
Abstract
Background
The aim of the study was to determine whether the combination of Glasgow Coma Scale (GCS) and Pupil responses score (GCSP) with arterial lactate level would be an index to predict the short term prognosis in patients with traumatic brain injury (TBI).
Methods
A retrospective study was performed enrolling all TBI patients admitted to intensive care unit (ICU) from 2019 to 2020. The demographics, clinical characteristics, and arterial lactate concentration were recorded. The GCSP and arterial blood analysis (ABG) with lactate was tested as soon as the patient was admitted to ICU. The Glasgow Outcome Scale (GOS) after discharge was regarded as the clinical outcome. A new index named GCSP-L was the combination of GCSP and lactate concentration. GCSP-L was the GCSP score (range 1-15) plus the lactate score (range 0-2). The lactate score was defined based on different lactate concentrations. If lactate was below 2 mmol/L, lactate score was 0, which above 5 mmol/L was 2 and between 2 and 5 mmol/L, the score was 1. As the range of GCSP was 1-15, the range of the GCSP-L was 1 to 17. The area under receiver operating characteristic curve (AUC) was calculated to evaluate the predictive ability of GCSP, lactate and GCSP-L. Statistical significance was set when p value < 0.05.
Results
A total of 192 TBI patients were included in the study. Based on GCSP, mild, moderate, and severe TBI were 13.02, 14.06 and 72.92%, respectively. There were 103 (53.65%) patients with the lactate concentration below 2 mmol/L (1.23 ± 0.37 mmol/l), 63 (32.81%) of the range from 2 to 5 (3.04 ± 2.43 mmol/l) and 26 (13.54%) were above 5 mmol/l (7.70 ± 2.43 mmol/l). The AUC was 0.866 (95% CI 0.827-0.904) for GCSP-L, 0.812 (95% CI 0.765-0.858) for GCSP and 0.629 (95% CI 0.570—0.0.688) for lactate. The AUC of GCSP-L was higher than the other two, GCSP and lactate alone.
Conclusions
The combination of GCSP and lactate concentration can be used to predict the short term prognosis in TBI patients.
Similar content being viewed by others

Background
Traumatic brain injury (TBI) is a common type of trauma worldwide [1] and a major cause of physical and cognitive disability [2]. It’s important for early identification of a patient’s clinical condition, reliable prognostic factors. Outcome prediction and severity evaluation are useful for clinical decision making, family counseling, evaluation of the quality of treatment, and medical resource allocation [1]. A simple combination of the Glasgow Coma Scale (GCS) and Pupil responses (GCSP) have been shown to be an early indicator of prognostic information and an extended index of clinical severity in TBI patients [3]. The GCSP is used to assess 4 aspects of a patient’s responsiveness, which are eye, verbal, motor responses, and pupil responses. Each of these aspects contains information about prognosis [4].
Nowadays the role of arterial lactate in TBI has gained great interest. Although higher arterial lactate may be a biomarker of poor systemic physiology, it may have neuroprotective effects on the intracranial pressure (ICP), the cerebral blood flow (CBF), and cerebral cellular metabolism [5, 6]. Some studies also have demonstrated that exogenously administered lactate has been associated with improved outcomes [7]. High lactate may be a protective factor for TBI patients. An arterial blood analysis (ABG) with lactate will be obtained immediately as soon as TBI patients are admitted to the intensive care unit (ICU). It’s rapid and convenient to have the arterial lactate concentration.
The GCSP score, together with the lactate concentration may be a simple and useful index to evaluate clinical severity and predict the prognosis. The aim of the study was to determine whether the combination of GCSP score with arterial lactate would be a good index to evaluate clinical severity and predict the prognosis in TBI patients.
Methods
Patients
This study was a retrospective study. The study was approved by the Ethics Committee of Beijing Tiantan Hospital. All TBI patients admitted to the ICU at Beijng Tiantan Hospital, Capital Medical University in China from 2019 to 2020 were enrolled in the study. Exclusion criteria: The patients with a history of chronic kidney and liver diseases, unstable hemodynamics, and obvious sign of infection (pulmonary, intracranial infection et al), were excluded. These diseases affect lactate concentration. And the patients with age under 18 years old, without ABG or Glasgow Outcome Scale (GOS) were excluded.
