
Abstract
Background
We examined in persons with type 2 diabetes (T2D) whether the use of insulin and the risk of serious hypoglycemic events with insulin is higher in persons with more advanced CKD.
Methods
In a national cohort of 855,133 veterans with T2D seen at Veteran Affairs clinics between Jan 1, 2008 and December 31, 2010 with at least two serum creatinine measurements, we defined insulin use from pharmacy records and serious hypoglycemic events by ICD-9/10 codes from emergency room visits or hospitalizations that occurred until December 31, 2016.
Results
Mean age was 66 ± 11 years and 97% were men. Mean baseline eGFR was 73 ± 22 ml/min/1.73 m2. In a multivariable Cox regression model of those without insulin use at baseline (N = 653,200), compared to eGFR ≥90 group, eGFR < 30 group had higher hazard (HR 1.80, 95% CI 1.74 to 1.88) of subsequent insulin use. In a multivariable Cox model with propensity score matching for baseline insulin use (N = 305,570), both insulin use (HR 2.34, 95% CI 2.24 to 2.44) and advanced CKD (HR 2.28, 95% CI 2.07 to 2.51 for comparison of eGFR < 30 to eGFR ≥90 ml/min/1.73 m2 groups) were associated with increased risk of subsequent serious hypoglycemic events.
Conclusions and relevance
In T2D, more advanced CKD was associated with greater insulin use. Both insulin use and advanced CKD were risk factors for serious hypoglycemic events. The safety of insulin compared to newer glycemic agents in more advanced CKD needs further study.
Similar content being viewed by others


Background
There are more than 30 million adults with diabetes mellitus (DM) in the United States [1]. Diabetes is the leading cause of chronic kidney disease (CKD) with almost 1 in 3 persons with diabetes developing kidney disease [2]. Despite the public health importance of kidney disease in persons with type 2 diabetes (T2D), there is a paucity of data on optimal treatment for glycemic control in this population [3]. Fundamental questions such as the role of insulin in glycemic control in CKD still need to be addressed.
It is often considered that insulin requirements go down with advanced CKD as insulin is cleared by the kidney [3,4,5]. However, cross-sectional studies suggest higher insulin use in persons with more advanced CKD [6,7,8]. Therefore, it remains unclear whether the need for insulin is decreased or increased in advanced CKD.
A serious adverse effect of insulin therapy is hypoglycemia that results in emergency room visit or hospitalization. While insulin therapy is a known risk factor for hypoglycemic episodes [10], whether advanced CKD by itself is associated with increased risk of hypoglycemia has been controversial. The incidence of hypoglycemia defined as blood glucose < 70 mg/dl was higher in those with more advanced CKD in a study of veterans [9]. However, a prospective observational study of individuals with T2D using continuous glucose monitors found that hypoglycemia was common in persons with moderate to severe CKD but was not more common than in those with preserved GFR [9]. The question of whether both insulin use and advanced CKD are independently associated with increased risk of hypoglycemia may have therapeutic implications for glycemic control in persons with T2D and CKD as hypoglycemic episodes are associated with increased risk of CKD progression [10], stroke [11] and mortality [12, 13].
Therefore, in the current study we examined the hypothesis that requirement for insulin for glycemic control in T2D is lower in those with advanced CKD. We also examined whether the incidence of serious hypoglycemic episodes is greater in those with more advanced CKD and augmented in those with more advanced CKD on insulin.
Materials and methods
Patient population
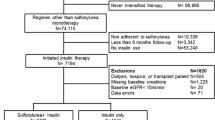
This was an observational study of veterans in the United States with an encounter in the Veteran Affairs (VA) system corresponding to a diagnosis of T2D between January 1, 2008 and December 31, 2010, and who had at least two outpatient serum creatinine measurements during the same time-period. The index date was defined as the date of the second outpatient serum creatinine value. Among the 1,187,700 veterans with T2DM and two outpatient serum creatinine measurements, the analytic cohort (N = 855,135) included those with non-missing data for demographics, blood pressure, body mass index (BMI) and hemoglobin A1C (HbA1c) and VA pharmacy prescription fill data (Fig. 1). This study was conducted with approval from the University of Utah Institutional Review Board as well as in accordance to the Declaration of Helsinki.

