
Abstract
Purpose
There are few reports about balloon dilatation combined with internal and external drainage tube in the treatment of ureteral stricture under interventional therapy. The aim of the study is to explore the safety, effectiveness and long-term efficacy of this treatment strategy.
Materials and methods
It is a retrospective and observational study. From October 2013 to October 2016, 42 patients with benign lower ureteral stricture received interventional treatment. Balloon dilatation combined with internal and external drainage tube implantation were used. There were 25 male patients and 17 female patients. There were 7 cases (16.7%) with congenital ureteral stricture, 12 cases (28.6%) with inflammation, 15 cases (35.7%) with ureteral stricture after lithotomy or lithotripsy, and 8 cases (19.0%) with ureteral stricture after pelvic or abdominal surgery. After the drainage tube was removed, B ultrasound, enhanced CTU or IVP of urinary system were reexamined every six months. The follow-up time was 12–60 months.
Results
The age was 52.9 ± 11.6 years. The length of ureteral stricture was 1.1 ± 0.5 cm. 42 patients completed interventional treatment, the technical success rate was 100%, no ureteral perforation, rupture or other complications were identified. Preoperative urea nitrogen 9.2 ± 2.3 mmol/L and creatinine 175.8 ± 82.8umol/L. Urea nitrogen and creatinine were 3.8–9.1 mmol/L and 45.2–189.6 umol/L when removing the drainage tube. There were significant differences in the levels of urea nitrogen and creatinine before and after tube removal (P < 0.05). The ureteral patency rate was 100% at 6 months, 93% at 12 months, 83% at 18 months, 79% at 24 months, 76% at 30 months and 73% at 36–60 months. The overall success rate was 73%. Multivariate Cox regression analysis showed that stenosis length was a risk factor for postoperative patency (P < 0.05).
Conclusion
Balloon dilatation combined with internal and external drainage tube implantation in the treatment of benign lower ureteral stricture is safe and effective.
Similar content being viewed by others


Introduction
Ureteral stricture is a relatively rare urinary system disease, which refers to ureteral stenosis caused by various reasons, eventually leading to hydronephrosis or renal failure [1]. There are many causes of ureteral stricture, including congenital and secondary ureteral stricture. The causes of secondary ureteral stricture include calculus, inflammation, injury after lithotripsy [2], ureteral related operation, tumor invasion, retroperitoneal fibrosis, iatrogenic injury caused by abdominal and pelvic surgery, radiotherapy, etc. [3, 4]. Especially iatrogenic injury, although with the improvement of endoscopic technology and surgical methods, the incidence of iatrogenic injury decreased continuously, from 10% 20 years ago to 3–6% 10 years ago, and even less than 0.2% reported in recent years [5, 6]. However, due to the increase of the number of operations, the absolute number of iatrogenic injuries is rising, which should be paid great attention by medical staff. Commonly used treatments for ureteral strictures include open surgery and minimally invasive treatment. Internal and external drainage tubes are mostly used for drainage of the biliary system [7]. There were few reports of balloon dilatation combined with internal and external drainage tube in the treatment of ureteral stricture under interventional therapy, and the observation of long-term therapeutic effect of balloon dilatation is scarce in the literature. This study retrospectively collected the data of patients with ureteral stricture treated by balloon dilatation combined with internal and external drainage tube in the Interventional Therapy Department of our hospital, to analyse the safety, effectiveness and long-term efficacy of this treatment method.
Materials and methods
General information
From October 2013 to October 2016, clinical data from 42 patients with benign lower ureteral stenosis were collected, who were treated in the Interventional Therapy Department of Wuhan Union Hospital Affiliated to Tongji College of Huazhong University of science and technology. Balloon dilatation combined with internal and external drainage tube implantation were used. The study was approved by the hospital ethics committee, and all patients' data collection was informed and agreed by the patients and their families. All patients had unilateral single segment benign lower ureteral stenosis. B-ultrasound, enhanced CTU or/and MRU examination were performed before the operation to determine the cause, location and length of the stenosis. Antegrade pyelography was performed during the operation. All patients had different degrees of hydronephrosis, which were divided into mild (less than 3 cm), moderate (3–4 cm) and severe (more than 4 cm).
