxide Levels (FENO) for Clinical Applications. Am J Respir Crit Care Med 184:602–615
Yang S, Park J, Lee YK, Kim H, Hahn YS (2015) Association of longitudinal fractional exhaled nitric oxide measurements with asthma control in atopic children. Respir Med 109:572–579
Gemicioglu B, Musellim B, Dogan I, Guven K (2014) Fractional exhaled nitric oxide (FeNo) in different asthma phenotypes. Allergy Rhinol 5:157–161
Sippel JM, Holden WE, Tilles SA, O’Hollaren M, Cook J, Thukkani N et al (2000) Exhaled nitric oxide levels correlate with measures of disease control in asthma. J Allergy Clin Immunol 106:645–650
Peirsman EJ, Carvelli TJ, Hage PY, Hanssens LS, Pattyn L, Raes MM et al (2014) Exhaled nitric oxide in childhood allergic asthma management: a randomised controlled trial. Pediatr Pulmonol 49:624–631
Busse WW, Morgan WJ, Gergen PJ, Mitchell HE, Gern JE, Liu AH et al (2011) Randomized trial of omalizumab (anti-IgE) for asthma in inner-city children. N Engl J Med 364:1005–1015
Sorkness CA, Wildfire JJ, Calatroni A, Mitchell HE, Busse WW, O’Connor GT et al (2013) Reassessment of omalizumab-dosing strategies and pharmacodynamics in inner-city children and adolescents. J Allergy Clin Immunol Pract 1:163–171
Wenzel S, Ford L, Pearlman D, Spector S, Sher L, Skobieranda F et al (2013) Dupilumab in persistent asthma with elevated eosinophil levels. N Engl J Med 368:2455–2466
Haldar P, Brightling CE, Hargadon B, Gupta S, Monteiro W, Sousa A et al (2009) Mepolizumab and exacerbations of refractory eosinophilic asthma. N Engl J Med 360:973–984
Hamid Q (2003) Gross pathology and hystopatology of asthma. J Allergy Clin Immunol 111:431–432
Dent AG, Sutedja TG, Zimmerman PV (2013) Exhaled breath analysis for lung cancer. J Thorac 5:540–550
Horváth I, Hunt J, Barnes PJ, Alving K, Antczak A, Baraldi E et al (2005) ATS/ERS Task Force on Exhaled Breath Condensate. Exhaled breath condensate: methodological recommendations and unresolved questions. Eur Respir J 26:523–548
Corhay JL, Moermans C, Henket M, Nguyen Dang D, Duysinx B, Louis R (2014) Increased of exhaled breath condensate neutrophil chemotaxis in acute exacerbation of COPD. Respir Res 15:115
Schwarz K, Biller H, Windt H, Koch W, Hohlfeld JM (2015) Characterization of exhaled particles from the human lungs in airway obstruction. J Aerosol Med Pulm Drug Deliv 28:52–58
Tseliou E, Bessa V, Hillas G, Delimpoura V, Papadaki G, Roussos C et al (2010) Exhaled nitric oxide and exhaled breath condensate pH in severe refractory asthma. Chest 138:107–113
Liu L, Teague WG, Erzurum S, Fitzpatrick A, Mantri S, Dweik RA et al (2011) National Heart, Lung, and Blood Institute Severe Asthma Research Program (SARP). Determinants of exhaled breath condensate pH in a large population with asthma. Chest 139:328–336
Kazani S, Planaguma A, Ono E, Bonini M, Zahid M, Marigowda G (2013) Exhaled breath condensate eicosanoid levels associate with asthma and its severity. J Allergy Clin Immunol 132:547–553
Comhair SA, Erzurum SC (2010) Redox control of asthma: molecular mechanisms and therapeutic opportunities. Antioxid Redox Signal 12:93–124
Tomasiak-Lozowska MM, Zietkowski Z, Przeslaw K, Tomasiak M, Skiepko R, Bodzenta-Lukaszyk A (2012) Inflammatory markers and acid-base equilibrium in exhaled breath condensate of stable and unstable asthma patients. Int Arch Allergy Immunol 159:121–129