All the patients who met the criteria of TBI would be admitted directly to ICU of the hospital within 4 h of injury. All TBI patients received the same initial standardized treatment protocol, which included appropriate resuscitation and stabilization in accordance with the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC) [8]. After admitted to the ICU, neurologic evaluation will be performed immediately, including GCS score, pupil reactivity, and neurologic deficits. Patients were examined by CT scan as soon after stabilization as possible. According to CT findings, patients were taken either to the operating room for surgical evacuation of significant space-occupying lesions, or conservative management in ICU. CT scanning was repeated 6 and 24 hours after injury, as well as immediately after surgery, or when a patients level of consciousness deteriorated. An intracranial pressure (ICP) monitor or a ventricular catheter was inserted as needed. Arterial blood samples (ABG) were taken at admission for blood gas analysis.
Data collection
The demographics and clinical characteristics were recorded after the patients were admitted to ICU, such as age, gender, body mass index (BMI), type of injury, acute physiology and chronic health evaluation II (APECHE II), injury severity score (ISS), initial GCS, pupil reactivity at admission of ICU. And every patient would have an ABG test for the first time after being admitted to ICU, thus the lactate concentration would be recorded.
ISS calculation divides the body into 6 areas. ISS is the sum of the squares of the highest abbreviated injury score (AIS) evaluation values of the 3 most severely injured areas. The ISS score ranges from 1 to 75 points. The mild to moderate is defined as ISS sore ranging from 1 to 8. And 9 to 15 is considered as serious injury, 16 to 24 is severe injury, ≥ 25 is critical injury.
GCSP is defined as the combination of GCS score and pupil reactivity score [3]. The pupil reactivity score is to reflect the number of nonreactive pupils. If both pupils are unreactive to light the score was 2. If only 1 pupil is unreactive to light the score is 1. If neither pupil is unreactive to light the score is 0. Thus, GCSP is obtained simply by subtracting the pupil reactivity score from the GCS total score. The range of GCSP is 1 to 15. GCSP score can be used to classify injuries, which 1 to 8 is mild, 9 to 12 is moderate and severe is range from 13 to 15 [3].
The combination of GCSP and arterial lactate concentration (GCSP-L)
We first constructed a lactate score [9]. If the lactate concentration was below 2 mmol/L [9], the lactate score was 0. If it was above 5 mmol/L [6, 10], the score was 2. If it was between 2 and 5 mmol/L, the score was 1. Next, a combined GCSP-L was obtained by GCSP score plus the lactate score, GCSP-L = GCSP score + Lactate score. Since the GCSP score has a range from 1 to 15, the GCSP-L can range of possible values from 1 to 17.
Outcome
Clinical outcome was assessed after discharge using the GOS. 1 = death, 2 = vegetative, 3 = severe disability, 4 = moderate disability, 5 = good recovery. Favorable outcomes were considered good recovery and moderate disability; severe disability, vegetative state, and dead were unfavorable. And ICU length of stay, hospital length of stay would be recorded.
Statistical analysis
Given the nonnormality, data were expressed as mean with standard deviation (SD), and numbers and percentages for categorical variables. Receiver operating characteristic curve (ROC) analysis was used to estimate the prediction. The area under ROC (AUC) was calculated to evaluate the predictive ability of GCSP, lactate and GCSP-L. Statistical significance was set when p value < 0.05. All statistics were analyzed using GraphPad Prism version 8.0 (GraphPad Software, USA) and SPSS version 25.0 (IBM Corporation, USA).
Results
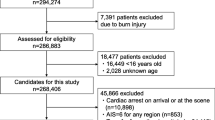
There were 214 TBI patients enrolled in the study. Out of 214 TBI patients, there were 2 patients without ABG after being admitted to ICU and 5 without GOS after discharge. Fifteen patients were excluded, 2 patients because they were below 18 years old, 3 because they have had kidney disease, 4 because of liver diseases, 4 for unstable hemodynamics, and 2 for a doubtful sign of intracranial infection. Thus, there were 192 TBI patients included in the study (Fig. 1). The TBI patients would be admitted to ICU. All the patients were treated in accordance with the standardized management protocol [8].