Intraoperative consumables: percutaneous renal puncture Kit (NPAS-100-RH-NT, Cook, USA), internal and external drainage catheter (ULT10.2-38-40-P-32S-CLB-RH, Cook, USA), 6F vascular sheath (TERUMO6F-10CM, Terumo, Japan), 0.035 inch guide wire (RF*GA35153M, RF*PA35263M, Terumo, Japan), 6 mm/8 mm diameter balloon (PTA5-35-135-6-8.0, PTA5-35-135-8-8.0, Cook, USA), 5F multipurpose catheter (MPA1, Cordis, USA).
Method
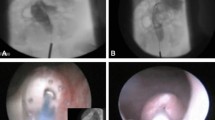
Endoscopic retrograde ureteral dilatation with double-J stent implantation and renal puncture balloon dilatation with internal and external drainage tube implantation are both standard treatment methods in our center, and which treatment method is selected is evaluated according to the imaging data of patients before treatment. In this group of patients, we chose the latter treatment modality. After local anesthesia, Chiba needle was punctured into the renal calyces of the middle group under the guidance of ultrasound. 6F catheter sheath was introduced under Digital subtraction angiography (DSA), and 5F multipurpose catheter was introduced through the catheter sheath. Contrast agent was injected to show that the renal pelvis and calyces were dilated, the lower ureter was narrow, and the proximal ureter was significantly dilated. During the operation, we selected a balloon with a diameter of 6 mm or 8 mm by referring to the diameter of the ureter in the normal area of the patient. The balloon catheter was used to dilate the ureteral stricture (Fig. 1). The inflation time of the balloon should not exceed 5 min each time; the balloon can be inflated repeatedly, but at an interval of 3–5 min. Prepare the 10.2F internal and external drainage tube, and open the appropriate side hole in the proximal part. The guide wire was retained and the sheath was pulled out. A 10.2F internal and external drainage tube was inserted through the guide wire, and the distal end of the tube was looped into the bladder cavity. The proximal side hole of the catheter is located in the renal pelvis, and the end of the catheter is connected with a drainage bag (Fig. 2). The drained urine was routinely tested and cultured, and targeted treatment was performed based on the results. After the hematuria disappears, the connecting port outside the body of the internal and external drainage tubes is closed with a heparin cap and no longer connected to the drainage bag. The drainage tube was washed with gentamicin saline once a month. Renal function and imaging examination were performed every two months to evaluate whether the drainage was sufficient. According to previous experience, the incidence of ureteral restenosis is very high after removal of the drainage tube within 6 months, so we routinely keep the drainage tube for 6 months. Six months later, the end of the internal and external drainage tube was pulled out from the bladder cavity to the renal pelvis under fluoroscopy, and the contrast agent was injected through the tube (Fig. 3).

Fluoroscopic image showing the guidewire inserted through a percutaneous access to the urinary bladder, ureteral stenosis was dilated with a balloon

The internal and external drainage tube was implanted under fluoroscopy, with the distal end of the tube located in the bladder and the side holes of the tube located in the renal pelvis

The end of the drainage tube is pulled into the renal pelvis. The contrast medium smoothly enters the bladder cavity through the ureter by drainage tube radiography
The criteria for tube removal: Imaging examination showed that there was no ureteropelvic dilatation. Renal function tests revealed a significant decrease in urea nitrogen and creatinine levels. The distal end of the drainage tube was moved from the bladder to the renal pelvis before tube removal, and contrast agent was injected through the external orifice of the tube, which showed that the contrast agent smoothly entered the bladder from the renal pelvis through the ureter. If the above criteria are met, remove the tube. If not met, the end of the drainage tube is repositioned into the bladder with a guide wire. Repeat the above operations after three months.
Follow up
After the internal and external drainage tubes were removed, B-ultrasound, enhanced CTU or IVP of urinary system were reexamined every six months (Fig. 4). The overall success rate is defined as the patency rate at 36–60 months of follow-up.

Recheck CT to confirm that the position of drainage tube is satisfactory
Statistical analysis
All analyses were performed using SPSS software (Version 24.0, IBM, Armonk, New York). The measurement data were expressed as mean ± standard deviation. The counting data are expressed as percentages. Paired T test was used for renal function before operation and tube removal, Cox regression analysis was used for multivariate analysis, P < 0.05 showed that the difference was statistically significant.