Mattarucchi E, Baraldi E, Guillou C (2012) Metabolomics applied to urine samples in childhood asthma; differentiation between asthma phenotypes and identification of relevant metabolites. Biomed Chromatogr 26:89–94
Di Gangi IM, Pirillo P, Carraro S, Gucciardi A, Naturale M, Baraldi E et al (2012) Online trapping and enrichment ultra performance liquid chromatography-tandem mass spectrometry method for sensitive measurement of “arginine-asymmetric dimethylarginine cycle” biomarkers in human exhaled breath condensate. Anal Chim Acta 754:67–74
Carraro S, Giordano G, Reniero F, Carpi D, Stocchero M, Sterk PJ et al (2013) Asthma severity in childhood and metabolomic profiling of breath condensate. Allergy 68:110–117
Baraldi E, Carraro S, Giordano G, Reniero F, Perilongo G, Zacchello F (2009) Metabolomics: moving towards personalized medicine. Ital J Pediatr 35:30
Fitzpatrick AM, Park Y, Brown LA, Jones DP (2014) Children with severe asthma have unique oxidative stress-associated metabolomic profiles. J Allergy Clin Immunol 133:258–261
Conway SJ, Izuhara K, Kudo Y, Litvin J, Markwald R, Ouyang G et al (2014) The role of periostin in tissue remodeling across health and disease. Cell Mol Life Sci 71:1279–1288
Takayama G, Arima K, Kanaji T, Toda S, Tanaka H, Shoji S et al (2006) Periostin: a novel component of subepithelial fibrosis of bronchial asthma downstream of IL-4 and IL-13 signals. J Allergy Clin Immunol 118:98–104
Izuhara K, Arima K, Ohta S, Suzuki S, Inamitsu M, Yamamoto K (2014) Periostin in allergic inflammation. Allergol Int 63:143–151
Yuyama N, Davies DE, Akaiwa M, Matsui K, Hamasaki Y, Suminami Y et al (2002) Analysis of novel disease-related genes in bronchial asthma. Cytokine 19:287–296
Sidhu SS, Yuan S, Innes AL, Kerr S, Woodruff PG, Hou L et al (2010) Roles of epithelial cell-derived periostin in TFG-beta activation, collagen production, and collagen gel elasticity in asthma. Proc Natl Acad Sci USA 107:14170–14175
Blanchard C, Mingler MK, McBride M, Putnam PE, Collins MH, Chang G et al (2008) Periostin facilitated eosinophil tissue infiltration in allergic lung and esophageal responses. Mucosal Immunol 1:289–296
Masuoka M, Shiraishi H, Ohta S, Suzuki S, Arima K, Aoki S et al (2012) Periostin promotes chronic allergic inflammation in response to Th2 cytokines. J Clin Invest 122:2590–2600
Matsumoto H (2014) Serum periostin: a novel biomarker for asthma management. Allergol Int 63:153–160
Jia G, Erickson RW, Choy DF, Mosesova S, Wu LC, Solberg OD et al (2012) Periostin is a systemic biomarker of eosinophilic airway inflammation in asthmatic patients. J Allergy Clin Immunol 130:647–654
Kanemitsu Y, Matsumoto H, Izuhara K, Tohda Y, Kita H, Horiguchi T et al (2013) Increased periostin associates with greater airflow limitation in patients receiving inhaled corticosteroids. J Allergy Clin Immunol 132:305–312
Parulekar AD, Mustafa AA, Hanania NA (2014) Periostin, a novel biomarker of Th2-driven asthma. Curr Opin Pulm Med 20:60–65
Corren J, Lemanske RF, Hanania NA, Korenblat PE, Parsey MV, Arron JR et al (2011) Lebrikizumab treatment in adults with asthma. N Engl J Med 365:1088–1098
Bobolea I, Barranco P, Del Pozo V, Romero D, Sanz V, Lopez-Carrasco V et al (2015) Sputum periostin in patients with different severe asthma phenotypes. Allergy. doi:10.1111/all.12580