The flowchart of the study. A total of 214 patients with traumatic brain injury (TBI) were screened over the 2 years; 22 patients were excluded in the study. ABG = arterial blood analysis, GOS = Glasgow Outcome Scale
Demographics, admission status and clinical outcome
Of the 192 TBI patients included in the study, the mean age was 54 ± 16 years old and 75% were male (Table 1). The types of TBI were intracranial hemorrhage (ICH), subdural hemorrhage (SDH), epidural hemorrhage (EDH), diffuse axonal injury, and others, respectively 51.56, 27.08, 14.06, 4.69, and 2.60%. The critical patients were 69.79% among the patients according to ISS (Table 1). Head AIS made the maximal contribution in ISS score of all the patients. According to CT findings, 112 patients (58.33%) were taken to the operating room for surgery. Of all TBI patients, 65.63% (126 patients) were received mechanical ventilation. Most of the patients were received sedation and analgesia, 95.83 and 96.88% respectively.
Based on GCSP, the score between 13 to 15 considered as mild was 13.02%, moderate (9-12) and severe (1-8) were 14.06 and 72.92%, respectively. The percentage of favorable outcomes was 27.62% (GOS after discharge: good recovery 15.63%, moderate disability 11.98%). ICU length of stay was 19 ± 18 days, and hospital length of stay (23 ± 21) days (Table 1).
There were 103 (53.65%) patients with the lactate concentration below 2 mmol/L (1.23 ± 0.37 mmol/l). Meanwhile, the number of range from 2 to 5 was 63 (32.81%), and the mean lactate was 3.04 ± 2.43 mmol/l. The others (26 (13.54%)) were above 5 mmol/l, and mean lactate was 7.70 ± 2.43 mmol/l (Table 1).
Sensitivity and specificity based on GCSP, GCSP-L and lactate
The ROC curves are shown in Fig. 2. The GCSP-L achieved the largest AUC of 0.866 (95% confidence interval [CI], 0.827-0.904), which was higher than the others, 0.812 (95% CI 0.765-0.858) for GCSP and 0.629 (95% CI 0.570—0.0.688) lactate respectively.

The receiver operating curves (ROC) of GCSP, lactate and GCSP-L. The area under the receiver operating characteristic curve (AUC) was 0.866 (95% CI 0.827-0.904) for GCSP-L, 0.812 (95% CI 0.765-0.858) for GCSP and 0.629 (95% CI 0.570—0.0.688) for lactate. GCSP = Glasgow Coma Scale and Pupil response score, GCSP-L = Glasgow Coma Scale, Pupil response and Lactate score
Discussion
Lactate is an important biomarker of systemic physiology and may have neuroprotective effects in TBI patients. GCS score and pupil reaction are two clinical features, that provide some information about prognosis for a brain-injuryed patient. This study combined the lactate concentration and GCSP score, which named GCSP-L, to predict short term prognosis in TBI patients. The findings highlighted that GCSP-L can be used to predict the short term prognosis, and may provide more information than either GCSP or lactate alone.
GCS score is widely used as an index of brain damage, differing severity and monitoring patients’ progress and estimating prognosis [11]. GCS score assess 3 aspects of a patient’s responsiveness, they are eye, verbal, and motor responses [4]. Each of these aspects contains information about prognosis. Recently, a simple combination of GCS and Pupil responses (GCSP) have been shown to be an early indicator of prognostic information and an extended index of clinical severity in TBI patients [3]. GCSP yields more informative data than using either GCS or pupil reaction alone. Nowadays, some researches are using GCSP to prognosis and estimate severity in TBI patients [12]. So this study used GCSP as the reference index to estimate severity and prognosis.
High arterial lactate is considered to be a prognosis factor of poor systemic physiology and poor outcome, however, in TBI patients it may have a protective and beneficial effect [6]. A study demonstrated that there was a negative correlation between arterial lactate and ICP in severe TBI patients [13]. ICP decreased while arterial lactate increased. High arterial lactate could regulate the cerebral vessels by vasodilation leading to reduce ICP [7] and increases in the CBF [5]. With these effects, high lactate may be beneficial for TBI patients. Further the role of arterial lactate as cerebral energy fuel in TBI has gained interest the last years [14, 15]. Some researches have showed that exogenous supplemental lactate can be utilized aerobically as a preferential energy substrate after TBI [7]. The experimental group gave an intervention of a 3-h intravenous infusion of hypertonic sodium lactate (aiming to increase systemic lactate to 5 mmol/L). With the sodium lactate therapy, a significant increase in cerebral microdialysis concentrations of lactate was observed and also a decrease of ICP. In a word, high lactate may have neuroprotective effects and beneficial effects at TBI patients. Thus, the study used GCSP plus lactate score as a new index (GCSP-L) to evaluate the severity of TBI patients.
