
Abstract
Background
The present research explored the effect of an educational program based on the health belief model (HBM) on prisoners’ HIV preventive behaviors in the south of Iran.
Methods
The present quasi-experimental research was conducted in 2019–20 on 280 prisoners, 140 in the control group (CG) and 140 in the intervention group (IG). The sampling was simple randomized. The data were collected using a questionnaire in two parts, one exploring the demographic information and the other the HBM constructs. The final follow-up was completed 3 months after the educational intervention (8 sessions long) in November 2020.
Results
After the intervention, statistically significant between-group differences were found in the healthy behavior score and all HBM constructs except for the perceived barriers (p < 0.001). Perceived severity and susceptibility were found to be the strongest predictors of HIV preventive behaviors.
Conclusion
The educational intervention showed to positively affect the adoption of preventive behaviors mediated by the HBM constructs. To remove barriers to HIV preventive behaviors or any other healthy behavior, researchers are suggested to develop multi-level interventions (beyond the personal level) to gain better findings.
Similar content being viewed by others

Background
HIV, the virus accounting for the acquired immunodeficiency syndrome (AIDS), is one of the world’s most serious health issues. Approximately 38 million people are currently living with HIV. Tens of million people have died of AIDS-related reasons since the beginning of the epidemic [1]. Despite a global decline in the prevalence of the new HIV infection, in countries such as Iran, the rate of HIV infection is still high. In 2019, the estimated number of HIV patients in Iran was 59,000. Every year, about 4100 new infected cases are diagnosed, and 2500 AIDS-related mortalities occur in the country [2]. Among different populations, prisoners are at a higher risk of HIV, HCV, and HBV infections due to high-risk behaviors such as drug abuse and unprotected sex [3]. . Prisoners are 7 to 12 times more likely to be infected with HIV than the public [4]. The outbreak of the disease in Kermanshah Prison in 1995 triggered a national response to HIV [2].
Among the estimated 10.2 million prisoners world-wide, 3.8% were found to be HIV-positive [5]. A systematic review/meta-analysis of prisoners in 2019 showed an incidence rate of 0 (in Bosnia and Herzegovina) to over 20% (in Iran, Zambia, Spain) [6]. Similarly, in another systematic review, the prevalence of HIV was found to be between 0 and 24.40% among Iranian prisoners [7]. In two other studies, the same rate was reported to be 1.23 and 2.1% [8, 9].
Specific policies are made to prevent and control HIV infection in the prisons of Iran. Examples are screening the newly admitted prisoners, distributing condoms for safe sexual activities [10], initiating and expanding the administration of methadone maintenance therapy, setting up triangular clinics in prisons and exchanging needle/syringe regularly [9, 11].
Prisons are hazardous places for HIV infection due to the overcrowd, poor nutrition, limited healthcare, continued drug abuse, unsafe injections, unprotected sex and tattoos. In addition, many prisoners come from marginalized populations – such as the injecting drug users (IDU), who have already experienced an elevated risk of HIV [12].
As suggested by the World Health Organization (WHO), the best way to control HIV is to educate populations that are more at risk [13]. . There is research evidence that health education and knowledge promotion are the best ways to fight AIDS before it grows any further [14]. The HBM is a disease prevention model with a primary focus on how belief and behavior go hand in hand. It assumes that showing preventive behaviors depends on people’s perceived risk of the disease, the effect of the disease on their life and the effect of healthy behaviors on less susceptibility to and severity of the disease [15]. HBM constructs can apply to HIV educational programs, and raise awareness of HIV preventive behaviors [16]. A body of research has proved the effectiveness of HBM-based educational interventions in preventing HIV in different populations [14, 17]. This model has six constituent parts including perceived susceptibility, severity, benefits, barriers, self-efficacy and cues for action [18].
Educational interventions have been previously used in relation to HIV. Yet, they mostly addressed populations other than prisoners, or they used other theories than the HBM [12]. Maintaining prisoners’ health protects a whole society. Thus, HIV preventive measures are essential in prisons to provide useful education and information [6]. The present research is pioneering in exploring the effect of an educational program based on the HBM on prisoners’ HIV preventive behaviors in the south of Iran. The present findings suggest useful strategies to implement educational interventions and promote HIV preventive behaviors to health policy-makers.
