
Abstract
We tend to investigate the connection between time to appropriate therapy (TTAT) and prognosis in pediatric patients with nosocomial Klebsiella pneumoniae (K. pneumoniae) bloodstream infection, and find the optimal cutoff point for the empirical administration of antimicrobials. This retrospective study was conducted in Children’s Hospital of Chongqing Medical University, and inpatients with nosocomial K. pneumoniae bloodstream infection were finally enrolled. We applied the Classification and Regression Tree (CART) analysis to find the TTAT cutoff point and the Logistic Regression analysis to evaluate prognostic indicators. The incidence of septic shock and mortality was 17.91% (12/67) and 13.43% (9/67), respectively. The CART-derived TTAT cutoff point was 10.7 h. The multivariate logistic regression analysis indicated delayed therapy (TTAT ≥ 10.7 h), pediatric risk of mortality (PRISM) III scores ≥ 10, time to positivity (TTP) ≤ 13 h, and requiring for invasive mechanical ventilation were independently associated with the incidence of septic shock (Odds ratio [OR] 9.87, 95% Confidence interval [CI] 1.46–66.59, P = 0.019; OR 9.69, 95% CI 1.15–81.39, P = 0.036; OR 8.28, 95% CI 1.37–50.10, P = 0.021; OR 6.52, 95% CI 1.08–39.51, P = 0.042; respectively) and in-hospital mortality (OR 22.19, 95% CI 1.25–393.94, P = 0.035; OR 40.06, 95% CI 2.32–691.35, P = 0.011; OR 22.60, 95% CI 1.78–287.27, P = 0.016; OR 12.21, 95% CI 1.06–140.67, P = 0.045; respectively).
Conclusions TTAT is an independent predictor of poor outcomes in children with nosocomial K. pneumoniae bloodstream infection. Initial appropriate antimicrobial therapy should be administrated timely and within 10.7 h from the onset of bloodstream infection is recommended.
Similar content being viewed by others


Introduction
Klebsiella pneumoniae (K. pneumoniae) is the most common antimicrobial-resistant gram-negative pathogens in nosocomial bloodstream infection, causing high economic burden [1]. Timely antimicrobial therapy is critical to the prognosis in patients with bloodstream infection [2]. According to the 2021 Surviving Sepsis Campaign [3], antimicrobials are recommended as soon as possible for sepsis patients (≤ 3 h for patients without shock, ≤ 1 h for patients with suspicious septic shock). The 1-h and 3-h goals are strongly recommended, while with low quality of evidence and remains controversial [3, 4]. Meanwhile, our previous study showed that the delayed appropriate antimicrobial therapy ≥ 13.6 h, not ≥ 1 or 3 h, was associated with the highest sepsis-related mortality in children with Streptococcus pneumoniae sepsis [5]. Furthermore, 1-h or 3-h goal sometimes is unrealistic to be achieved due to limitations in early recognition or diagnosis of sepsis [4]. In some ways, immediate antimicrobial treatment is lifesaving. However, overdiagnosis of sepsis and premature administration of antimicrobials may result in overtreatment and antimicrobial-associated harms [6, 7]. The Infectious Diseases Society of America states the administration time of antimicrobials vary with different pathogens and populations [8]. In adult patients, the optimal appropriate antimicrobial therapy time windows were 24 h for K. pneumoniae bloodstream infection [9], 48.1 h for Enterococci bloodstream infection [10], 52 h for Pseudomonas aeruginosa bloodstream infection [11] and 44.75 h for Staphylococcus aureus bacteremia [12]. Bacteremia patients with different pathogens could have different appropriate antimicrobial time windows and this remains unclear in pediatric patients with K. pneumoniae bloodstream. Therefore, the optimal antimicrobials administration time windows in different populations need to be explored. We tend to prove the prognostic value of time to appropriate therapy (TTAT) in children with nosocomial K. pneumoniae bloodstream infection, and to find an optimal time point for the appropriate antimicrobials administration.