Kou K, Okawa T, Yamaguchi Y, Ono J, Inoue Y, Kohno M et al (2014) Periostin levels correlate with disease severity and chronicity in patients with atopic dermatitis. Br J Dermatol 171:283–291
Ohta N, Kurakami K, Ishida A, Furukawa T, Saito F, Kakehata S et al (2012) Clinical and pathological characteristics of IgG4-related sclerosing sialadenitis. Laryngoscope 122:572–577
Ishida A, Ohta N, Suzuki Y, Kakehata S, Okubo K, Ikeda H et al (2012) Expression of pendrin and periostin in allergic rhinitis and chronic rhinosinusitis. Allergol Int 61:589–595
Nishizawa H, Matsubara A, Nakagawa T, Ohta N, Izuhara K, Shirasaki T et al (2012) The role of periostin in eosinophilic otitis media. Acta Otolaryngol 132:838–844
Okamoto M, Hoshino T, Kitasato Y, Sakazaki Y, Kawayama T, Fujimoto K et al (2011) Periostin, a matrix protein, is a novel biomarker for idiopathic interstitial pneumonias. Eur Respir J 37:1119–1127
Uchida M, Shiraishi H, Ohta S, Arima K, Taniguchi K, Suzuki S et al (2012) Periostin, a matricellular protein, plays a role in the induction of chemokines in pulmonary fibrosis. Am J Respir Cell Mol Biol 46:677–686
Stankovic KM, Goldsztein H, Reh DD, Platt MP, Metson R (2008) Gene expression profiling of nasal polyps associated with chronic sinusitis and aspirin-sensitive asthma. Laryngoscope 118:881–889
Fujimoto K, Kawaguchi T, Nakashima O, Ono J, Kawaguchi A, Tonan T et al (2011) Periostin, a matrix protein, has potential as a novel serodiagnostic marker for cholangiocarcinoma. Oncol Rep 25:1211–1216
Sirica AE, Almenara JA, Li C (2014) Periostin in intrahepatic cholangiocarcinoma: pathobiological insights and clinical implications. Exp Mol Pathol 97:515–524
Zhu M, Fejzo MS, Anderson L, Dering J, Ginther C, Ramos L et al (2010) Periostin promotes ovarian cancer angiogenesis and metastasis. Gynecol Oncol 119:337–344
Ryner L, Guan Y, Firestein R, Xiao Y, Choi Y, Rabe C et al (2015) Up-regulation of periostin and reactive stroma is associated with primary chemoresistance and predicts clinical outcomes in epithelial ovarian cancer. Clin Cancer Res. pii: clincanres.3111.2014
Xiao ZM, Wang XY, Wang AM (2013) Periostin induces chemoresistance in colon cancer cells through activation of the PI3 K/Akt/survivin pathway. Biotechnol Appl Biochem. doi:10.1002/bab.1193
Erkan M, Kleeff J, Gorbachevski A, Reiser C, Mitkus T, Esposito I et al (2007) Periostin creates a tumor-supportive microenvironment in the pancreas by sustaining fibrogenic stellate cell activity. Gastroenterology 132:1447–1464
Baril P, Gangeswaran R, Mahon PC, Caulee K, Kocher HM, Harada T et al (2007) Periostin promotes invasiveness and resistance of pancreatic cancer cells to hypoxia-induced cell death: role of the beta4 integrin and the PI3k pathway. Oncogene 26:2082–2094
Kotobuki Y, Yang L, Serada S, Tanemura A, Yang F, Nomura S et al (2014) Periostin accelerates human malignant melanoma progression by modifying the melanoma microenviroment. Pigment Cell Melanoma Res 27:630–639
Kudo Y, Iizuka S, Yoshida M, Nguyen PT, Siriwardena SB, Tsunematsu T et al (2012) Periostin directly and indirectly promotes tumor lymphangiogenesis of head and neck cancer. PLoS One. doi:10.1371/journal.pone.0044488
Zhou W, Ke SQ, Huang Z, Flavahan W, Fang X, Paul J et al (2015) Periostin secreted by glioblastoma stem cells recruits M2 tumor-associated macrophage and promotes malignant growth. Nat Cell Biol 17:170–182