Methods
Design and population
The present research was quasi-experimental in type. There were two groups included, a control (CG) and an intervention group (IG). The research was done in 2019–20 with an educational program developed based on the HBM to promote HIV preventive behaviors in prisoners with 3–5 years’ imprisonment in the south of Iran. A 3-month follow-up was also included.
Setting
The present research was set in Roudan County in the south of Iran, with an area of about 3044.4 km2. Roudan is 100 km away from Bandar Abbas. Its capital city with the same name, Roudan, is located in 27°:27′ of the north and 57°:11′ of the east at an altitude of about 190 m above the sea level.
Eligibility criteria
The inclusion criteria were: at least 6 months’ time left until release from the prison, no chronic mental disease (according to the medical records) and informed consent to participate in the research.
Exclusion criteria
The exclusion criteria were failure to regularly attend the educational sessions (absence for more than 2 sessions), not to be available for the post-test, and incomplete questionnaires.
Sample size estimation
To estimate the sample size, the following formula was used:
In their study, Ebrahimipour et al. reported the standard deviation of self-efficacy in the intervention and control groups as 13.24 and 15.32, respectively [12]. They assumed α to be 0.05, β as 0.2 and μ1- μ2 as 5. Thus, they estimated a sample size of 130. With an attrition rate of 5–7%, the final sample size was decied to be 140.
Sampling
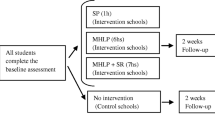
There are 4 modules (or pods) in Shahid Lajevardi Prison in Roudan. There are 1200 inmates overall (i.e., about 300 in each module). The 1st and 2nd modules, which were adjacent, were selected as the IG and the 3rd and 4th as the CG. There are certain educational and cultural activities routinely planned in this prison for inmates. Modules 1 and 2 receive the educational and cultural services on different days from the modules 3 and 4. Thus, we decided to include modules 1 and 2 together in one group and modules 3 and 4 in the other group. The list of inmates in all four modules was obtained from the authorities. The Excel software was used to select 70 subjects from each module through simple randomization. If a subject did not meet the inclusion criteria, he was replaced by another through simple randomization (Fig. 1). To ensure the minimal contamination effect, the IG and CG subjects were selected from different modules. Thus, the inmates had fewer chances of communicating with each other. The break time of the two groups was scheduled to be different from each other.

Flowchart for sample selection
Intervention procedure
The pretest was given to the CG and IG using the HBM questionnaire. According to the pretest results, an educational need analysis was done to decide on the educational materials, methods and number of sessions needed for education. The educational content of each session was decided on according to the learners’ comprehension, use of reliable scientific sources, experts’ commentaries as well as those of the participants within the HBM framework. Besides the target behaviors, the educational methods, number of sessions and duration of each session were specified in the material development process. Overall, 8 educational sessions were to be held for 2 months in 10–15 educational groups. Each session was 40 to 60 minutes long with a 10-minute break. The teaching modes were lecture, group discussions, brainstorming, concept mapping, movies, and photos. It is noteworthy that all subjects participated until the last session, and there was no attrition. The CG had a 1-hour educational session on HIV transmission and the significance of personal health in preventing the infection. Three months after the intervention, the posttest questionnaire was given to both groups to assess the effectiveness of the educational intervention.
The educational content included:
-
1.
general considerations about HIV and some facts and figures about the incidence rate,
-
2.
emphasis on the hazardous prison environment and how it affected HIV infection,
-
3.
prisoners’ awareness of the different ways of transmitting the disease and high-risk behaviors in prison,
-
4.
physical, mental and social benefits of no HIV infection,
-
5.
challenges of and barriers to HIV preventive behaviors, and increased self-efficacy.
The details of the educational sessions are summarized in Supplementary 1.
Data collection
The data were collected as self-reporting questionnaires. Having consented to take part in the study, the participants in each group received adequate information about the purpose of study and what they were expected to do. The pre-test questionnaires were provided to the IG and CG. Also, 3 months after the educational intervention, the post-test questionnaires were provided to both groups. For the participants who were illiterate, the questions were read out loud by one of the researchers to minimize the bias. A specific well-trained member of the research teach was assigned to this task. The answers were transcribed with no change or personal interpretation. The questionnaire completion took between 20 and 25 minutes.