Methods
Study designs and patients
This retrospective, observational cohort study was conducted in Children’s Hospital of Chongqing Medical University, National Clinical Research Center for Child Health and Disorder, ranked the top two children’s hospitals in China (rank list: http://top100.imicams.ac.cn/home). Patients diagnosed with K. pneumoniae bloodstream infection were enrolled. Inclusion was marked as follows: (i) inpatients, (ii) 1 month ≤ age ≤ 18 years, (iii) with monomicrobial K. pneumoniae bloodstream infection. The exclusion criteria were as the following: (i) patients diagnosed with community-acquired K. pneumoniae bloodstream infection, (ii) patients with incomplete clinical information and (iii) patients received appropriate antimicrobials against K. pneumoniae prior to blood culture. This is a retrospective study so that informed consent was exempted.
Data collection and definitions
We retrospectively gathered the basic information (eg. Sex, weight and so on), underlying conditions, axillary temperature, sources of infection, microbiological and laboratory data, treatment and outcomes. Nosocomial infection was the infections occurred > 48 h after admission [13]. K. pneumoniae isolated from blood culture associate with related clinical manifestations of infection was diagnosed as K. pneumoniae bloodstream infection [13]. Patients with immunosuppression were characterized as patients with immunodeficiency diseases, or patients received chemotherapy or immunosuppressive steroid therapy more than 14 days [5]. Hypoalbuminemia was defined as intravascular albumin level < 2.5 g/dL for children younger than 7 months and < 3.4 g/dL for children 7 months or older [14]. Source of infection was defined according to the CDC /NHSN surveillance guidelines [15]. Disease severity of patients in different subgroups were compared by using the Pediatric Risk of Mortality (PRISM) III score [16]. Time to positivity (TTP) was characterized as the time interval from the start of incubation to the alert of bacterial growth [17]. Our previous study, for children with K. pneumoniae bloodstream infection, showed that TTP ≤ 13 h and a PRISM III score ≥ 10 were related to poor outcomes [18]. Empiric antimicrobial treatment was characterized as antimicrobials initially administrated without in vitro sensitivity test results [19]. Appropriate antimicrobial therapy was defined as patients received at least one intravenous antimicrobials documented in vitro susceptibility basing on the breakpoint established according to the Clinical and Laboratory Standards Institute (CLSI) guideline [20]. Multi-drug resistant (MDR) was defined as bacteria with resistance to 3 or more antimicrobials classes [21]. TTAT was defined as the time span between onset of bloodstream infection and the first dose of appropriate antimicrobials [9]. The onset of bloodstream infection was identified by no less than two senior infectious disease physicians according to clinical manifestations (e. g. fever, chill and so on) and biomarkers (e. g. C-reactive protein, procalcitonin and so on), and approved by the subsequent positive blood culture result. Sepsis and septic shock were diagnosed basing on the Sepsis-3.0 [22].
Clinical outcomes
The primary outcome was in-hospital mortality, the second outcome was incidence of septic shock.
Statistical analysis
Classification and regression tree (CART) analysis [23] was used to find the optimal cutoff point of TTAT and the area under the receiver operating characteristic (ROC) curve [24] was used to examine the prognostic value of the TTAT cutoff point. Kaplan–Meier survival analysis were used to compare the incidences of septic shock and mortality between early and delayed therapy groups which grouped according to the TTAT cutoff point. In-hospital mortality of different delay time spans to appropriate antimicrobials therapy were assessed by using linear χ2 test. In groups comparing, we applied the Manne-Whitney U test or the Student’s t test for inferential statistics of continuous data, and the Pearson χ2 test or the Fisher’s exact test for categorical variables. Logistic regression test was applied to find independent risk factors of poor outcomes. All variables were analyzed in multivariate analysis except for those with P-level ≥ 0.10 in univariate analysis, by using forward likelihood ratio selection. Odds ratio (OR) and the corresponding 95% confidence interval (CI) were calculated. All statistical analyses were conducted by SPSS software 23.0 for Windows. The level of significance was set at P-value < 0.05 (two-sided).
Results
Study population
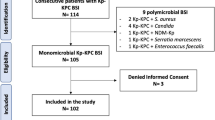
One hundred and thirty-two patients were retrospectively enrolled at the beginning. There were sixty-five patients were excluded: sixty cases were classified as community-acquired infection, three cases with incomplete clinical information, and two cases received effective antimicrobials against K. pneumoniae isolates prior to blood culture. Finally, sixty-seven cases were enrolled in this study (Fig. 1).