Xu D, Xu H, Ren Y, Liu C, Wang X, Zhang H et al (2012) Cancer stem cell-related gene periostin: a novel prognostic marker for breast cancer. PLoS One 7:e46670
Takanami I, Abiko T, Koizumi S (2008) Expression of periostin in patients with non-small cell lung cancer: correlation with angiogenesis and lymphangiogenesis. Int J Biol Markers 23:182–186
Oku E, Kanaji T, Takata Y, Oshima K, Seki R, Morishige S et al (2008) Periostin and bone marrow fibrosis. Int J Hematol 88:57–63
Kashima TG, Nishiyama T, Shimazu K, Shimazaki M, Kii I, Grigoriadis AE et al (2009) Periostin, a novel marker of intramembranous ossification, is expressed in fibrous dysplasia and in c-Fos-overexpressing bone lesions. Hum Pathol 40:226–237
Yamaguchi Y, Ono J, Masuoka M, Ohtta S, Izuhara K, Ikezawa Z et al (2013) Serum periostin levels are correlated with progressive skin sclerosis on patients with systemic sclerosis. Br J Dermatol 168:717–725
Ishikawa K, Yoshida S, Nakao S, Nakama T, Kita T, Asato R et al (2014) Periostin promotes the generation of fibrous membranes in proliferative vitreoretinopathy. FASEB J 28:131–142
Arima K, Ohta S, Takagi A, Shiraishi H, Masuoka M, Ontsuka K et al (2015) Periostin contributes to epidermal hyperplasia in psoriasis common to atopic dermatitis. Allergol Int 64:41–48
Sen K, Lindermeyer MT, Gaspert A, Eichinger F, Neusser MA, Kretzler M et al (2011) Periostin is induced in glomerular injury and expressed de novo in interstitial renal fibrosis. Am J Pathol 179:1756–1767
Bible E (2014) Polycystic kidney disease: Periostin is involved in cell proliferation and interstitial fibrosis in polycystic kidney disease. Nat Rev Nephrol 10:66
Wantanasiri P, Satirapoj B, Charoenpitakchai M, Aramwit P (2015) Periostin: a novel tissue biomarker correlates with chronicity index and renal function in lupus nephritis patients. Lupus. pii:0961203314566634
Huang Y, Liu W, Xiao H, Maitikabili A, Lin Q, Wu T et al (2015) Matricellular protein periostin contributes to hepatic inflammation and fibrosis. Am J Pathol 185:786–797
Zhao S, Wu H, Xia W, Chen X, Zhu S, Zhang S et al (2014) Periostin expression is upregulated and associated with myocardical fibrosis in human failing hearts. J Cardiol 63:373–378
Nair P, Kraft M (2012) Serum periostin as a marker of Th2-dependent eosinophilic airway inflammation. J Allergy Clin Immunol 130:655–656
Ruan K, Bao S, Ouyang G (2009) The multifaceted role of periostin in tumorigenesis. Cell Mol Life Sci 66:2219–2230
Ebrahim AH, Alalawi Z, Mirandola L, Rakhshanda R, Dahlbeck S, Nguyen D et al (2014) Galectins in cancer: carcinogenesis, diagnosis and therapy. Ann Transl Med 2:88
Meijers WC, Januzzi JL, DeFilippi C, Adourian AS, Shah SJ, van Veldhuisen DJ et al (2014) Elevated plasma galectin-3 is associated with near-term rehospitalization in heart failure: a pooled analysis of 3 clinical trials. Am Heart J 167:853–860
Panjwani N (2014) Role of galectins in re-epithelialization of wounds. Ann Transl Med 2:89
Schattner M (2014) Platelets and galectins. Ann Transl Med 2:85
Sziksz E, Kozma GT, Pállinger E, Komlósi ZI, Adori C, Kovács L et al (2010) Galectin-9 in allergic airway inflammation and hyper-responsiveness in mice. Int Arch Allergy Immunol 151:308–317
Niki T, Tsutsui S, Hirose S, Aradono S, Sugimoto Y, Takeshita K et al (2009) Galectin-9 is a high affinity IgE-binding lectin with anti-allergic effect by blocking IgE-antigen complex formation. J Biol Chem 284:32344–32352