Generally, hyperlactatemia is defined as lactate levels > 2 mmol/L, whereas lactic > 4 mmol/L represents acidosis [9]. But in this study we used 5 mmol/l as the second grading criteria. If it was above 5 mmol/L, the score was 2. If it was between 2 and 5 mmol/L, the score was 1. Because some studies demonstrated that the arterial lactate contribution to cerebral lactate will increase to 60% at 5 mmol/L [6, 10], which will serve as cerebral energy fuel especially the cerebral lactate. Some studies showed that infusing exogenous supplemental lactate to maintain lactate concentration above 5 mmol/l, the lactate can be utilized as cerebral energy fuel [7].
After admitted to the hospital or ICU, GCSP assessment and a ABG test will be performed immediately. It’s very easy and rapid to have the results of the combination of GCSP and lactate concentration. Although GCSP is widely used for assessment of a patient’s clinical condition, the AUC of GCSP-L is greater than GCSP and lactate (AUC 0.866, 0.812 and 0.629 respectively). GCSP-L can be used to predict the short term prognosis and GCSP-L may provide more information about clinical severity and outcomes than either GCSP or lactate alone.
There are some limitations in the study. First, the study screened all the TBI patients immediately after admitted to the ICU within 4 hours. But we didn’t have the exact data of the time from the patients were injured to visiting the hospital. If the lactate can be obtained at once TBI happened, the GCSP-L may be more precise to evaluate the short term prognosis. Second, there were 69.79% critical patients according to ISS. The patients were severe and poor prognosis. However, the patients with severe unstable hemodynamic were excluded. Third, this was a retrospective study. A larger patient population and randomized controlled trials should be performed.
Conclusions
The combination of GCSP and lactate concentration can be used to predict short term prognosis in TBI patients.
Availability of data and materials
The datasets analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- TBI:
-
Traumatic Brain Injury
- GCS:
-
Glasgow Coma Scale
- GCSP:
-
Glasgow Coma Scale and Pupil responses
- ICP:
-
Intracranial Pressure
- CBF:
-
Cerebral Blood Flow
- ABG:
-
An Arterial Blood Analysis
- ICU:
-
Intensive Care Unit
- GOS:
-
Glasgow Outcome Scale
- SIBICC:
-
the Seattle International Severe Traumatic Brain Injury Consensus Conference
- BMI:
-
Body Mass Index
- APECHE II:
-
Acute Physiology and Chronic Health Evaluation II
- AIS:
-
Highest Ais Evaluation
- ISS:
-
Injury Severity Score
- GCSP-L:
-
Glasgow Coma Scale, Pupil responses and Arterial Lactate Concentration
- ROC:
-
Receiver Operating Characteristic Curve
- AUC:
-
the Area under Receiver Operating Characteristic Curve
- ICH:
-
Intracranial Hemorrhage
- SDH:
-
Subdural Hemorrhage
- EDH:
-
Epidural Hemorrhage
References
Malekahmadi M, Shadnoush M, Islam SMS, Shirvani A, Pahlavani N, Gholizadeh Navashenaq J, et al. The effect of French maritime pine bark extract supplementation on inflammation, nutritional and clinical status in critically ill patients with traumatic brain injury: a randomized controlled trial. Phytother Res. 2021;35(9):5178–88.
Alashram AR, Padua E, Romagnoli C, Annino G. Hyperbaric oxygen therapy for cognitive impairments in patients with traumatic brain injury: a systematic review. Appl Neuropsychol Adult. 2022:1–12. Online ahead of print. https://doi.org/10.1080/23279095.2022.2041418.