Results
There were 25 male patients and 17 female patients. The average age was 52.9 ± 11.6 years (range, 27–73 years). According to age, there were 6 young (< 40 years old), 23 middle-aged (40–60 years old) and 13 elderly (> 60 years old) (Tables 1, 2). There were 6 cases of mild hydronephrosis, 15 cases of moderate hydronephrosis and 21 cases of severe hydronephrosis. The length of ureteral stricture was 0.2–2.1 cm, with an average of 1.1 ± 0.5 cm. The length of ureteral stricture was graded according to the following criteria. Mild stenosis: stenosis length < 0.8 cm (18 cases), moderate stenosis: stenosis length 0.8–1.5 cm (16 cases), severe stenosis: stenosis length > 1.5 cm (8 cases). There were 7 cases (16.7%) with congenital ureteral stricture, 12 cases (28.6%) with inflammation, 15 cases (35.7%) with ureteral stricture after lithotomy or lithotripsy, and 8 cases (19.0%) with ureteral stricture after pelvic or abdominal surgery. Preoperative urea nitrogen was 3.9–12.9 mmol/L, with an average of 9.2 ± 2.3 mmol/L. Preoperative creatinine was 54.5–339.5 umol / L, with an average of 175.8 ± 82.8 umol / L (Tables 1, 2).
All 42 patients completed the interventional operation, and the technical success rate was 100%. The mean follow-up time was 42.6 ± 16.8 months (range, 12–60 months). In all 42 patients, all the internal and external drainage tubes were successfully removed according to our criteria for tube removal. There were 9 patients with 6 mm diameter balloon and 33 patients with 8 mm diameter balloon during the operation. After the internal and external drainage tube was implanted, no complications such as ureteral perforation and rupture occurred. The clearance time of hematuria in the drainage bag was 1–4 days, with an average of 1.9 ± 0.9 days. The internal and external drainage tubes indwelling time: 6 months in 33 cases, 9 months in 9 cases (Table 1). Urea nitrogen was 6.3 ± 1.4 mmol/L, and the creatinine was 84.4 ± 27.3umol/L when the internal and external drainage tubes were removed (Table 2). There were significant differences in the levels of urea nitrogen and creatinine before operation and during tube removal (P < 0.05) (Table 3). There were 5 patients with bladder irritation after drainage tube implantation, who improved with oral antibiotic therapy.
There were 3 cases of ureteral restenosis in 12 months, 4 cases in 18 months, 2 cases in 24 months, 1 case in 30 months and 1 case in 36 months. The ureteral patency rate was 100% at 6 months, 93% at 12 months, 83% at 18 months, 79% at 24 months, 76% at 30 months and 73% at 36–60 months (Fig. 7). The overall success rate was 73%.
Multivariate Cox regression analysis showed that the degree of stenosis was a risk factor for patency rate (P < 0.05) (Table 4, Figs. 5 and 6).

Patency rate of the drainage tube during follow-up in patients with different degrees of stenosis

Cox regression analysis showed that the degree of stenosis was a risk factor for patency rate (P < 0.05)
Discussion
Commonly used treatments for ureteral strictures include open surgery and minimally invasive treatment. The methods of minimally invasive treatment include ureteroscopic treatment and interventional treatment. Ureteroscopic treatment includes transurethral cold knife ureterotomy, holmium laser ureterotomy [8, 9], rigid ureteroscopic dilatation, balloon dilatation, ureteral stent implantation, etc. Esteban Emiliani et al. [10] reported that endoureterotomy and endopyelotomy should be considered a reasonable treatment option in selected patients of ureteral strictures. Ureteroscopy is generally retrograde to the ureter through the bladder. For lower ureteral stricture, due to the stricture of the ureteral opening or the failure of the guide wire to travel far in the ureter, the operation can not be completed retrogradely [2, 11, 12]. Therefore, for lower ureteral stenosis, antegrade interventional therapy has certain advantages. Antegrade interventional therapy includes balloon dilatation and ureteral stent implantation. Li et al. [13] reported 78 cases of lower ureteral stenosis, using percutaneous nephrostomy combined with balloon dilatation, the effective rate was 92%. In this group of 42 patients, the technical success rate was 100%, which was consistent with that reported in the literature.
