
Abstract
Background
Substantial global progress has been made in reducing under-five mortality since 1990, yet progress is insufficient to meet the sustainable development goal of 2030 which calls for ending preventable child deaths. There are disproportional survivals among children in the world. Therefore, the study aimed to assess the Survival status of under-five mortality and determinants in Sub-Saharan African Countries using the recent DHS data.
Methods
The data was retrieved from the birth record file from the standard Demographic and Health Survey dataset of Sub-Saharan Africa countries. Countries that have at least one survey between 2010 and 2018 were retrieved. Parametric shared frailty survival analysis was employed.
Results
A total of 27,221 (7.35%) children were died before celebrating their fifth birthday. Children at an early age were at higher risk of dying and then decrease proportionally with increased age. The risk of death among rich and middle family were lowered by 18 and 8% (AHR =0.82, 95% CI: 0.77-0.87) and (AHR = 0.92, 95% CI: 0.87-0.97) respectively, the hazard of death were 11, 19, 17, 90 and 55% (AHR = 1.06, 95% CI: 1.00-1.12), (AHR = 1.11,95%CI:1.04-1.19), (AHR = 1.17, 95% CI:1.12-1.23), (AHR = 1.90, 95%CI: 1.78-2.04) and (AHR = 1.55, 95% CI:1.47-1.63) higher than among children in rural, use unimproved water, delivered at home, born less than 18 months and between 18 and 23 months birth intervals respectively. The hazard of death was 7% among females and low birth weights (AHR = 0.93, 95%CI: 0.90 – 0.97) and (AHR = 0.93 95%CI: 0.89-0.97) respectively. There was also a significant association between multiple births and birth orders (AHR = 2.11, 95%CI: 2.51 – 2.90), (AHR = 3.01, 95%CI: 2.85-3.19) respectively.
Conclusions
Death rate among under-five children was higher at an early age then decreases as age advanced. Wealth status, residence, water source, place of delivery, sex of the child, plurality, birth size, preceding birth interval, and birth order were the most predictor variables. The health care program should be designed to encourage a healthy family structure. The health care providers should intervene in the community to inspire maternal health services.
Similar content being viewed by others
Background
Under-five mortality (U5MR) is a key global indicator of child health and one of the most important measurements of nation development [1,2,3]. It is a serious issue for demographers and public health specialists and it is a core indicator of the development of families, societies, and the earth at large [4]. Under-five mortality is the probability of dying before celebrating 5 years of age and it is expressed as mortality per 1000 live birth [2, 3]. According to the report of the World Health Organization (WHO) and UNICEF [5, 6], substantial global progress has been made in reducing under-five mortality faster than any other time during the past two decades and since the 1990s, the global U5MR has dropped 53% from 91 per 100 live births in 1990s to 43 in 2015. Despite these gains, child existence remains an urgent concern. In 2013, around 17,000 children under age five die every day which showed that progress has been insufficient [7]. There are a disproportionate number of deaths among children less than 5 years of age in the world [3], particularly SSA regions had the highest death rate for children less than 5 years of age, with most of these deaths, occurred in the rural areas [3]. Because greater than two-third of the people are rural inhabitants [7,8,9]. Every year millions of children under 5 years of age die, mostly from preventable causes [3]. In 2015, more than 80% of the total 5.9 million under-five deaths were estimated to have occurred mostly from easily avoidable causes like pneumonia, diarrhea, and malaria in developing countries [10]. According to an estimate from GDB 2017 collaborates, even though numerous countries are on the track for achieving the target of SDGs at least 25 death per 1000 live birth by 2030, African countries would need to increase the annual rate of decline from 2015 to 2030 that two to ten times higher than what was recorded between 1990 to 2015 to meet the stated goals [11]. Furthermore, recent studies conducted in East Africa (Rwanda, Burundi, and Tanzania) have indicated that child survival has been influenced by community socio-demographic factors, maternal and child health characteristics, environmental and behavioral factors [12]. U5MR is still highest in the WHO African countries (greater than 80 per 1000 live birth, about 7 times higher than the WHO European region 11 per 100 live births in high-income countries however it is 11 times in low-income countries [12]. In the years, between 2016 to 2030 about 95 million children are projected