Questionnaire content and scoring system
The questionnaire contained closed-ended questions rated on a Likert scale. There were two parts as introduced below.
Part I (demographic information)
Several variables were included in this part of the questionnaire. These included the participants’ age, level of education, marital status, job, history of imprisonment, history of drug abuse, the use of condoms in sex affairs, and sex partners.
Part II (HBM constructs)
The HBM constructs are summarized in Table 1. The content of the questionnaire is presented in Supplementary 2.
All items were rated on a 5-point Likert scale: strongly agree (1 point), agree (2 points), neutral (3 points), disagree (4 points), and strongly disagree (5 points). Each construct was assessed separately, and the total score was not calculated. The score for each construct was calculated for each participant. Higher scores represented stronger feelings about that construct. All constituent parts showed to be positively associated with the target behavior except for the perceived barriers which was negatively correlated.
Data quality assurance
The researcher-made instrument was developed in the light of the related literature, and the national plan to prevent and control HIV infection developed by the ministry of health and the deputy of health in the disease management center. Before the main data collection phase, the questionnaires were piloted on a group of 20 subjects similar to the main participants. Their comments were used to revise the content of the questionnaire and better organize the items. The content validity was also approved by a panel of experts. Then, the required qualitative and quantitative adaptations were made. The internal consistency of the instrument was approved using Cronbach’s alpha. To substantiate the reliability of the questionnaire, the test-retest method was used. To this aim, the questionnaire was submitted twice at a 2-week interval to 20 subjects who were similar to the main participants. The ICC was found to be 0.86, interpreted as high. Thus, the reliability of the questionnaire was confirmed.
Ethical considerations
The participants were supposed to sign an informed letter of consent. The confidentiality of the information they provided was ensured. All the required measures were taken to ensure the confidentiality of the participants’ information. The research procedures were fully explained. The results were also, later on, provided to them. Prisoners with mental diseases were more vulnerable. Their condition could affect their voluntary decisions. Thus, their decision whether to participate in the study or not was respected. Their decision did not affect the availability of facilities provided in prison, such as healthcare services or healthy food. If they did not consent to take part in the research, they were not treated adversely by the prisoners. Their participation was quite fair and respected. Before the study, the final draft of the questionnaire was reviewed by the prison authorities, and their comments were used to revise the instrument.
The study conformed to the world medical association (WMA) of Helinski and the Nuremberg Code. The project was approved by the ethics committee of Hormozgan University of medical sciences (#IR.HUMS.REC.1398.112).
Output
The output was an increase in perceived susceptibility, severity, benefits, self-efficacy and barriers.
Outcome
The expected outcome was the adoption of HIV preventive behaviors.
Data management and analysis
To analyze the quantitative variables (age and HBM scores), mean and standard deviation were used. To describe qualitative data, frequency and relative frequency were used. To test the assumptions of parametric tests such as the normality of distribution and equality of variance, Kolmogorov-Smirnov test and Levene’s test were run. Then, independent-samples T-test was used to compare HBM scores and the adoption of preventive behaviors in the two groups. Paired-samples T-test was run to compare the pretest and post-test results within each group. ANCOVA was used to control and adjust for the scores before and after the intervention. Besides, multiple linear regression analysis was run to assess the effect of each HBM construct on the behavior score. Healthy behavior was considered as the dependent variable and the model constructs as independent variables. All the analyses were done in SPSS20.
Results
Research population
The present quasi-experimental study was conducted on a total number of 280 prisoners (140 in the IG and 140 in the CG). The participants’ age ranged between 19 and 65 years with a mean and standard deviation of 35.49 ± 8.24 in the CG and 35.29 ± 8.82 in the IG. Concerning education, in both research groups, the most frequent education level was secondary school (39.3% in the IG and 40.03% in the CG). The majority of prisoners in both groups had 1–2-time experience of imprisonment (94.35% in the IG and 80% in the CG). The majority of prisoners had a history of drug addiction (57.9% in the IG and 67.1% in the CG). The other demographic variables are summarized in Table 2.