Flow diagram of the population
Clinical characteristic of K. pneumoniae bloodstream infection in children
The median age was 4.33 (Inter-quartile range [IQR] 0.76–10.67) years, and the male accounted for 61.69% (42/67). More than half of the patients had hematologic malignancy or immunosuppression (44/67, 65.67%; 41/67, 61.19%, respectively). The most common source of bloodstream infections originated from respiratory tract (55.22%), followed by gastrointestinal tract (20.90%) and unknown source (14.93%). There were 32 (47.76%) extended-spectrum beta-lactamase (ESBL) positive and 6 (8.96%) multidrug resistant (MDR) K. pneumoniae isolates. More than half of the K. pneumoniae isolates resistant to sulbactam (40/67, 59.70%). The resistant rates of cephalosporin and tazobactam were 22.39% (15/67) and 20.90% (14/67), respectively. There were 28 (41.79%) patients received antimicrobial therapy prior to blood culture. Furthermore, thirty-eight (56.72%) patients were treated with carbapenems empirically before the susceptibility tests. The median TTP and TTAT was 14.12 (IQR 12.72–16.22) hours and 4.52 (IQR 0.97–14.18) hours, respectively. Twenty-two (32.84%) patients with secondary hypoalbuminemia and eleven (16.42%) patients administered with invasive mechanical ventilation during hospitalization. The median length of stay before the onset of bloodstream infection was13.68 (IQR 6.59–17.53) days, the median length of whole hospitalization stay was 28.96 (IQR 20.04–42.75) days. Septic shock occurred in 17.91% (12/67) of patients. The in-hospital mortality was 13.43% (9/67). The detailed characteristics of those patients are presented in Table 1.
TTAT of K. pneumoniae bloodstream infection in children
The TTAT cutoff point derived by CART to delineate the risk of in-hospital mortality was 10.7 h. Patients were classified into early (TTAT < 10.7 h) and delayed therapy group (TTAT ≥ 10.7 h) according to TTAT cutoff point. Twenty-three (34.33%) patients received delayed therapy. Patients received delayed therapy had remarkably higher in-hospital mortality than those received early therapy (29.17% vs 4.65%, P = 0.028). In patients with TTAT < 10.7 h, higher proportions of PRISM III scores ≥ 10 and TTP ≤ 13 h still significantly indicated higher in-hospital mortality (P < 0.01) (Fig. 2). The TTAT cutoff point derived from CART was demonstrated with a good prognostic value in ROC curve analysis (Area under the curve [95% confidence interval (CI)], 0.721 [0.564–0.879], 77.78% sensitivity and 70.69% specificity), with moderate predictive efficacy [24]. Figure 3 showed the Kaplan–Meier survival curve of those patients. In χ2 test for a linear trend, patients in TTAT ≥ 10.7 h group had the highest in-hospital mortality when compared to those in TTAT < 3 h and 3 h ≤ TTAT < 10.7 h periods groups. (P = 0.008) (Fig. 4).

Classification and regression tree analysis of predictors of in-hospital mortality in children with K. pneumoniae bloodstream infection

The comparison of patients in different TTAT groups according to in-hospital mortality (a) and septic shock (b)

In-hospital mortality stratified by the length of delay in receiving appropriate therapy. *, P level for χ2 test for linear trend
Clinical characteristics differences between the early and delayed therapy groups
Table 2 showed the characteristic differences of patients in different TTAT group. When compared with the delayed therapy (TTAT ≥ 10.7 h) group, more patients in early therapy (TTAT < 10.7 h) group had hematologic malignancy (84.09% vs 30.43%, P < 0.001) and immunosuppression (72.73% vs 39.13%, P = 0.007). Portion of patients who administrated with carbapenem empirically before the susceptibility tests in early therapy group were prominently higher than that in delayed therapy group (68.18% vs 34.78%, P = 0.009). Meanwhile, patients received delayed therapy may attribute to the notably higher proportion of empirical third-generation cephalosporin therapy (26.09% vs 4.55%, P = 0.029) and cephalosporin resistant isolates (39.13% vs 13.64%, P = 0.017) than those received early therapy. Accordingly, patients received delayed therapy had significantly higher incidence of secondary hypoalbuminemia (56.52% vs 20.45%, P = 0.002) and septic shock (39.13% vs 6.82%, P = 0.003), higher proportion of requiring invasive mechanical ventilation (34.78% vs 6.82%, P = 0.010), higher in-hospital mortality (30.43% vs 4.55%, P = 0.010) than those early therapy patients. While, the early and delayed therapy groups had no differences with the PRISM III scores, the length of stay before the onset of bloodstream infection and length of the whole hospitalization stay.