to die between birth and exactly 5 years of age if the 2015 mortality rate remains constant in each country, and around 70 million would die if each country continues to reduce its mortality rate at peace estimate from 2000 to 2015. If all countries achieve the SDGs of 25 or fewer death per 1000 live birth by 2030, and 56 million death by 2030, therefore about two-third of all SSA countries need to accelerate progress to achieve this goal [13]. Here, the objective of this study was to estimate time to death, and its determinants among under-five children in SSA countries which are important for concerned bodies and strategists to take instantaneous actions. And it is also important to develop different designs to achieve the front SDGs. By 2030, SDGs agree to end preventable deaths on newborns and children under 5 year’s age. Deaths happening before celebrating the fifth birthday remain an enormous public health concern, especially in SSA and South Asian countries, and an overwhelming majority (80%) of the world’s estimated under-five deaths occurred in these two sub-regions [14]. Therefore to succeed in the SDGs target, justifiable efforts are needed mainly in developing countries.
Methods
Data sources
The data source was the recent (2010-2018) demographic and health survey (DHS) among 33 Sub-Saharan Africa countries. This standard Demographic and Health Survey is nationally representative and population-based surveys collected through uniform questionnaires and comparable across countries. The data were collected by multi-stage stratified cluster sampling design for each country. The details of the recorded data were accessed at www.measuredhs.com.
Populations and samples
The source population was all live births under 5 years of children preceded 5 years before each survey among 33 Sub-Saharan Africa countries. The data were extracted from the birth record (BR file) file from the standard DHS dataset of Sub-Saharan Africa countries with at least one survey from 2010 to 2018. A total of 370, 237 under-five children were included from 11 east African, 6 central African, 13 West African, and 3 South African countries.
Eligibility identification
In this study, all live births followed for 5-year full cohort preceding 5 years the survey in the selected enumeration areas in 33 Sub-Saharan African countries. However, some Sub-Saharan African Countries such as Central Africa Republic, Eswatini, Sao Tome Principe, Madagascar, and Sudan were not included in this study because they have no recent DHS data (no report after 2010/2011). As well, three Sub-Saharan Africa Countries such as Botswana, Mauritania, and Eritrea were excluded because their data set was not publicly available.
Outcome variable
The outcome variable of this study was the time to under-five children’s death. The survival time of a child beyond 59 months was declared as censored whereas children who died up to 59 months were declared as an event.
Independent variables
The independent variables were summarized as socio-demographic characteristics (parental educational status, wealth index of the household, residence, water source, sub-region, and County income), obstetric characteristics (birth interval, place of delivery, antenatal care visit, parity, and birth order), and under five-children and maternal characteristics (sex, weight, and plurality), etc.
Modeling of parametric shared frailty survival analysis
The frailty model is a random-effects model which has an unobserved multiplicative effect on the hazard rate for the entire individual in the same group. In the shared frailty model children in the same Country share the same nuisance (frailty) factor. Parameter θ provides information on the variability (the dependency) in the population in the same Country. Under-five children in the same Country i with ui > 1 and ui < 1 have a more frail than high risk and lower risk respectively. Based on the different frailty terms one frailty term was employed using Country taken as random effect dependency. For single frailty term model specification will be given by [15]
Where ui = exp(wi) is called the frailty for the ith Country. The ui’s, i = 1. . . s, are the actual values of a sample from a density fU.
Parametric frailty model fitted using Gompertz baseline hazard distributional assumption and gamma frailty distribution model fitted in Country taken as random effects frailty for the independent variables.
Level of dependence in the shared frailty model
The correlation between any two event times from the same country is measured by Kendall’s tau (τ). Kendall’s tau (τ) measured the dependency of two events in the same country which is dividing the frailty (θ) by two-plus frailty (θ). The higher frailty (θ) leads to the higher dependency and the higher Kendall’s tau (τ).