Brennan PM, Murray GD, Teasdale GM. Simplifying the use of prognostic information in traumatic brain injury. Part 1: the GCS-pupils score: an extended index of clinical severity. J Neurosurg. 2018;128(6):1612–20.
Reith FCM, Lingsma HF, Gabbe BJ, Lecky FE, Roberts I, Maas AIR. Differential effects of the Glasgow coma scale score and its components: an analysis of 54,069 patients with traumatic brain injury. Injury. 2017;48(9):1932–43.
Carteron L, Solari D, Patet C, Quintard H, Miroz JP, Bloch J, et al. Hypertonic lactate to improve cerebral perfusion and glucose availability after acute brain injury. Crit Care Med. 2018;46(10):1649–55.
Svedung Wettervik T, Engquist H, Howells T, Rostami E, Hillered L, Enblad P, et al. Arterial lactate in traumatic brain injury - relation to intracranial pressure dynamics, cerebral energy metabolism and clinical outcome. J Crit Care. 2020;60:218–25.
Bouzat P, Sala N, Suys T, Zerlauth JB, Marques-Vidal P, Feihl F, et al. Cerebral metabolic effects of exogenous lactate supplementation on the injured human brain. Intensive Care Med. 2014;40(3):412–21.
Hawryluk GWJ, Aguilera S, Buki A, Bulger E, Citerio G, Cooper DJ, et al. A management algorithm for patients with intracranial pressure monitoring: the Seattle international severe traumatic brain injury consensus conference (SIBICC). Intensive Care Med. 2019;45(12):1783–94.
Cheong Y, Lee S, Lee DK, Kim KS, Sang BH, Hwang GS. Preoperative hyperlactatemia and early mortality after liver transplantation: selection of important variables using random forest survival analysis. Anesth Pain Med (Seoul). 2021;16(4):353–9.
Boumezbeur F, Petersen KF, Cline GW, Mason GF, Behar KL, Shulman GI, et al. The contribution of blood lactate to brain energy metabolism in humans measured by dynamic 13C nuclear magnetic resonance spectroscopy. J Neurosci. 2010;30(42):13983–91.
Yang C, Lang L, He Z, Hui J, Jiang J, Gao G, et al. Epidemiological characteristics of older patients with traumatic brain injury in China. J Neurotrauma. 2022;39:850–9.
Chico-Fernández M, Abelardo Barea-Mendoza J, Servià-Goixart L, Ormazabal-Zabala T, Quintana-Díaz M, González-Robledo J, et al. Factors associated with death due to trauma in patients with a Glasgow coma scale score of 3 and bilateral fixed dilated pupils. Emergencias. 2021;33(2):121–7.
Lu W, Jiang C, Wang Z, Chen Y, Bai R, Yan G, et al. Lactic acid, neuron-specific enolase, and blood-brain barrier index after a severe traumatic brain injury: a prospective study. Br J Neurosurg. 2020:1–5.
Lozano A, Franchi F, Seastres RJ, Oddo M, Lheureux O, Badenes R, et al. Glucose and lactate concentrations in cerebrospinal fluid after traumatic brain injury. J Neurosurg Anesthesiol. 2020;32(2):162–9.
Stefani MA, Modkovski R, Hansel G, Zimmer ER, Kopczynski A, Muller AP, et al. Elevated glutamate and lactate predict brain death after severe head trauma. Ann Clin Transl Neurol. 2017;4(6):392–402.
Acknowledgements
None.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
YMW and JXZ performed the conceptualization and design of the work, statistical analysis, manuscript preparation, and the critical revision of the content. YMW, ZZ, YMZ, RS and HLL performed data collection and data analysis. All authors revised and approved the submitted manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The retrospective study was approved by the Ethics Committee of Beijing Tiantan Hospital, and this study was conducted in accordance with the principles of the declaration of Helsinki standards. Patient consent was waived by the institutional review board because of its retrospective nature and minimal risk for patients.
Consent for publication
Not applicable.
Competing interests
None of the authors has declared a conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, YM., Zhu, N., Zhou, YM. et al. The combination of arterial lactate level with GCS-pupils score to evaluate short term prognosis in traumatic brain injury: a retrospective study. BMC Neurol 22, 430 (2022). https://doi.org/10.1186/s12883-022-02970-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-022-02970-1