Comparisons of clinical characteristics between the survival and non-survival groups
Table 3 compared the clinical characteristics of the survival and non-survival patients. Patients in non-survival group had significantly higher proportions of cephalosporin resistant and extended spectrum beta-lactamase (ESBL) positive isolates, PRISM III scores ≥ 10, TTP ≤ 13 h and TTAT ≥ 10.7 h, higher incidence of requiring invasive mechanical ventilation and septic shock when compared to those in survival group. (P < 0.05). The whole hospitalization days and hospitalization days before the onset of bloodstream infection were not prominently associated with outcomes.
Risk factors of in-hospital mortality
Risk factors of in-hospital mortality were examined by logistic regression analysis. All results were shown in Table 4. Univariate analysis demonstrated that there was positive correlation between in-hospital mortality and the portion of patients with PRISM III scores ≥ 10. So as the patients with early TTP (TTP ≤ 13 h), delayed therapy (TTAT ≥ 10.7 h), requiring for invasive mechanical ventilation, with secondary hypoalbuminemia during hospitalization, ESBL positive isolates, and cephalosporin resistant isolates. According to the multivariate analysis, PRISM III scores ≥ 10 (OR 40.06, 95% CI 2.32–691.35, P = 0.011), early TTP (OR 22.60, 95% CI 1.78–287.27, P = 0.016), delayed therapy (OR 22.19, 95% CI 1.25–393.94, P = 0.035), and need for invasive mechanical ventilation (OR 12.21, 95% CI 1.06–140.67, P = 0.045) were independent risk factors of in-hospital mortality.
Risk factors of septic shock
Table 5 showed the logistic regression analysis of risk factors of septic shock. In univariate analysis, patients with PRISM III scores ≥ 10, early TTP (TTP ≤ 13 h), delayed therapy (TTAT ≥ 10.7 h), requiring for invasive mechanical ventilation, with ESBL positive isolates and secondary hypoalbuminemia after admission were remarkably associated with the incidence of septic shock. Multivariate analysis demonstrated that delayed therapy (OR 9.87, 95% CI 1.46–66.59, P = 0.019), PRISM III scores ≥ 10 (OR 9.69, 95% CI 1.15–81.39, P = 0.036), early TTP (OR 8.28, 95% CI 1.37–50.10, P = 0.021) and need for invasive mechanical ventilation (OR 6.52, 95% CI 1.08–39.51, P = 0.042) were independent risk factors of septic shock.
Discussion
In this study, we demonstrated that patients with PRISM III scores ≥ 10, TTP ≤ 13 h, requiring for invasive mechanical ventilation were independently associated with poor outcomes, which were consistent with our previous study [18]. Furthermore, we also showed that delayed therapy (TTAT ≥ 10.7 h) may predict higher incidence of septic shock or in-hospital mortality, which was similar to previous studies indicating delayed appropriate antimicrobial therapy was correlated to poor outcomes [2]. Falcone et al. [9] indicated that appropriate antimicrobial therapy should begin within 24 h from the collection of blood culture in adult carbapenemase-producing K. pneumoniae bloodstream infection patients. In this study, we found TTAT ≥ 10.7 h increased 22.19-fold risk of in-hospital mortality and 9.87-fold risk of septic shock in nosocomial K. pneumoniae bloodstream infection children. The differences of TTAT thresholds between us and Falcone et al. [9] may be as follows. First, we used different definition of the start point of TTAT. It is more accurate to define the start point of TTAT as onset of bloodstream infection. Obtaining the accurate TTAT for community-acquired infection patients seems to be unrealistic, whereas it`s feasible to gain the information of onset of bloodstream infection and accurate TTAT for nosocomial infection patients. Second, we used CART analysis to find the optimal TTAT cutoff point (10.7 h), and linear χ2 test and ROC curve analysis and were also applied to demonstrated it. However, Falcone et al. [9] didn’t explore the optimal TTAT cutoff point. Third, although we both enrolled patients with K. pneumoniae bloodstream infection, we concerned patients in different age groups. Two studies [6, 25] stated that TTAT > 3 h indicated higher mortality. Nevertheless, our TTAT was much longer. The explanations may as the following. First, patients with septic shock should administrate appropriate antimicrobials more aggressively than those with sepsis-associated organ dysfunction but without shock [19]. There were 17.91% (12/67) patients with septic shock in our study. While, there were 78.13% (125/160) and 79.23% (103/130) patients with septic shock in Han’s [6] study and Weiss’s [25] study, respectively. The lower proportion of septic shock patients in our study may explain the longer TTAT cutoff point. Second, the methods of defining TTAT cutoff points were different. We used the CART analysis while the other two studies used multivariate analysis.