The best fit model selection
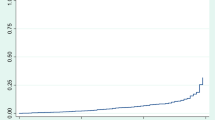
The best fit model was selected using Akakian Information Criteria (AIC) and the Log-likelihood ratio test. The lowest Akakian Information Criteria and the highest Log-likelihood ratio value declare the best fit model. Besides, the Cox-Snell residual plot was also employed for model adequacy. If the model fits, the Cox-Snell residuals should have a standard exponential distribution with λ = 1. One way to verify the fit is to calculate an empirical estimate of the cumulative hazard function based on the Kaplan–Meier survival estimates taking the Cox–Snell residuals as the time variable. If the model fits the data, the plot should be a straight line with a slope of 1.
Results
Weighted and unweighted samples in SSA using demographic and health survey data
Thirty-three SSA countries were included in this study. Greater than two in five 154,897 (41.83%) of the participants were found in the West African region with one in ten 34,433 (9.30%) concentrated in Nigeria. Greater than one –third 124,908 (33.75%) of the respondents were located in the East Africa region. Around one in fifteen 21,090 (5.7%) respondents were found in Kenya (Table 1).
Socio-demographic characteristics of the study participants
The majority 278,395 (75%) of the mothers were between the age of 20-35 years and their mean age was 29.24 ± 0.03. less than one-fourth 93,277 (24.54%) of the women were attended their secondary school and above. Around five out of seven 251,011 (70.11%) of the respondents have dwelled in rural. Nearly half 162,726 (47.75%) of the study participants had poor wealth status. Among four sub-regions of Sub-Saharan Africa: about four in ten 154,023 (42%) of them reside in the central region. However, South Africa accounts for 11,549 (3.19%) (Table 2).
Under five-children and maternal obstetric characteristics of the study participants
Of the total under-five children, the proportion of male and females children are almost equal (50%). Surprisingly around two-thirds, 219,360 (63.32%) of them were exposed to low birth weight and greater than half 207,429 (56.07%) of their birth order was less than three. Only 218,559 (59.15%) of the women have at least one ANC follow-up (Table 3).
Under-five children’s survival in Sub-Saharan Africa
Of the total of 370,237 under-five children, 27,221 (7.35%) were died before celebrating their fifth birthday. From the total of under-five children followed for 5 years, the cumulative probability of survival at the end of 5 years was 89.54% (95% CI: 0.89-0.90). But the cumulative survival among male and female was 88.74% (95% CI: 0.89-0.90) and 90.36% (95% CI: 0. 90-0.91) respectively. The cumulative probability of survival at 1 year was 92.59% (0.92-0.93) (Table 4).
Kaplan Meier survival analysis
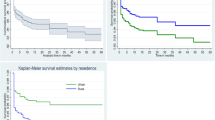
The survival probability of under-five children was estimated using Kaplan Meier survival estimate. The Kaplan Meier confirms with the life table results. The survival probability is very low among newborns and starts to stabilize when the child reaches 2 years of age. This means that children age between 0 and 2 years are at a higher risk of dying and the risk decreases proportionally with the increase of age for both children aged between 0 and 2 years and those aged between 2 and 5 years (Fig. 1A). The probability of death among children who had lower than 24 months of pregnancy interval (Fig. 1C) and women’s didn’t expose to antenatal care follow-up (Fig. 1E) were higher. The highest probability of death among under-five children was in the Western Africa region of SSA. Among those who are between the age of one and 2 years old children, the probability of death was higher among children living in South Africa. However, the survival probability of under-five children after 2 years of age in West Africa and Central Africa was proportional through 5 years of life. Similarly, the probability of survival of children after 2 years was proportional throughout 5 years period of life in East and South Africa (Fig. 1D). The probabilities of death among children who live in the rural area (Fig. 1B) and delivered at home (Fig. 1F) were higher as compared to children living in urban and delivered at health institutions respectively.