Between-group comparison of HBM constructs in the pretest and posttest
Before the intervention, the two groups showed no statistically significant difference in terms of the HBM scores (p > 0.05). However, after the educational intervention, the between-group difference was statistically significant (p < 0.001). In the IG, the behavior score was 22.93 ± 4.35 in the pretest, which was increased to 31.85 ± 0.739 in the posttest. This increase was statistically significant. However, in the CG, the behavior score did not change significantly from the pretest to posttest (Table 3).
Controlling the covariate effect of scores in the pretest
To control and adjust for the effect of pretest scores, ANCOVA was used. As summarized in Table 3, the pretest scores were found to be statistically significant covariates of perceived severity (partial η2 = 0.084; p = 0.001), perceived barriers (partial η2 = 0.036; p = 0.002), and behavior (partial η2 = 0.370; p < 0.001). But as the pretest scores and the ANCOVA result showed, perceived susceptibility (partial η2 = 0.001; p = 0.692), benefits (partial η2 = 0.001; p = 0.825) and self-efficacy (partial η2 = 0.001; p = 0.534) were not statistically significant.
Predictors of AIDS preventive behavior
To analyze the effect of each HBM construct on the adoption of healthy behavior, multiple linear regression analysis was used. How the dependent and independent variables behaved was different. As indicated in Table 4, perceived severity, susceptibility, benefits, self-efficacy and barriers were the best predictors of healthy preventive behavior. The adjusted R-square of 0.411 shows that the model managed to explain 41% of variation in behavior in the intervention group (Table 5).
Discussion
The present study explored the effect of an educational intervention on the adoption of HIV preventive behaviors based on the HBM model. Multivariate regression analysis (R2 = 0.411) showed that the independent variable in the model (HBM constructs) managed to explain 41% of variance in the dependent variable (i.e. adoption of HIV preventive behavior).
The present findings showed that the two groups did not diverge significantly in terms of perceived susceptibility before the intervention. However, after the educational intervention, the between-group difference was statistically significant. This finding was consistent with a body of research that showed the effectiveness of educational interventions in increasing the chances of HIV infection [14, 17, 19]. However, a number of studies reported the failure of educational interventions at increasing participants’ susceptibility of HIV and medical adherence in HIV patients [20,21,22]. This divergence can be partly due to the differing demographic features of the research populations. In the abovementioned studies, the research population was female adolescents, often at a lower risk of high-risk behaviors such as sexual behaviors and drug injection than the target population in this research. Further divergences can be the duration, content and teaching methods used in the intervention, which were more limited in the aforementioned studies than the present study. It is noteworthy that perceived susceptibility showed to affect prisoners’ promotion of healthy behavior. Arguably, the theory-based education managed to increase prisoners’ susceptibility to the infection. Researchers believe that, to motivate a certain healthy behavior, people need to get aware of the potential adverse effects of a disease or how it affects their awareness [23].
The present findings showed that the mean score of perceived severity was increased in the IG. Similarly, a body of research showed that educational interventions managed to increase the mean score of perceived severity in [14, 16, 19, 24]. Moreover, our findings showed that perceived severity was the strongest predictor of adopting HIV-AIDS preventive behaviors. This is in contrast to some other research which showed no effect of perceived severity on the adoption of healthy behavior [24]. It can be argued that the severely adverse effects of HIV infection are adequately perceived by the prisoners. Thus, prisoners are motivated enough to show HIV preventive behaviors. Presumably, prisoners with a better perceived severity of the adverse effects of HIV show more protective behaviors. According to Rosen Stock’s theory, perceived severity can promote preventive and medical measures in individuals [25]. As put forth by Bakhtiari, one who perceives him/herself at the risk of a major problem, takes a serious measure to protect oneself [26].
The present findings showed that the mean score of perceived benefits was significantly increased in the IG compared to the CG. Similarly, a body of research reported the effectiveness of education in increasing the perceived benefits of HIV preventive behaviors [14, 16, 27] . Contrary to the present findings, in a number of studies, perceived benefits was not correlated with HIV preventive behaviors [22, 28] . Different purposes of research and socio-demographic features in different geographies can be other potential reasons for the different findings. As an instance, in the study conducted by Gharlipour et al., probably failed HIV therapeutic measures canceled out the effect of the educational intervention on the participants’ perceived benefits. Our educational intervention, however, evidently highlighted the benefits of preventing HIV and managed to encourage people to adopt preventive healthy behaviors.