We found that the secondary hypoalbuminemia during hospitalization may be associated with delayed appropriate antimicrobial therapy. Untimely antimicrobial therapy could lead to persistent bloodstream infection, which leads to increased breakdown and loss of albumin [26]. Low albumin levels may indicate severe condition and poor outcomes [26]. Moreover, this study showed patients received delayed therapy were with significantly higher proportion of empiric third-generation cephalosporin administration before blood culture than those received early therapy. The explanation may as the following. The third-generation cephalosporin is one of the most recommended empiric antimicrobial therapies in nosocomial infections [27]. However, with increased of third-generation resistant K. pneumoniae isolates [1], empirical third-generation cephalosporin administration may result in delayed appropriate antimicrobial therapy. K. pneumoniae is the most common antimicrobial resistant bacteria [1], and the nosocomial gram-negative bacteria bloodstream infection patients had higher proportion of inappropriate antimicrobial therapy [28]. Therefore, it is very important for clinicians to evaluate whether the empiric antimicrobial therapy is appropriate or not. More than half (38/67, 56.72%) of patients in our study empirically administrated with carbapenem. And the prevalence of carbapenem-resistant K. pneumoniae in this study (7/67, 10.45%) was higher than that reported in the European Centre for Disease Prevention and Control (website: http://atlas.ecdc.europa.eu/public/index.aspx?Instance=GeneralAtlas). We consumed that frequently using carbapenem may contribute to carbapenem-resistant K. pneumoniae isolate.
Appropriate antimicrobial therapy can improve the clinical outcomes in children with severe bloodstream infection. However, to avoid overtreatment, early recognition of the bloodstream infection and the pathogen is a new challenge to clinicians. In high-income countries, some rapid diagnostic testing technologies can help the clinician to identify K. pneumoniae quickly. However, in some low-income countries, the clinical experiences and education level of recognizing K. pneumoniae bloodstream infection may be more important. Furthermore, building susceptibility databases of K. pneumoniae isolates may help guiding clinicians to choose more appropriate and timely empiric antimicrobial therapy.
This study has some limitations. Firstly, this is a single-center retrospective study, and the sample is relatively small, so that more studies are expected to strength our results. Secondly, we only enrolled patients with nosocomial K. pneumoniae bloodstream infection, and this may influence the extrapolation of our data to other populations. Thirdly, when applied our results to clinical practice, we should pay attention to the difference of definitions of the start point of TTAT between us and other studies.
Conclusions
TTAT could be a prognostic factor in children with nosocomial K. pneumoniae bloodstream infection and the timely antimicrobial therapy can improve prognosis. The clinicians should initiate appropriate antimicrobials within 10.7 h of the onset of the K. pneumoniae bloodstream infection.
Availability of data and materials
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Abbreviations
- CART:
-
Classification and Regression Tree
- CI:
-
Confidence interval
- CLSI:
-
The Clinical and Laboratory Standards Institute
- ESBLs:
-
Extended spectrum beta-lactamases
- IQR :
-
Inter-quartile range
- MDR:
-
Multi-drug resistant
- OR:
-
Odds ratio
- PRISM:
-
Pediatric risk of mortality
- ROC:
-
The receiver operating characteristic
- TTAT :
-
Time to appropriate therapy
- TTP:
-
Time to positivity
References
Wyres KL, Lam MMC, Holt KE. Population genomics of Klebsiella pneumoniae. Nat Rev Microbiol. 2020;18(6):344–59. https://doi.org/10.1038/s41579-019-0315-1.