Banner et al. [14] first reported the use of balloon dilatation in the treatment of ureteral stricture in 1983. A large number of studies have confirmed that balloon dilatation has a significant effect in the treatment of ureteral stenosis [15, 16], and has become one of the main treatment for benign ureteral stenosis [1]. Wai Loon Yam et al. [17] found that balloon dilatation of benign ureteric stricture is a feasible option, its effect can be long-lasting in selected patients. Jianhua Li et al.[13] demonstrated that percutaneous renal access anterograde flexible ureteroscope plus retrograde balloon dilatation is safe, effective and mini-invasive. Yam et al. [18] reported that balloon dilatation is safe and effective in the treatment of ureteral stricture, and the effective duration is long. The main complications were mucosal injury, ureteral perforation, hematuria and lumbar discomfort. The most common postoperative complication in this group of patients was hematuria, which lasted for 1–4 days. No serious complications such as ureteral rupture occurred. Kuntz NJ et al. retrospectively analyzed 151 cases of ureteral stricture treated by balloon dilatation, the success rate of operation was 95%, and the incidence of intraoperative complications was 5% [19]. Referring to the depth of ureteroscopic cold knife incision for the whole layer of the ureter, directly to the adipose tissue around the ureter [20], we believe that the full expansion of the ureter is helpful to improve the therapeutic effect. In this group of 42 patients, our selected balloon diameter was 6–8 mm, and no complications such as ureteral rupture occurred.
In 1967, Zimskind first implanted the stent into the ureter to relieve ureteral obstruction. In 1987, double-J stent was used for the first time. The commonly used ureteral stents are double-J stent [21], metal stent [22, 23], new anti biological peptide stent, etc. According to different conditions, it is very important to choose the appropriate stent [24]. For benign ureteral stricture, double-J stent is the most commonly used. Metal stents are mostly used for malignant ureteral strictures [25]. Ureteral stents can be used alone or in combination after balloon dilatation or endoscopic treatment [26]. Studies have shown that double-J stent after balloon dilatation can prevent ureteral rebound and scar contraction, help to drain urine and restore renal function. Hua-liang Yu et al. [27] found that treatment of benign ureteral stricture by double J stents using high-pressure balloon angioplasty produces a better therapeutic effect.
The commonly used drainage methods include internal drainage, external drainage and internal – -external drainage [28, 29]. External drainage refers to the implantation of nephrostomy tube after renal puncture. Internal drainage is accomplished by placement of a ureteral stent [30]. Internal–external drainage is performed by simultaneous ureteral stent implantation and external drainage tube implantation after renal puncture [31]. There are many benefits to preserving the external drainage tube when implanting a double-J stent by renal puncture. Because hematuria is often present shortly after renal puncture, blood clots may block the double-J stent. In the stage of hematuria, opening the external drainage tube can avoid double-J stent blockage. If it is necessary to replace the double-J stent, it can also be operated through the access of the external drainage tube. There are few reports about indwelling internal and external drainage tube after balloon dilatation. In this group, 10.2F internal and external drainage tube is used. Using this method, the patient does not need an external drainage bag, and the urine can flow into the bladder through the tube. The tube can be flushed regularly through the opening left outside the body to prevent blockage. The opening retained outside the body can be used as a path for removing or replacing the tube, which is directly operated and very convenient. Different from the double-J stent, the removal or replacement must use cystoscopy or catcher, which is complex and more painful for patients. The tube can be pulled out directly, and the success rate of tube removal is higher than that of double J stent. According to the research report, the success rate of percutaneous antegrade removal of double J stent is 93–97% [32, 33]. Cheng-Shi Chen [34] reported the success rate of retrograde removal of double-J stent was 97.44% (304/312). The success rate of tube removal in this study was 100%, which was higher than the success rate of double-J stent removal reported in the literature.