Overall survival estimate of under-five children (A), survival estimates in residence (B), survival estimates in Pregnancy interval (C), survival estimates in SSA-regions (D), survival estimates by ANC visit (E), survival estimates by place of delivery (F)
Model comparison
The study tried to fit different baseline hazard parametric distributional assumptions. Based on the information criteria Gompertz baseline distribution was the best fit model with gamma frailty distribution. The Log-logistic and Lognormal baseline hazard distribution model and the inverse Gaussian frailty distribution models did not converge. Therefore, Gompertz’s baseline distribution with gamma frailty distribution was the best fit model since it has the lowest AIC value (Table 5).
Factors associated with under-five children mortality in Sub-Saharan Africa
To recognize the potential significant factors for under-five children mortality country-level parametric shared frailty survival model was fitted. The value of the shape parameter in the Gompertz baseline hazard distribution model was (ρ = −0.04, 95%CI: −0.043 – − 0.039). This negative value indicates that the hazard of death among under-five children had decreased exponentially as the age of under-five children increase. The dependency (heterogeneity) of under-five children in the same country estimated by the model was statistically significant with a value theta (θ = 0.07, 95% CI: 0.04-0.12), and the dependency within-country was τ = 3%.
After controlling country-level frailty, the results from Gompertz parametric baseline hazard distribution revealed the educational status of the husband/intimate partner, wealth status, residence, water source, sex of the child, preceding birth interval, birth order, birth size, and place of delivery were statistical predictors of under-five child survival.
The hazard of death among children who were born from rich and middle families was lower by 18% (AHR =0.82, 95% CI: 0.77-0.87) and 8% (AHR = 0.92, 95% CI: 0.87-0.97) respectively. The risks of death among under-five children were; residing in a rural area, used water from an unimproved source, and delivered at home. Those who reside in rural were 11% times more at risk of death when compared with urban dwellers (AHR = 1.06, 95% CI: 1.00-1.12). Those who had water from improved water sources had 19% times at risk of death when compared with those who had improved water sources (AHR = 1.11, 95%CI: 1.04-1.19). In the same way, those who were born at home had a 17% reduced risk of death when compared to those who are born in the health institutions (AHR = 1.17, 95% CI: 1.12-1.23).
The estimated hazard of death among female under-five children and not low birth weight were lowered by 7% as compared to male infants and low birth weight under-five children (AHR = 0.93, 95%CI: 0.90 – 0.97) and (AHR = 0.93 95%CI:0.89-0.97) respectively. The hazard of death among multiple-birth children was 2.1 times higher than singleton births (AHR = 2.11, 95% CI: 2.51 – 2.90). The estimated hazard among under-five children born less than 18 months and between 18 and 23 months preceding birth interval was a higher risk of death by 90 and 55% than children born greater than 24 months interval (AHR = 1.90, 95%CI: 1.78-2.04) and (AHR = 1.55, 95% CI:1.47-1.63) respectively. Children born from birth order of four and above was 3 times (AHR = 3.01, 95%CI: 2.85-3.19) higher risk of death as compared to the birth order of less than four (Table 6).
Discussions
The estimation of child mortality is challenging for the great majority of developing countries without a well-functioning vital registration system due to issues with data quality (and for some countries data quantity) [16]. The Sub-Sahara region made significant development in increasing child survival for the past two decades. But the survival rates are still steady especially among newborns which indicates the region’s level of improvement in the quality of life [3, 9, 16]. And these rates are also important in identifying the directions for the public health program in the region.