We also found that the educational intervention had no effect on perceived barriers. This is consistent with a number of studies that reported the ineffectiveness of educational interventions in HIV preventive behaviors and adherence to medications [14, 22]. Contrary to this finding, some other studies found an increase in perceived barriers after the educational intervention [20, 27, 29]. Different types of barriers in different studies (physical, financial, psychological and social) can also account for the divergent findings. No increase in the perceived barriers score in the present study was quite expected because, as also reflected in the questionnaire items, most barriers were out of an individual’s control. Naturally, in only one educational intervention, we were unable to overcome such personal barriers that required higher-order interventions such as organizational, social and even political. Of note is that in this research, a lower perceived barrier score was accompanied by a higher rate of healthy behaviors. Thus, it can be expected to be effective in the adoption of healthy behavior.
The present findings also revealed a higher mean score of self-efficacy in the IG than CG in the posttest. This is consistent with a number of studies which also reported an increase in the self-efficacy score after the educational intervention [14, 27]. Another study showed that self-efficacy was significantly and strongly correlated with HIV preventive behaviors in Thai youngsters [12]. Furthermore, self-efficacy has proved to be key to the reduced rate of high-risk AIDS-related behaviors [30]. In contrast, in two other works of research by Smith and Bandora [31]. and Zamboni [32]., education showed to have no effect on patients’ self-efficacy [22]. Improving self-efficacy was suggested as a secondary goal for lowering the rate of HIV infection. According to the socio-cognitive theory, those with a lower self-efficacy stand higher chances of showing risky behaviors [27]. As expected in our research, those with a higher self-efficacy showed more HIV-AIDS preventive behaviors [28]. Thus, improving prisoners’ self-efficacy can to a large extent prevent the incidence rate of HIV.
The present findings showed an increase in the participants’ score of HIV preventive behaviors in IG compared to CG after the intervention. Similarly, other studies reported the effectiveness of adopting HIV preventive behaviors and adherence to medications [16, 22] . It can be argued that the educational intervention could have positively affected the participants’ healthy behavior by affecting the HBM constructs as the mediating factors.
Limitations, strengths and suggestions for future research
The present research was conducted on male prisoners in the south of Iran; thus, the generalization of the findings to other populations especially women is limited. To increase the generalizability, future research needs to include comparable male and female samples in areas with different cultural and socioeconomic features. The short-term follow-up was another limitation. Therefore, it is suggested that the participants be followed up for at least a year to assess their consistency of behavior. Another limitation of this research was the self-reporting nature of the questionnaire. The participants might have produced socially desirable responses which can threaten the integrity of responses. Still, we attempted to ensure the subjects of the confidentiality of the information they provided to maximize their honesty. The data were collected anonymously to reduce the biased responses. A lack of access to confidential prison information, including the number of HIV-infected inmates and drug abuse in prisons, were among the other limitations of the present study.
There were certain strengths as well. For instance, the theory employed (i.e., the HBM) was a systematic framework to explain the healthy preventive behavior. This theory clearly described the key concepts included in the intervention [33]. Making a goal-oriented and theory-based intervention, selecting a high-risk research population and having a control group are among the other strengths of the present research.
Implications
As there is no definite cure for HIV infection and there has been no theory-based educational intervention for the target research population (i.e., prisoners), the present findings can significantly contribute to the existing literature. They pave the way for future comparative HIV-related research and can help policy makers develop better interventional programs to prevent HIV-related risky behaviors in the light of relevant theories.
Conclusion
The present research showed the effectiveness of HBM in adopting HIV preventive behaviors among prisoners. The educational intervention managed to positively affect the prisoners’ healthy behaviors by affecting the HBM constructs first. As the results showed, the educational intervention had no effect on perceived barriers, which was quite expected, as perceived barriers could not be removed until the end of a simple short-term intervention. To remove barriers to the adoption of healthy behaviors, researchers should develop multi-level interventions to gain more desirable outcomes. We particularly aim to implement goal-oriented educational programs based on health education and promotion frameworks to prevent HIV behaviors.
Availability of data and materials
The datasets used and/or analyzed during the study are available from the corresponding author on reasonable request.
Abbreviations
- HBM:
-
Health belief model
- IG:
-
Intervention group
- CG:
-
Control group
References
The Global HIV Epidemic https://www.kff.org/global-health-policy/fact-sheet/the-global-hivaids-epidemic.