It has been reported that in the treatment of ureteral strictures, the indwelling time of double-J stent is about 6 weeks–3 months [35,36,37]. If it is necessary to continue indwelling, the double-J stent must be replaced [38]. In this study, we retained the internal and external drainage tubes for 6 months before reexamination. According to the previous experience at our center, the risk of restenosis is high after removal of the tube within 6 months. Although the usual indwelling time of double-J stent is 6 weeks to 3 months, some scholars have put forward different opinions. The study by Li et al. suggests that the indwelling time is related to the efficacy, and the recommended indwelling time is 6 months [39]. The indwelling time of internal and external drainage tube is longer due to regular flushing. The longest indwelling time in this group was 9 months, no tube blockage occurred. All drainage tubes were successfully removed on schedule. In this group, restenosis mainly occurred within 36 months, especially within 18 months, which indicates that ureteral restenosis is easy to occur in the process of ureteral repair (Fig. 7) Therefore, we suggest balloon dilatation combined with internal and external drainage tube implantation to prevent ureteral restenosis. After 36 months of follow-up, there was no ureteral stricture in this group, This indicates a low incidence of mid- to long-term restenosis after stable repair of the ureter.

The ureteral patency rate was 100% at 6 months, 93% at 12 months, 83% at 18 months, 79% at 24 months, 76% at 30 months and 73% at 36–60 months
In this group, the 6-month ureteral patency rate was 100%, the 12-month ureteral patency rate was 93%, the 18 month ureteral patency rate was 83%, the 24 month ureteral patency rate was 79%, the 30 month ureteral patency rate was 76%, and the 36–60 month ureteral patency rate was 73% (Fig. 7). The overall success rate was 73%. This is consistent with the success rate of 76.5% reported by Han [9] for endoureterotomy. There are many prognostic factors affecting the efficacy, such as the cause of stenosis [40], the length of stenosis [41], the time of stenosis [42], stent indwelling time [43] and the location of stenosis. According to the prospective study of Byun SS et al. [44], the length and etiology of ureteral stenosis are the factors influencing the effect of balloon dilatation. It has been reported that the successful rate of balloon dilatation is high when the stenosis length is less than 2 cm. The success rate of ureteral dilatation is high when the stenosis time is less than 3–6 months [15]. Cox regression analysis showed that the degree of ureteral stricture was a risk factor for restenosis, which is consistent with the results of other studies. However, the sample size of this group is relatively small, and it is a single center retrospective analysis. In the later stage, we can design a multi center, prospective, randomized controlled study to obtain more reliable research results.
Conclusion
Balloon dilatation combined with internal and external drainage tube implantation in the treatment of benign lower ureteral stricture is a safe and reliable treatment strategy, with satisfactory short-term and long-term effects.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
References
Tran H, Arsovska O, Paterson RF, Chew BH. Evaluation of risk factors and treatment options in patients with ureteral stricture disease at a single institution. Can Urol Assoc J. 2015;9(11–12):E921–4. https://doi.org/10.5489/cuaj.3057.
May PC, Hsi RS, Tran H, Stoller ML, Chew BH, Chi T, Usawachintachit M, Duty BD, Gore JL, Harper JD. The Morbidity of ureteral strictures in patients with prior ureteroscopic stone surgery: multi-institutional outcomes. J Endourol. 2018;32(4):309–14. https://doi.org/10.1089/end.2017.0657.
Liatsikos EN, Karnabatidis D, Katsanos K, Kallidonis P, Katsakiori P, Kagadis GC, Christeas N, Papathanassiou Z, Perimenis P, Siablis D. Ureteral metal stents: 10-year experience with malignant ureteral obstruction treatment. J Urol. 2009;182(6):2613–7. https://doi.org/10.1016/j.juro.2009.08.040.
Ghosh B, Jain P, Pal DK. Managing mid and lower ureteral benign strictures: the laparoscopic way. J Laparoendosc Adv Surg Tech A. 2018;28(1):25–32. https://doi.org/10.1089/lap.2017.0256.
Ambani SN, Faerber GJ, Roberts WW, Hollingsworth JM, Wolf JS Jr. Ureteral stents for impassable ureteroscopy. J Endourol. 2013;27(5):549–53. https://doi.org/10.1089/end.2012.0414.
Bader MJ, Eisner B, Porpiglia F, Preminger GM, Tiselius HG. Contemporary management of ureteral stones. Eur Urol. 2012;61(4):764–72. https://doi.org/10.1016/j.eururo.2012.01.009.