In the current study, therefore, we tried to assess the survival status of under-five mortality and its determinants in Sub-Saharan Africa using the recent (2010-2018) Demographic and Health Survey data with country-based Shared frailty analysis. The result of this study indicated that out of 370,237 under-five children 27,221 (7.35%) were died before celebrating their fifth birth year. Children’s death depends on socio-demographic characteristics of the respondents, child characteristics, obstetric and environmental factors. Hence, this study revealed that the hazard of death among under-five children decreased exponentially as the age of under-five children increase. This means that the survival probability was very low among newborns. This finding is consistent with findings of other multi-country analyses [3, 7, 17]. Because newborns are exposed to prematurity, low birth weight, intrauterine growth retardation, and at an early age, since they are new for the external environments, newborns are susceptible to easily preventable child deaths such as birth trauma, asphyxia, hypothermia, sepsis, and lack of essential newborn care services. The higher number of births was associated with a greater risk of under-five mortality than their counterparts y. Studies have also shown a similarly elevated risk of under-five mortality among children born to mothers who gave more birth [3, 9, 18, 19]. This is because; higher parity is often associated with short-birth intervals, which influence under-five mortality risk through depletion of mother’s health and nutritional status, and premature birth [20]. Children from rich and middle economic status households experienced a lower risk of under-five mortality compared with households from poor economic status. In a similar vein, studies in 55 low resource countries using household assets index to measure wealth status found that under-five child mortality was significantly higher among households whose economic status is poor than households that had higher economic status [7, 21,22,23]. The effect of household wealth status on under-five children mortality may have operated through access to goods and services such as food, housing transportation, or financial access to care [24].
We also found evidence that the length of preceding birth interval was significantly associated with the risk of death before age of five. The hazard of death among under-five children born less than 18 months preceding birth interval was higher by 2 times than children born birth interval for more than 2 years. The risk of death is also higher by 1.5 times among children born from the birth interval between 18 and 23 months compared to a birth interval greater than 24 months. Thus, agreeing with the findings of some previous studies [3, 9, 16, 21, 22, 25]. A possible explanation is that a shorter length of the birth interval increases the risk of premature birth, low birth weight, maternal depletion syndrome, folate insufficiency, and newborn exposure to the susceptibility of infectious disease and in addition, it leads to competition in familial resource among children [26]. The risk of under-five mortality was slightly (by 7%) lower among female children as compared to male children. This has been explained by a sex difference in genetics and biological make-up that girls are advantage against many causes of death over boys [27, 28]. Excess male child mortality can be explained by biological factors (lower resistance to infection, higher risk of prematurity birth, difficult labor related to a larger average body size and head circumference), gender discrimination differential feeding and medical care practice, or response to HI related drugs [29, 30]. The size of children at birth was found to be significantly associated with higher under-five mortality.
Being low birth weight was a risk for child mortality. This evidence is also supported by other findings that small-sized children at birth have a higher risk of dying before they reach the fifth birthday [3, 21, 31]. This might be due to the immaturity of their organs which makes them find it more difficult to adapt to the external environment and independent life. Most premature babies are prone to have sepsis which is one of the major causes of under-five mortality [3, 32]. Furthermore, this study suggests that children from mothers who live in rural areas were significantly associated with high under-five mortality compared to those who live in the urban area. This concurs with previous studies in Cambodia and Nigeria [21, 25]. This is on the ground that those who live in the urban area have access to improved water supply, improved sanitation facility, unlimited health care access as well as other social and economic services [32, 33]. Findings have shown that children born other than health institutions have a 17% risk experience of under-five mortality compared to under-five children who were born in a health institution. Similar studies conducted in Pakistan [27], Indonesia [22], and Nigeria [21] showed that the place of delivery is significantly associated with childhood survival. Children born from mothers who have access to safe drinking water had a significant risk of under-five mortality.
This finding was supported by studies carried out in Cambodian [25], Nigeria [34], Egypt, and Eretria [35, 36]. The possible explanation for this finding is that children learn to crawl and walk and they experience exposure to pathogens that causes diarrhea from a variety of environmental sources, including contaminated water [37]. It is also households often use unimproved water to prepare weaning foods; thereby transmitting pathogens to children that causes diarrheal disease which has been resulted in high mortality [38, 39]. This study showed that the risk of death was 2.7 times higher among multiple birth under-five children as compared to singleton births. This evidence was similar to previous studies carried out in Unit states of America, Guinea Bissau, and Ethiopia [40,41,42].