SeyedAlinaghi S, Leila T, Mazaheri-Tehrani E, Ahsani-Nasab S, Abedinzadeh N, McFarland W, et al. HIV in Iran: onset, responses and future directions. AIDS (London, England). 2021;35(4):529.
Gharaei HA, Fararouei M, Mirzazadeh A, Sharifnia G, Rohani-Rasaf M, Bastam D, et al. The global and regional prevalence of hepatitis C and B co-infections among prisoners living with HIV: a systematic review and meta-analysis. Infect Dis Poverty. 2021;10(1):1–17.
Defante Ferreto LE, Guedes S, Braz Pauli F, Soligo Rovani S, Aní Caovilla Follador F, Paula Vieira A, et al. Seroprevalence and associated factors of HIV and hepatitis C in Brazilian high-security prisons: a state-wide epidemiological study. Plos One. 2021;16(7):e0255173.
Seyedalinaghi SA, Farhoudi B, Mohraz M, Firouzeh MM, Hosseini M, Kamali K. Prevalence of HIV in a prison of Tehran by active case finding. Iran J Public Health. 2017;46(3):431–2.
Sayyah M, Rahim F, Kayedani GA, Shirbandi K, Saki-Malehi A. Global view of HIV prevalence in prisons: a systematic review and meta-analysis. Iran J Public Health. 2019;48(2):217.
Akbari M, Akbari M, Naghibzadeh-Tahami A, Joulaei H, Nasiriyan M, Hesampour M, et al. Prevalence of HIV/AIDS among Iranian prisoners: a review article. Addict Health. 2016;8(3):195.
Golsoorat F, Pahlaviani M. Prevalence and associated factors of HIV infection among male prisoners in Tehran, Iran. Arch Iran Med. 2017;20(6):356.
Navadeh S, Mirzazadeh A, Gouya MM, Farnia M, Alasvand R, Haghdoost A-A. HIV prevalence and related risk behaviours among prisoners in Iran: results of the national biobehavioural survey, 2009. Sex Transm Infect. 2013;89(Suppl 3):iii33–6.
Eshrati B, Asl RT, Dell CA, Afshar P, Millson PM, Kamali M, et al. Preventing HIV transmission among Iranian prisoners: initial support for providing education on the benefits of harm reduction practices. Harm Reduct J. 2008;5(1):1–7.
Shahbazi M, Farnia M, Rahmani K, Moradi G. Trend of HIV/AIDS prevalence and related interventions administered in prisons of Iran-13 years’ experience. Iran J Public Health. 2014;43(4):471.
HIV in prisons https://www.euro.who.int/en/health-topics/communicable-diseases/hivaids/policy/policy-guidance-for-key-populations-most-at-risk2/hiv-in-prisons.
Organization WH. Effectiveness of interventions to address HIV in prisons. Geneva: World Health Organization; 2007. p. 5–124.
Khazaeian S, Kariman N, Ebadi A, Nasiri M. Effect of an educational intervention on AIDS prevention among the female heads of household: application of the health belief model. Shiraz E Med J. 2019;20(4):e80892. https://doi.org/10.5812/semj.80892.
Anuar H, Shah S, Gafor H, Mahmood M, Ghazi HF. Usage of health belief model (HBM) in health behavior: a systematic review. Malays J Med Health Sci. 2020;16(11):2636–9346.
Karimy M, Ghofranipor F, Heidarnia A. The effect of health education based on health belief modelon preventive actio of aids on addict in zarandieh. J Guilan Univ Med Sci. 2009;18(70):64–73.
Jeihooni AK, Arameshfard S, Hatami M, Mansourian M, Kashfi SH, Rastegarimehr B, et al. The effect of educational program based on health belief model about HIV/AIDS among high school students. Int J Pediatr Mashhad. 2018;6(3):7285–96.
Dadipoor S, Ranaei V, Ghaffari M, Rakhshanderou S, Safari-Moradabadi A. Safe driving behaviors among taxi drivers: a predictive cross-sectional study based on the health belief model. Arch Public Health. 2020;78(1):1–6.