Matsubara S, Isayama H, Nakai Y, Kawakubo K, Yamamoto N, Saito K, Saito T, Takahara N, Mizuno S, Kogure H, Ishizawa T, Arita J, Hasegawa K, Koike K. Endoscopic ultrasound-guided gallbladder drainage with a combined internal and external drainage tubes for acute cholecystitis. J Gastroenterol Hepatol. 2020;35(10):1821–7. https://doi.org/10.1111/jgh.15065.
Gnessin E, Yossepowitch O, Holland R, Livne PM, Lifshitz DA. Holmium laser endoureterotomy for benign ureteral stricture: a single center experience. J Urol. 2009;182(6):2775–9. https://doi.org/10.1016/j.juro.2009.08.051.
Han PK, Rohan M, Mohd AB. The short-term outcome of laser endoureterotomy for ureteric stricture. Med J Malaysia. 2013;68(3):222–6.
Emiliani E, Breda A. Laser endoureterotomy and endopyelotomy: an update. World J Urol. 2015;33(4):583–7. https://doi.org/10.1007/s00345-014-1405-3.
Lucas JW, Ghiraldi E, Ellis J, Friedlander JI. Endoscopic management of ureteral strictures: an update. Curr Urol Rep. 2018;19(4):24. https://doi.org/10.1007/s11934-018-0773-4.
Zhao P. Endoscopic management of ureteral stricture: NYU case of the month, August 2018. Rev Urol. 2018;20(3):140–2. https://doi.org/10.3909/riu0819.PMID:30473642;PMCID:PMC6241893.
Li J, Chen L, Li J, Wang X. Efficacy and safety of percutaneous renal access flexible ureteroscope plus balloon dilatation for patients with complex lower ureterostenosis. Zhonghua Yi Xue Za Zhi. 2014;94(46):3642–5.
Banner MP, Pollack HM, Ring EJ, Wein AJ. Catheter dilatation of benign ureteral strictures. Radiology. 1983;147(2):427–33. https://doi.org/10.1148/radiology.147.2.6836121.
Lu C, Zhang W, Peng Y, Li L, Gao X, Liu M, Fang Z, Wang Z, Ming S, Dong H, Shen R, Xie F, Sun Y, Gao X. Endoscopic balloon dilatation in the treatment of benign ureteral strictures: a meta-analysis and systematic review. J Endourol. 2019;33(4):255–62. https://doi.org/10.1089/end.2018.0797.
Peng Y, Li X, Li X, Zhang C, Yang K, Xiong G, Zhou L, Wang G. Fluoroscopy-free minimally invasive ureteral stricture balloon dilatation: a retrospective safety and efficacy cohort study. Transl Androl Urol. 2021;10(7):2962–9. https://doi.org/10.21037/tau-21-203.PMID:34430399;PMCID:PMC8350239.
Yam WL, Lim SKT, Ng KS, Ng FC. Is there still a role of balloon dilatation of benign ureteric strictures in 2019? Scand J Urol. 2020;54(1):80–5. https://doi.org/10.1080/21681805.2020.1716845.
Yam WL, Lim SKT, Teo JK, et al. 130 Balloon dilatation of ureteric and ureteroileal strictures. Eur Urol Suppl. 2016;15(3):e130–e130.
Kuntz NJ, Neisius A, Tsivian M, Ghaffar M, Patel N, Ferrandino MN, Sur RL, Preminger GM, Lipkin ME. Balloon dilation of the ureter: a contemporary review of outcomes and complications. J Urol. 2015;194(2):413–7. https://doi.org/10.1016/j.juro.2015.02.2917.
Dubosq F, Pasqui F, Girard F, Beley S, Lesaux N, Gattegno B, Thibault P, Traxer O. Endoscopic lithotripsy and the FREDDY laser: initial experience. J Endourol. 2006;20(5):296–9. https://doi.org/10.1089/end.2006.20.296.
Mohyelden K, Hussein HA, El Helaly HA, Ibrahem H, Abdelwahab H. Long-term outcomes of two ipsilateral vs single double-j stent after laser endoureterotomy for bilharzial ureteral strictures. J Endourol. 2021;35(6):775–80. https://doi.org/10.1089/end.2020.0956.