Flow diagram of study cohort
Data source and covariates
We used the VA Informatics and Computing Infrastructure (VINCI) [14] platform to access the national VA data. Age (defined at index date), gender and race were obtained from the VA Corporate Data Warehouse (CDW) [15] data. Diagnosis of T2D was defined by International Classification of Disease (ICD-9) codes (Supplemental Table 1) recorded between 1/1/2008 to 12/31/2010 in VA Inpatient and Outpatient Medical SAS Datasets [16, 17]. While we required an ICD-9 diagnostic code of T2D mellitus to minimize the inclusion of type 1 diabetes mellitus in the study cohort, duration of T2D was calculated by the first occurrence of ICD-9 code for T2D, hemoglobin A1C > 6.5% or use of anti-diabetic medications from Oct 1, 1999 to the index date. Baseline comorbidities included coronary artery disease, congestive heart failure, cerebrovascular disease, peripheral vascular disease, lung disease and cancer. These were considered present if they were recorded in the VA Inpatient and Outpatient Medical SAS Datasets within 3 years prior to the index date. As the index date was defined by the second outpatient serum creatinine and the outpatient labs could be drawn either before or after a clinic visit, we used ±90 days window around the index date to capture clinic visits data such as blood pressures and weight. The first recorded outpatient systolic and diastolic blood pressures within 90 days of the index date were used. BMI was calculated using the first weight value recorded within 90 days of the index date and most recently recorded height value, not restricting to within the last 90 days. As HbA1c is measured only every 3 months (particularly in those not under good glycemic control) and even less frequently in clinical practice (particularly in those at glycemic control goal), we used ±180 days window around the index date to minimize missing HbA1c data.
Veterans’ prescription records [18] were used to identify baseline medication exposure of hypoglycemic agents, antihypertensive medications and statins. As many medications are commonly filled for 90 days, we applied ±90 days window around the index date to capture baseline medications. For baseline insulin use, we applied ±180 days window in order to minimize misclassification of new insulin use for those who might have missed filling their insulin in the 90 days window around the index date. Hypoglycemic agents were classified as insulin, sulfonylureas, metformin, thiazolidinedione (TZD) and other agents. Antihypertensive medications were classified as alpha-blockers, beta-blockers, calcium channel blockers, angiotensin converting enzyme inhibitors or angiotensin receptor blockers (ACEI/ARB), loop-diuretics and thiazide-type diuretics.
In the current analysis, we followed the veterans until death or the administrative censor date of December 31, 2016.
Prevalent and new insulin use
Prevalent insulin use was identified through review of the patient’s prescription data within 180 days of the index date. In those not on insulin at baseline, incidence of new insulin use was determined by the first time that the patient had a prescription for insulin after the index date.
Hypoglycemic episodes
We defined serious hypoglycemic events as those that needed medical attention as evidenced by an emergency room visit with a diagnosis of hypoglycemia and/or hospitalization with a primary discharge diagnosis of hypoglycemia codes. A previously validated definition [19, 20] was used to identify hypoglycemic events from ICD 9/10 codes from emergency room visits or hospitalizations that occurred from the index date until the censor date. (Supplemental Table 2).
Statistical analyses
Baseline characteristics of participants with and without insulin use were described by means and standard deviations or medians and interquartile ranges for numeric variables, and proportions for categorical variables.
Associations of eGFR categories with baseline and subsequent insulin use
In the entire analytic cohort (N = 855,133), we used a multivariable logistic regression model to relate baseline insulin use as the dependent variable to eGFR groups as the predictor variable, with eGFR ≥90 ml/min/1.73 m2 as the reference group. This model included adjustment for age, gender, race, coronary artery disease, stroke, peripheral vascular disease, congestive heart failure, lung disease, cancer, systolic and diastolic blood pressures, BMI, HbA1c, diabetes duration, use of ACE-Is or ARBs, sulfonylurea, metformin, TZDs, and other hypoglycemic agents.
In those not on insulin at baseline (N = 653,200), we used a multivariable Cox regression to estimate the association of subsequent, new insulin use by different eGFR groups with eGFR ≥90 ml/min/1.73 m2 as the reference. This model was adjusted for the same variables as above.
Associations of insulin use and eGFR categories with serious hypoglycemic events
To examine whether insulin use and eGFR categories were independently associated with serious hypoglycemic events, we first conducted a multivariable Cox regression analysis in the entire analytic cohort (N = 855,133) with the same covariates as above. To further reduce the risk of indication bias between veterans not on and on insulin use at baseline, we repeated the multivariable Cox regression model for serious hypoglycemia events in a propensity score matched cohort (N = 305,570). The propensity scores were generated by the above multivariable logistic regression model of baseline insulin as the dependent variable. The distribution of propensity scores was checked to ensure overlap between insulin use groups. We then used a Stata module (psmatch2) [21] to perform 1–1 matching by caliper without replacement on the estimated propensity scores between insulin use groups. Standardized mean differences in the covariates between the insulin use groups were evaluated before and after matching by examining a plot of the standardized mean differences across the covariates. There were no significant departures from balance following the application of propensity-score matching (maximum standardized difference = 4%).
In additional multivariable Cox regression analyses, we examined the joint associations of baseline insulin use and eGFR groups with serious hypoglycemic events using eGFR ≥90 and not on insulin as the reference group in the entire cohort (N = 855,133) and propensity score matched cohort (N = 305,570).