Khazaeian S, Navidian A, Sanavi FS, Hadipoor L. Investigating the effect of education on man immunodeficiency virus/acquired immune deficiency syndrome preventive behaviors in vulnerable women living in peripheral neighborhoods: applications of the health belief model. J Educ Health Promot. 2020;9:302. https://doi.org/10.4103/jehp.jehp_325_20.
Pirzadeh A, GhR S. Effect of educational program on knowledge and health belief model structures about acquired immune deficiency syndrome (AIDS) among high school female student in Isfahan, Iran. J Gorgan Univ Med Sci. 2012;14(3):66–71.
Kharazi SS, Peyman N. Effect Of educational interventions based on the health belief model on the promotion of aids preventive behaviors among female high school students in Mashhad, Iran, In 2016. Health Syst Res. 2017;13(1):14–18.
Gharlipour Z, Mohebi S, Sharifirad G, Yadegari J. Effect of educational intervention based on the expanded health belief model on antiretroviral therapy adherence in the patients with AIDS. J Hum Environ Health Promot. 2018;4(2):64–70.
Karimy M, Azarpira H, Araban M. Using health belief model constructs to examine differences in adherence to pap test recommendations among Iranian women. Asian Pac J Cancer Prev. 2017;18(5):1389.
Montanaro EA, Bryan AD. Comparing theory-based condom interventions: health belief model versus theory of planned behavior. Health Psychol. 2014;33(10):1251.
Rosenstock IM. Historical origins of the health belief model. Health Educ Monogr. 1974;2(4):328–35.
Bakhtari Aqdam F, Nuri Zadeh R, Sahebi L. Effect of education based on health belief model on believe promotion and screening behaviours of breast cancer among women reffered to Tabriz health centers. Medl J Tabriz Uni Medl Sci. 2012;2012(33):25–31.
Bastami F, Mostafavi F, Hassanzadeh A. Effect of educational intervention on knowledge, perceived benefits, barriers and self-efficacy regarding AIDS preventive behaviors among drug addicts. J Edu Health Promot. 2015;4:90.
Khumsaen N, Stephenson R. Beliefs and perception about HIV/AIDS, self-efficacy, and HIV sexual risk behaviors among young Thai men who have sex with men. AIDS Educ Prev. 2017;29(2):175–90.
Hounton SH, Carabin H, Henderson NJ. Towards an understanding of barriers to condom use in rural Benin using the health belief model: a cross sectional survey. BMC Public Health. 2005;5(1):1–8.
Bandura A. Perceived self-efficacy in the exercise of control over AIDS infection. Eval Program Plann. 1990;13(1):9–17.
Smith KW, McGraw SA, Costa LA, McKinley JB. A self-efficacy scale for HIV risk behaviors: development and evaluation. AIDS Educ Prev. 1996;8(2):97–105.
Zamboni BD, Crawford I, Williams PG. Examining communication and assertiveness as predictors of condom use: implications for HIV prevention. AIDS Educ Prev. 2000;12(6):492.
Grandahl M, Rosenblad A, Stenhammar C, Tydén T, Westerling R, Larsson M, et al. School-based intervention for the prevention of HPV among adolescents: a cluster randomised controlled study. BMJ Open. 2016;6(1):e009875.
Acknowledgements
The authors would like to thank Hormozgan University of medical science for their financial support. The authors would also like to express gratitude to the participants for their sincere cooperation.
Funding
This research received a grant from Hormozgan University of medical science.
Author information
Authors and Affiliations
Contributions
Z.H designed the study, supervised data collection, analyzed the data and reviewed the manuscript; S.D. designed the study, collected data, analyzed the data, drafted the manuscript and critically reviewed the manuscript; P. N designed the study and reviewed the manuscript; SH. M analyzed the data and reviewed the manuscript; T.A., S.D., Z.H. reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study conformed with the WMA of Helinski and the Nuremberg Code. It was also approved by the Ethics Committee of Hormozgan University of medical sciences (#IR.HUMS.REC.1398.112). All participants provided written informed consent before entering the study.
Consent for publication
Not applicable.
Competing interests
None to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Education and training content.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hosseini, Z., Najafi, P., Mohseni, S. et al. The effect of a theory-based educational program on southern Iranian prisoners’ HIV preventive behaviors: a quasi-experimental research. BMC Public Health 22, 1342 (2022). https://doi.org/10.1186/s12889-022-13763-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-13763-z