Guandalino M, Droupy S, Ruffion A, Fiard G, Hutin M, Poncet D, Pereira B, Paparel P, Terrier JE. Stent Allium urétéral dans la prise en charge des sténoses urétérales Étude rétrospective multicentrique [The Allium ureteral stent in the management of ureteral stenoses, a retrospective, multicenter study]. Prog Urol. 2017;27(1):26–32. https://doi.org/10.1016/j.purol.2016.11.005.
Benson AD, Taylor ER, Schwartz BF. Metal ureteral stent for benign and malignant ureteral obstruction. J Urol. 2011;185(6):2217–22. https://doi.org/10.1016/j.juro.2011.02.008.
Lundeen CJ, Forbes CM, Wong VKF, Lange D, Chew BH. Ureteral stents: the good the bad and the ugly. Curr Opin Urol. 2020;30(2):166–70. https://doi.org/10.1097/MOU.0000000000000701.
Miyazaki J, Onozawa M, Takahashi S, Maekawa Y, Yasuda M, Wada K, Maeda Y, Masaki T, Yamaguchi A, Suzuki M, Sakai Y, Kimura T, Takai M, Seike K, Hashimoto T, Yamamoto S. The resonance® metallic ureteral stent in the treatment of malignant ureteral obstruction: a prospective observational study. BMC Urol. 2019;19(1):137. https://doi.org/10.1186/s12894-019-0569-y.PMID:31881875;PMCID:PMC6935232.
Lin CM, Tsai TH, Lin TC, Tang SH, Wu ST, Sun GH, Cha TL. Holmium: yttrium-aluminum-garnet laser endoureterotomy for benign ureteral strictures: a single-centre experience. Acta Chir Belg. 2009;109(6):746–50. https://doi.org/10.1080/00015458.2009.11680528.
Yu HL, Ye LY, Lin MH, Yang Y, Miao R, Hu XJ. Treatment of benign ureteral stricture by double J stents using high-pressure balloon angioplasty. Chin Med J (Engl). 2011;124(6):943–6.
Thornton RH, Covey AM. Urinary drainage procedures in interventional radiology. Tech Vasc Interv Radiol. 2016;19(3):170–81. https://doi.org/10.1053/j.tvir.2016.06.002.
Adamo R, Saad WE, Brown DB. Management of nephrostomy drains and ureteral stents. Tech Vasc Interv Radiol. 2009;12(3):193–204. https://doi.org/10.1053/j.tvir.2009.09.003.
Hausegger KA, Portugaller HR. Percutaneous nephrostomy and antegrade ureteral stenting: technique-indications-complications. Eur Radiol. 2006;16(9):2016–30. https://doi.org/10.1007/s00330-005-0136-7.
Tal R, Bachar GN, Baniel J, Belenky A. External-internal nephro-uretero-ileal stents in patients with an ileal conduit: long-term results. Urology. 2004;63(3):438–41. https://doi.org/10.1016/j.urology.2003.09.062.
Kim ET, Yang WJ, Shin JH, Wang YH, Narcise L. Clinical utility of the modified snare technique for percutaneous antegrade removal of double J ureteral stents. J Vasc Interv Radiol. 2020;31(1):155–161. https://doi.org/10.1016/j.jvir.2019.04.026. [Epub 2019 Aug 13. Erratum in: J Vasc Interv Radiol. 2020 May;31(5):868]
Shin JH, Yoon HK, Ko GY, Sung KB, Song HY, Choi E, Kim JH, Kim JW, Kim KR, Kwon J. Percutaneous antegrade removal of double J ureteral stents via a 9-F nephrostomy route. J Vasc Interv Radiol. 2007;18(9):1156–61. https://doi.org/10.1016/j.jvir.2007.06.016.
Chen CS, Shin JH, Li HL, Guo CY, Kim JW, Zheng L, Yao QJ, Geng X, Wang T. Analysis of the factors influencing retrograde removal of double J ureteral stents using a simple snare technique in female patients. Ann Transl Med. 2021;9(8):674. https://doi.org/10.21037/atm-21-1113.PMID:33987372;PMCID:PMC8106078.