The likely enlightenment for this evidence might be multi-fetal pregnancy and births lead to adverse pregnancy outcomes and child health, Another explanation might be parents with multiple births experience more anxiety, stress, and depression in the first year of life after birth than parents who had singletons birth. The probability of under-five mortality increases with total children ever born and this finding was consistent with preceding studies [32, 43, 44]. Also, an increase in the total number of children ever born could result in lack of care, low birth weight, premature births and heavy drain on the limited household resources as children have to compete for the little resources available for their survival. The likelihood of child survival decreased among children who are products of multiple births compared to their counterparts who were products of singletons. Low birth weight or competition for nutritional intake which occurs more among children who are products of multiple births could be a plausible explanation [44,45,46].
Limitations
Data were collected cross-sectional at a different point in time by self-reported interview which might be prone to recall and social desirability bias. The drawback of the secondary nature of data was expected.
Conclusions
The hazard of death among under-five children was higher at an early age than decrease as age advanced which means that the survival probability was very low among newborns. Wealth status, residence, water source, place of delivery, sex of the child, plurality, birth size, preceding birth interval, and birth order were the most predictor variables. In light of the above, we suggest that health care programs should be designed specifically to encourage a healthy family structure. Government and non-government organizations must work together to access safe water in the region and inspire maternal and child health services. The health care providers should intervene in the community to increase the health of the child and the health of the family as a whole.
Availability of data and materials
All the data sets are available on the hand of the corresponding author.
Abbreviations
- AHR :
-
Adjusted Hazard Ratio
- ANC:
-
Antenatal care
- DHS:
-
Demographic and health survey
- SSA:
-
Sub Saharan Africa
- GDB:
-
Global Disease Burdon
- SDGs:
-
Sustainable Development Goals
- WHO:
-
World Health Organization
References
McGuire JW. Basic health care provision and under-5 mortality: a cross-national study of developing countries. World Dev. 2006;34(3):405–2.
UNICEF. The under-five mortality rate: the indispensable gauge of child health. 2016. www.unicef.org/sowc08/docs/sowc08_panels.pdf. Accessed Mar 2016.
UNICEF, WHO, World Bank, UN-DESA Population Division. Levels and trends in child mortality report 2017: Estimates developed by the UN Inter-Agency Group for Child Mortality Estimation; 2018.
Global Health Observatory (GHO) data, 2017. http://www.who.int/gho/child_health/mortality/mortality_under_five_text/en/. Accessed 15 Jan 2018.
WHO. Children: reducing mortality. 2016. http://www.who.int/mediacentre/factsheets/fs178/en/. Accessed 26 Mar 2017.
UNICEF. Committing to child survival: a promise renewed progress report 2014. New York: UNICEF; 2014. http://data.unicef.org/corecode/uploads/document6/uploaded_pdfs/corecode/APR-2014-17Oct14-web_194.pdf
Wardlaw T, et al. UNICEF Report: enormous progress in child survival but greater focus on newborns urgently needed. Reprod Health. 2014;11:1–4.
National Institute of Statistics of Rwanda, Ministry of Finance and Economic Planning, Ministry of Health, and ICF International. Rwanda demographic and health survey 2014–2015. Rockville: ICF International; 2015.
Khan JR, Awan N. A comprehensive analysis on child mortality and its determinants in Bangladesh using frailty models. Arch Public Health. 2017;75:58.
National Statistics Bureau. Statistical year book of Bhutan 2016. Thimphu: Royal Government of Bhutan. http://www.nsb.gov.bt/publication/publications.php?id=3. Accessed 21 Aug 2018.
GBD 2017 Mortality Collaborators. Global, regional, and national age-sex-specific mortality and life expectancy, 1950–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392:1684–735.