Liu VX, Fielding-Singh V, Greene JD, Baker JM, Iwashyna TJ, Bhattacharya J, Escobar GJ. The Timing of Early Antibiotics and Hospital Mortality in Sepsis. Am J Respir Crit Care Med. 2017;196(7):856–63. https://doi.org/10.1164/rccm.201609-1848OC.
Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, . . . Levy M. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–247. https://doi.org/10.1007/s00134-021-06506-y.
Filbin MR, Thorsen JE, Zachary TM, Lynch JC, Matsushima M, Belsky JB, . . . Reisner AT. Antibiotic Delays and Feasibility of a 1-Hour-From-Triage Antibiotic Requirement: Analysis of an Emergency Department Sepsis Quality Improvement Database. Ann Emerg Med. 2020;75(1):93–9. https://doi.org/10.1016/j.annemergmed.2019.07.017.
Li Q, Cheng J, Wu Y, Wang Z, Luo S, Li Y, . . . Luo Z. Effects of Delayed Antibiotic Therapy on Outcomes in Children with Streptococcus pneumoniae Sepsis. Antimicrob Agents Chemother. 2019;63(9):e00623-19. https://doi.org/10.1128/aac.00623-19.
Han M, Fitzgerald JC, Balamuth F, Keele L, Alpern ER, Lavelle J, . . . Weiss SL. Association of Delayed Antimicrobial Therapy with One-Year Mortality in Pediatric Sepsis. Shock. 2017;48(1):29–35. https://doi.org/10.1097/shk.0000000000000833.
Weinberger J, Rhee C, Klompas M. A critical analysis of the literature on time-to-antibiotics in suspected sepsis. J Infect Dis. 2020;222(Supplement_2):S110-s118. https://doi.org/10.1093/infdis/jiaa146.
Kollef MH, Shorr AF, Bassetti M, Timsit JF, Micek ST, Michelson AP, Garnacho-Montero J. Timing of antibiotic therapy in the ICU. Crit Care (London Engl). 2021;25(1):360. https://doi.org/10.1186/s13054-021-03787-z.
Falcone M, Bassetti M, Tiseo G, Giordano C, Nencini E, Russo A, . . . Menichetti F. Time to appropriate antibiotic therapy is a predictor of outcome in patients with bloodstream infection caused by KPC-producing Klebsiella pneumoniae. Crit Care (London Engl). 2020;24(1):29. https://doi.org/10.1186/s13054-020-2742-9.
Zasowski EJ, Claeys KC, Lagnf AM, Davis SL, Rybak MJ. Time Is of the Essence: The Impact of Delayed Antibiotic Therapy on Patient Outcomes in Hospital-Onset Enterococcal Bloodstream Infections. Clin Infect Dis. 2016;62(10):1242–50. https://doi.org/10.1093/cid/ciw110.
Lodise TP Jr, Patel N, Kwa A, Graves J, Furuno JP, Graffunder E, . . . McGregor JC. Predictors of 30-day mortality among patients with Pseudomonas aeruginosa bloodstream infections: impact of delayed appropriate antibiotic selection. Antimicrob Agents Chemother. 2007;51(10):3510–5. https://doi.org/10.1128/aac.00338-07.
Lodise TP, McKinnon PS, Swiderski L, Rybak MJ. Outcomes analysis of delayed antibiotic treatment for hospital-acquired Staphylococcus aureus bacteremia. Clin Infect Dis. 2003;36(11):1418–23. https://doi.org/10.1086/375057.
Kim D, Park BY, Choi MH, Yoon EJ, Lee H, Lee KJ, . . . Jeong SH. Antimicrobial resistance and virulence factors of Klebsiella pneumoniae affecting 30 day mortality in patients with bloodstream infection. J Antimicrob Chemother. 2019;74(1):190–9. https://doi.org/10.1093/jac/dky397.
Meites S, Buffone GJ. Pediatric clinical chemistry, references values, 3rd edn. American Association for Clinical Chemistry. Washington: American Association for Clinical Chemistry; 1989.
Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36(5):309–32. https://doi.org/10.1016/j.ajic.2008.03.002.