Hibi H, Yamada Y, Nonomura H, Hatano Y, Mitsui K, Taki T, Honda N, Fukatsu H. Percutaneous ureteral incision with a small-caliber flexible ureteroscope. JSLS. 2003;7(2):107–10.
el Khader K, Koutani A, Tazi K, Iben Attya A, Hachimi M, Lakrissa A. Drainage interne par sondes urétérales double J. A propos de 91 cas [Internal drainage by double J ureteral stents. 91 cases]. Ann Urol (Paris). 1996;30(5):235–9.
Lojanapiwat B, Soonthonpun S, Wudhikarn S. Endoscopic treatment of benign ureteral strictures. Asian J Surg. 2002;25(2):130–3. https://doi.org/10.1016/S1015-9584(09)60160-3.
Leslie SW, Sajjad H. Double J placement methods comparative analysis. 2021 Sep 17. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021.
Li SQ, Yang DA, Li XT. Double J stent for pelvis-ureter junction stricture. Zhonghua Wai Ke Za Zhi. 1994;32(2):117–8.
Punekar SV, Rao SR, Swami G, Soni AB, Kinne JS, Karhadkar SS. Balloon dilatation of ureteric strictures. J Postgrad Med. 2000;46(1):23–5.
Van Cangh PJ, Nesa S. Endopyelotomy. Prognostic factors and patient selection. Urol Clin North Am. 1998;25(2):281–8. https://doi.org/10.1016/s0094-0143(05)70015-x.
Bozkurt OF, Tepeler A, Sninsky B, Ozyuvali E, Ziypak T, Atis G, Daggulli M, Resorlu B, Caskurlu T, Unsal A. Flexible ureterorenoscopy for the treatment of kidney stone within pelvic ectopic kidney. Urology. 2014;84(6):1285–9. https://doi.org/10.1016/j.urology.2014.07.041.
Hu J, Lai C, Gao M, Li K, He W, Zhu D, Xie W, Wu H, Xu M, Huang J, Han J. A nomogram to predict stricture-free survival in patients with ureteral stricture after balloon dilation. BMC Urol. 2021;21(1):129. https://doi.org/10.1186/s12894-021-00896-3.PMID:34530805;PMCID:PMC8444546.
Richter F, Irwin RJ, Watson RA, Lang EK. Endourologic management of benign ureteral strictures with and without compromised vascular supply. Urology. 2000;55(5):652–7. https://doi.org/10.1016/s0090-4295(00)00484-2.
Acknowledgements
Thank Pro. Guohui Liu for his help in English writing. Thank Dr. Wei Wang for his help in data collection. Thank Dr. Kang Zhang for his help in reference. Thank you for all those who offer help and support in this research.
Funding
No funding is provided in this study.
Author information
Authors and Affiliations
Contributions
HL have made substantial contributions to the conception and design of the work, and the acquisition, analysis of data, as well as manuscript writing. CZ have made contributions to the design of the work. BL have made contributions to the acquisition, analysis of data. BX have made contributions to analysis, interpretation of data, and manuscript writing. All authors have agreed both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work. CZ is corresponding author, and responsible for ensuring that all listed authors have approved the manuscript before submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The medical ethics committee of our college (Wuhan Union Hospital, Tongji Medical College, Huazhong University of science and technology, Wuhan, Hubei Province) approved the retrospective study and gave up the written informed consent. Although the ethics committee gave up the written consent, for the safety and rationality of the research, all participants signed informed consent for the study. Of course, all the patients signed the informed consent before the operation. During follow-up, we informed patients about the study and they agreed to use their data. We confirm that all methods were performed in accordance with the relevant guidelines and Declaration of Helsinki.
Consent for publication
All participants' information, images and inspection results are agreed to be published, and we have obtained written consent form the participants and our college. The details, images will be freely available on the internet and may be seen by the general public. The consent form is available if requested. These patients have not been reported in any other submission by anyone.
Competing interests
We declare that we have no financial and personal relationships with other people or organizations that can inappropriately influence our work, there is no professional or other personal interest of any nature or kind in any product, service and company that could be construed as influencing the position presented in this manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lu, H., Zheng, C., Liang, B. et al. Analysis of long-term effect of ureteral balloon dilatation combined with internal and external drainage tube in the treatment of benign ureteral stricture. BMC Urol 22, 4 (2022). https://doi.org/10.1186/s12894-022-00952-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12894-022-00952-6