UNICEF, WHO, World Bank, UN-DESA Population Division. Levels and trends in child mortality, 2015. Geneva: World Health Organization; 2015. Available from: https://www.who.int/maternal_child_adolescent/documents/levels_trends_child_mortality_2015/en/. Accessed Dec 2017
Lucia Hug D, et al. Global, regional, and national levels and trends in under-5 mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Inter-agency Group for Child Mortality Estimation. https://doi.org/10.1016/S0140-6736(15)00193-2.
United Nations Inter-Agency Group for Child Mortality Estimation (UN IGME). Levels & trends in child mortality: report 2017. New York: Estimates Developed by the UN Inter-Agency Group for Child Mortality Estimation; United Nations Children’s Fund; 2017.
Janssen LDP. The frailty model: Springer Science+Business Media, LLC; 2008. p. 1–329.
Marie R, Wajambo N. Survival analysis of time to event data an application to child mortality in Sub-Saharan Africa region using their demographic and health surveys 2018. Master’s program “Applied Statistics” Örebro University School of Business Health Surveys.
Yaya S, Bishwajit G, Okonofua F, Uthman OA. Under five mortality patterns and associated maternal risk factors in sub-Saharan Africa: a multi-country analysis. PLoS One. 2018;13(10):e0205977.
Dendup T, Zhao Y, Dema D. Factors associated with under-five mortality in Bhutan: an analysis of the Bhutan National Health Survey 2012. BMC Public Health. 2018;18:1375.
Adhikari R, Podhisita C. Household headship and child death: evidence from Nepal. BMC Int Health Hum Rights. 2010;10:13.
Hobcraft JN, McDonald JW, Rutstein SO. Demographic determinants of infant and early child mortality: a comparative analysis. Popul Stud. 1985;39(3):363–85.
Wegbom AI, Essi ID, Kiri VA. Survival analysis of under-five mortality and its associated determinants in Nigeria: evidence from a survey data. Int J Stat Appl. 2019;9(2):59–66.
Warrohmah A, et al. Analysis of the survival of children under five in Indonesia and associated factors. In: 3rd International Conference on Tropical and Coastal Region Eco Development 2017, IOP Conf. Series: Earth and Environmental Science, vol. 116; 2018. p. 012014.
Hertzman C, et al. Bucking the inequality gradient through early child development. BMJ. 2010;340(2):468–87.
Kanmiki EW, Bawah AA, Agorinya I, Achana FS, Awoonor-Williams JK, Oduro AR, et al. Socio-economic and demographic determinants of under-five mortality in rural northern Ghana. BMC Int Health Hum Rights. 2014;14:24.
Vanthy L, Chhorvann C, Bunleng H, Sopheab H. Determinants of children under-five mortality in Cambodia: analysis of the 2010 and 2014 demographic and health survey. Int Arch Public Health Community Med. 2019;3:029.
Rutstein SO. Effects of preceding birth intervals on neonatal, infant and under-five years mortality and nutritional status in developing countries: evidence from the demographic and health surveys. Int J Gynecol Obstet. 2005;89:7–24.49.
Alonso V, Fuster V, Luna F. Causes of neonatal mortality in Spain (1975–98): influence of sex, rural-urban residence, and age at death. J Biosoc Sci. 2006;38(04):537–51.
Sawyer CC. Child mortality estimation: estimating sex differences in childhood mortality since the 1970s. PLoS Med. 2012;9(8):1001287.
Drevenstedt GL, Crimmins EM, Vasunilashorn S, Finch CE. The rise and fall of excess male infant mortality. Proc Natl Acad Sci U S A. 2008;105(13):5016–21.
Yaya S, Diarra S, Mabeu MC, Pongou R. The sex gap in neonatal mortality and the AIDS epidemic in sub-Saharan Africa. BMJ Glob Health. 2018;3(5):1–5.
Adebowale SA, Morakinyo OM, Ana GR. Housing materials as predictors of under-five mortality in Nigeria: evidence from 2013 demographic and health survey. BMC Pediatr. 2017;17:30.
Kayode GA, Adekanmbi VT, Uthman OA. Risk factors and a predictive model for under-five mortality in Nigeria: evidence from Nigeria demographic and health survey. BMC Pregnancy Childbirth. 2012;12:10.