Gemke RJ, van Vught J. Scoring systems in pediatric intensive care: PRISM III versus PIM. Intensive Care Med. 2002;28(2):204–7. https://doi.org/10.1007/s00134-001-1185-2.
Cheng J, Zhang G, Li Q, Xu H, Yu Q, Yi Q, . . . Luo Z. Time to positivity of Klebsiella pneumoniae in blood culture as prognostic indicator for pediatric bloodstream infections. Eur J Pediatr. 2020. https://doi.org/10.1007/s00431-020-03675-8.
Cheng J, Zhang G, Li Q, Xu H, Yu Q, Yi Q, . . . Luo Z. Time to positivity of Klebsiella pneumoniae in blood culture as prognostic indicator for pediatric bloodstream infections. Eur J Pediatr. 2020;179(11):1689–98. https://doi.org/10.1007/s00431-020-03675-8.
Weiss SL, Peters MJ, Alhazzani W, Agus MSD, Flori HR, Inwald DP, . . . Tissieres P. Surviving sepsis campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Intensive Care Med. 2020;46(Suppl 1):10–67. https://doi.org/10.1007/s00134-019-05878-6.
Clinical and Laboratory Standards Institute. Performance standards for 407 antimicrobial susceptibility testing: 24th informational supplement. CLSI document 408 M100 -S24. Wayne: Clinical and Laboratory Standards Institute; 2014.
Magiorakos AP, Srinivasan A, Carey RB, Carmeli Y, Falagas ME, Giske CG, . . . Monnet DL. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–81. https://doi.org/10.1111/j.1469-0691.2011.03570.x.
Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, . . . Angus DC. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–10. https://doi.org/10.1001/jama.2016.0287.
Zhang H, Singer B. Recursive partitioning in the health sciences. New York: Springer; 1999. https://doi.org/10.1007/978-1-4757-3027-2.
Mandrekar JN. Receiver operating characteristic curve in diagnostic test assessment. J Thorac Oncol. 2010;5(9):1315–6. https://doi.org/10.1097/JTO.0b013e3181ec173d.
Weiss SL, Fitzgerald JC, Balamuth F, Alpern ER, Lavelle J, Chilutti M, . . . Thomas NJ. Delayed antimicrobial therapy increases mortality and organ dysfunction duration in pediatric sepsis. Crit Care Med. 2014;42(11):2409–17. https://doi.org/10.1097/ccm.0000000000000509.
Wiedermann CJ. Hypoalbuminemia as surrogate and culprit of infections. Int J Mol Sci. 2021;22(9):4496. https://doi.org/10.3390/ijms22094496.
Masterton R, Drusano G, Paterson DL, Park G. Appropriate antimicrobial treatment in nosocomial infections-the clinical challenges. J Hosp Infect. 2003;55(Suppl 1):1–12. https://doi.org/10.1016/s0195-6701(03)00294-9.
Moehring RW, Sloane R, Chen LF, Smathers EC, Schmader KE, Fowler VG Jr, . . . Anderson DJ. Delays in appropriate antibiotic therapy for gram-negative bloodstream infections: a multicenter, community hospital study. PLoS ONE. 2013;8(10):e76225. https://doi.org/10.1371/journal.pone.0076225.
Acknowledgements
Not applicable.
Funding
This study was supported by the Science and Technology Department of Chongqing (cstc2018jscx-msybX0021).
Author information
Authors and Affiliations
Contributions
All authors contribute to the study design, data acquisition, statistical analysis, article writing, revision, discussion and submission. All authors claim responsibility for this manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out in accordance with relevant guidelines and regulations. All authors declare that this study does not contain any human or animal experiments. This retrospective study was approved by the Ethics Committee of Children’s Hospital of Chongqing Medical University. File NO. (2020) 252. This is a retrospective study so that informed consent was exempted by the Ethics Committee of Children’s Hospital of Chongqing Medical University.
Consent for publication
Not applicable.
Competing interests
None reported.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cheng, J., Li, Q., Zhang, G. et al. Time to appropriate antimicrobial therapy serves an independent prognostic indicator in children with nosocomial Klebsiella pneumoniae bloodstream infection. BMC Pediatr 22, 568 (2022). https://doi.org/10.1186/s12887-022-03622-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-022-03622-6