Statistical analysis was performed using Stata Version 15.1 (College Station, TX, USA).
Results
Of the 855,133 veterans that met the criteria for the current analysis, 653,200 (76.4%) were not on insulin at baseline. In general, those on insulin had longer duration of diabetes, higher A1C, higher BMI and lower use of metformin and sulfonylureas (Table 1). They also had higher comorbidity burden with higher prevalence of history of heart failure, coronary artery disease and stroke. The baseline eGFR was lower in those on insulin compared to those not on insulin (69 ± 25 versus 74 ± 21 ml/min/1.73 m2).
From the entire analytic cohort (N = 855,133), we derived propensity scores for baseline insulin use in a logistic regression model. In the propensity score matched cohort (N = 305,570), standardized % bias across covariates was close to zero (Supplemental Fig. 1) and baseline characteristics of those with (N = 152,785) and without insulin use (N = 152,785) at baseline was well balanced with propensity score matching (Table 1).
Associations of levels of eGFR with prevalent and incident insulin use
With adjustment for demographics, baseline comorbidities (listed in Table 1), blood pressures, BMI, duration of diabetes, HbA1C and medications, in a multivariable logistic regression model, compared to veterans with an eGFR of ≥90 ml/min/1.73 m2, a substantially higher percentage of veterans with stage 3A (odds ratio (OR) 1.56, 95% CI 1.53 to 1.59), stage 3B (OR 2.35, 95% CI 2.29 to 2.42) and stage 4/5 (OR 3.55, 95% CI 3.43 to 3.66) CKD used insulin at baseline (Fig. 2, Panel A).

Associations of eGFR groups with baseline insulin use in the entire cohort in a logistic regression model (N = 855,133) and subsequent new insulin use in those without baseline insulin use (N = 653,200) in a Cox regression model
In those without insulin use at baseline (N = 653,200), there were 157,108 persons who needed insulin over 3,870,219 years of follow-up with an event rate of 4.0/100-person years of follow-up. In a Cox regression model adjusted for the above covariates, compared to veterans with an eGFR of ≥90 ml/min/1.73 m2, veterans with stage 3A (hazards ratio (HR) 1.31, 95% CI 1.28 to 1.33), stage 3B (HR 1.59, 95% CI 1.56 to 1.63) and stage 4/5 (HR 1.80, 95% CI 1.74 to 1.87) CKD had substantially higher new insulin use during follow-up (Fig. 2, Panel B).
Associations of baseline insulin use and levels of eGFR with subsequent serious hypoglycemic episodes
The incidence of serious hypoglycemic events in veterans with T2D not on insulin (0.21%, 9435 events, 4,460,465 years of follow-up) was lower compared to those on insulin (0.84%, 10,558 events 1,257,904 years of follow-up). Kaplan-Meier curves showed that these differences persisted across different stages of CKD (Fig. 3).

Kaplan-Meier curves for probability of serious hypoglycemic event by insulin and eGFR groups
In the entire analytic cohort (N = 855,133), in a multivariable Cox regression model adjusted for demographics, duration of diabetes, comorbidities, blood pressures, BMI, HbA1C, diabetes medications and use of ACE-I/ ARB, insulin use (HR 2.44, 95% CI 2.36 to 2.53) and more advanced CKD (HR 2.43, 95% CI 2.27 to 2.59 for comparison of eGFR < 30 versus ≥90 ml/min/1.73 m2 group) were both associated with increased risk of serious hypoglycemic events (Fig. 4, panel A). In a multivariable Cox regression model in the propensity score matched cohort (N = 305,570), the corresponding hazard ratios for hypoglycemic events for insulin use (HR 2.34, 95% CI 2.24 to 2.44) and more advanced CKD (HR2.28, 95% 2.07 to 2.51) were similar to that observed in the entire cohort (Fig. 4, panel B).

Individual associations of baseline insulin use and eGFR groups with serious hypoglycemic events in the entire cohort (N = 855,133) and propensity score matched cohort (N = 305,570)
Using those not on insulin with eGFR ≥90 ml/min/1.73 m2 as the reference group, those on insulin with eGFR < 30 ml/min/1.73 m2 had the highest risk of hypoglycemia (in the entire analytic cohort HR 5.62, 95% CI 5.19 to 6.09 and in the propensity score matched cohort HR 5.24, 95% CI 4.62 to 5.93) with the other groups having intermediate risks (Fig. 5, panels A and B).

Joint associations of baseline insulin use and eGFR groups with serious hypoglycemic events using eGFR ≥90 and not on insulin as the reference group in the entire cohort (N = 855,133) and propensity score matched cohort (N = 305,570)
Discussion
The main findings of this observational study are that insulin use was higher in more advanced CKD and that both insulin use and advanced CKD were independent risk factors for serious hypoglycemic events. Furthermore, compared to those with preserved kidney function and not on insulin, the risk of serious hypoglycemic events was nearly 5.3-fold higher in patients who used insulin and had eGFR < 30 ml/min/1.73 m2.