Dejene T, Girma E. Social determinants of under-five mortality in Ethiopia: event history analysis using evidence from Ethiopian Demographic and Health Survey (EDHS). Health (Irvine. Calif). 2013;5:879–84.
Kingsley EO, et al. The impact of water and sanitation on childhood mortality in Nigeria: evidence from demographic and health surveys, 2003–2013. Int J Environ Res Public Health. 2014;11:9256–72.
Woldemicael G. The effects of water supply and sanitation on childhood mortality in urban Eritrea. J Biosoc Sci. 2000;32:207–27.
Ali HA. The effect of water and sanitation on child mortality in Egypt. Göteborg: Environmental Economics Unit, Göteborg University; 2003.
World Health Organization. The physical school environment: an essential element of a health-promoting school. Geneva: World Health Organization; 2003.
Vanderslice J, Popkin B, Briscoe J. Drinking-water quality, sanitation, and breast-feeding: their interactive effects on infant health. Bull World Health Organ. 1994;72:589–601.
Jinadu MK, Olusi SO, Agun JI, Fabiyi AK. Childhood diarrhea in rural Nigeria. I. Studies on prevalence, mortality, and socio-environmental factors. J Diarrhoeal Dis Res. 1991;9:323–7.
Byberg S, Stergaard MD, Rodrigues A, Martins C, Benn CS, Aaby P, et al. Analysis of risk factors for infant mortality in the 1992-3 and 2002-3 birth cohorts in rural Guinea-Bissau. PLoS One. 2017;12(5):1–15.
Rathe M, Müller K, Sangild PT, Husby S. Clinical applications of bovine colostrum therapy: a systematic review. Nutr Rev. 2014;72(4):237–54.
Zhao D, Zou L, Lei X, Zhang Y. Gender differences in infant mortality and neonatal morbidity in mixed-gender twins. Sci Rep. 2017;7(1):3–8. https://doi.org/10.1038/s41598-017-08951-6.
Abir T, Agho KE, Page AN, Milton AH, Dibley MJ. Risk factors for under-5 mortality: evidence from Bangladesh demographic and health survey, 2004–2011. BMJ Open. 2015;5:e006722.
Amoroso CL, Nisingizwe MP, Rouleau D, Thomson DR, Kagabo DM, Bucyana T, et al. Next wave of interventions to reduce under-five mortality in Rwanda: a cross-sectional analysis of demographic and health survey data. BMC Pediatr. 2018;18(1):27.
Aheto JMK, Keegan TJ, Taylor BM, Diggle PJ. Childhood malnutrition and its determinants among under-five children in Ghana. Paediatr Perinat Epidemiol. 2015;29:552–61.
Adekanmbi VT, Kayode GA, Uthman OA. Individual and contextual factors associated with childhood stunting in Nigeria: a multilevel analysis. Matern Child Nutr. 2013;9(2):244–59.
Acknowledgments
Our deepest gratitude goes to the Demographic and Health Survey (DHS) data archivist that allows accessing the dataset.
Funding
No fund was accepted from any organization for this research.
Author information
Authors and Affiliations
Contributions
Desalegn Tesfa and Sofonyas Abebaw were involved in this study from the inception to design, acquisition, analysis, and interpretation of data and drafting of the manuscript. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
An ethical clearance letter was obtained from the Institutional Review Board of Debre Tabor University. As well, waiver of written informed consent was secured from the International Review Board of Demographic and Health Surveys (DHS) program data archivists to download the dataset for this study. The dataset was not shared or passed on to other bodies.
Consent for publication
Not applicable for this section.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tesfa, D., Tiruneh, S.A., Azanaw, M.M. et al. Time to death and its determinants among under-five children in Sub-Saharan Africa using the recent (2010–2018) demographic and health survey data: country-based shared frailty analyses. BMC Pediatr 21, 515 (2021). https://doi.org/10.1186/s12887-021-02950-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-021-02950-3