Katoh S, Shimizu H, Obase Y, Oomizu S, Niki T, Ikeda M et al (2013) Preventive effect of galectin-9 on double-stranded RNA-induced airway hyperresponsiveness in an exacerbation model of mite antigen-induced asthma in mice. Exp Lung Res 39:453–462
Di Lella S, Sundblad V, Cerliani JP, Guardia CM, Estrin DA, Vasta GR et al (2011) When galectins recognize glycans: from biochemistry to physiology and back again. Biochemistry 50:7842–7857
Newlaczyl AU, Yu LG (2011) Galectin-3 a jack-of-all-trades in cancer. Cancer Lett 313:123–128
Hsu DK, Zuberi RI, Liu FT (1992) Biochemical and biophysical characterization of human recombinant IgE-binding protein, an S-type animal lectin. J Biol Chem 267:14167–14174
Zuberi RI, Hsu DK, Kalayci O, Chen HY, Sheldon HK, Yu L et al (2004) Critical role for galectin-3 in airway inflammation and bronchial hyperresponsiveness in a murine model of asthma. Am J Pathol 165:2045–2053
López E, del Pozo V, Miguel T, Sastre B, Seoane C, Civantos E et al (2006) Inhibition of chronic airway inflammation and remodeling by galectin-3 gene therapy in a murine model. J Immunol 176:1943–1950
Pilette C, Colinet B, Kiss R, André S, Kaltner H, Gabius HJ (2007) Increased galectin-3 expression and intra-epithelial neutrophils in small airways in severe COPD. Eur Respir J 29:914–922
Nishi Y, Sano H, Kawashima T, Okada T, Kuroda T, Kikkawa K et al (2007) Role of galectin-3 in human pulmonary fibrosis. Allergol Int 56:57–65
Gao P, Gibson PG, Baines KJ, Yang I, Upham JW, Reynolds PN et al (2015) Anti-inflammatory deficiencies in neutrophilic asthma: reduced galectin-3 and IL-1RA/IL-1β. Respir Res 16:5
Baines KJ, Simpson JL, Wood LG, Scott RJ, Fibbens NL, Powell H et al (2014) Sputum gene expression signature of 6 biomarkers discriminates asthma inflammatory phenotypes. J Allergy Clin Immunol 133:997–1007
George BJ, Reif DM, Gallagher JE, Williams-DeVane CR, Heidenfelder BL, Hudgens EE et al (2015) Data-driven asthma endotypes defined from blood biomarker and gene expression data. PLoS One 10:e0117445
Christenson SA, Steiling K, van den Berge M, Hijazi K, Hiemstra PS, Postma DS et al (2015) Asthma-COPD overlap. Clinical relevance of genomic signatures of type 2 inflammation in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 191:758–766
Gustafsson M, Nestor CE, Zhang H, Barabási AL, Baranzini S, Brunak S et al (2014) Modules, networks and systems medicine for understanding disease and aiding diagnosis. Genome Med 6:82
Authors’ contributions
AC, LDF and CF carried on bibliographic research and took part in the draft of the paper; PM, AMR and GWC contributed to bibliographic research and reviewed the final manuscript. All authors read and approved the final manuscript.
Acknowledgements
This work was partially supported by ARMIA (Associazione Ricerca Malattie Immunologiche ed Allergiche).
Compliance with ethical guidelines
Competing interests The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Additional information
Alessandra Chiappori and Laura De Ferrari contributed equally to this work
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Chiappori, A., De Ferrari, L., Folli, C. et al. Biomarkers and severe asthma: a critical appraisal. Clin Mol Allergy 13, 20 (2015). https://doi.org/10.1186/s12948-015-0027-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12948-015-0027-7