Previous literature suggests that because the kidney is responsible for the majority of exogenous insulin clearance, patients with diabetes and CKD and lower renal clearance rates have higher levels of serum insulin and may require less insulin than those without CKD [4, 5]. In contrast to this commonly held belief, the results of this study suggest that the need for insulin for glycemic control is inversely related to kidney function with a graded increase in baseline and subsequent insulin use with higher stages of CKD.
There are potential biological explanations for this observed finding. First, insulin resistance is common in CKD [22, 23], possibly related to pro-inflammatory cytokines such as interleukin-6 and tumor necrosis factor-⍺ [24] and oxidative stress [25,26,27] that are involved in intracellular mechanisms of insulin resistance [28,29,30,31,32,33]. Second, pancreatic beta-islet cells have low expression of antioxidant enzymes and because of this low antioxidant capacity, they are highly sensitive to oxidative stress [34,35,36]. Experimental data suggest that beta cell dysfunction might be worsened in CKD due to increased oxidative stress from the accumulation of uremic toxins [37]. Third, many of the anti-diabetic medications are contraindicated in advanced CKD [38,39,40]. Thus, this combination of decreased insulin production, peripheral insulin resistance and contraindications for other medications could increase the need for exogenous insulin for glycemic control in CKD.
There are also potential biological explanations for the associations of advanced CKD with higher risk of hypoglycemia. Renal gluconeogenesis plays an important role in countering hypoglycemia in healthy adults [41,42,43]. People with moderate to severe CKD have reduced kidney mass and therefore, a reduced capacity for glucose release from the kidneys [44] which might increase the risk for hypoglycemia. However, the previous data on whether CKD is a risk factor for hypoglycemia has been conflicting. Some of the previous studies noted such an association [45, 46] but not all [9].
We found not only that the need for insulin was higher in more advanced CKD but that CKD and insulin use are independent factors that contribute to the risk of a hypoglycemic event and that this risk was the highest in patients with advanced CKD on insulin. This finding is of clinical significance for therapeutic options for glycemic control in advanced CKD as hypoglycemia has been associated with higher risk of mortality, cardiovascular disease, cognitive impairment and progression of CKD [47,48,49,50]. A previous study noted that in patients hospitalized due to an acute kidney injury, hypoglycemic events were most common in insulin users [20]. The safety profile of insulin compared to newer glycemic agents such as SGLT-2 inhibitors and GLP-1 analogs in advanced CKD need to be further examined in randomized controlled trials to determine optimal glycemic control therapy in this population.
The major limitation of the current study is the observational nature of the analyses despite the use of propensity score matching as there may be residual confounding from unknown covariates that were not included in the development of propensity scores. While the definitions of hypoglycemia relied on data from electronic medical records is also a limitation, we used a previously validated definition [19, 20]. Even though, we used a large national database of veterans, it is possible that serious hypoglycemic events that were treated at non-VA medical were not captured. However, such underreporting will likely bias the study towards the null hypothesis and therefore, the currently reported results are likely conservative estimates of the associations of insulin use and advanced CKD with the risk of hypoglycemic events. Lastly, the study cohort was predominantly male (97%); future studies of hypoglycemia in both women and men are warranted.
Conclusions
In summary, contrary to widely held assumption that advanced CKD is associated with decreased need for insulin, we found that insulin use was greater in T2D patients with more advanced CKD. Furthermore, this study also found that both insulin use and CKD are independent factors for risk of hypoglycemia, with patients with advanced CKD who use insulin being at the highest risk for a hypoglycemic event. Future randomized controlled trials are needed to determine the safety of insulin compared to newer glycemic agents in patients with T2D and advanced CKD.
Availability of data and materials
The data that support the findings of this study are available from Veterans Affairs, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
Abbreviations
- DM:
-
Diabetes mellitus
- CKD:
-
Chronic kidney disease
- T2D:
-
Type 2 diabetes
- eGFR:
-
Estimated glomerular filtration rate
- VA:
-
Veterans Affairs
- BMI:
-
Body mass index
- HbA1C:
-
Hemoglobin A1C
- VINCI:
-
VA Informatics and Computing Infrastructure
- CDW:
-
VA Corporate Data Warehouse
- ICD:
-
International Classification of Disease
- TZD:
-
Thiazolidinedione
- ACEI:
-
Angiotensin converting enzyme inhibitors
- ARB:
-
Angiotensin receptor blocker
References
Center for Disease Control and Prevention: Division of Diabetes Translation At A Glance,. U. S Department of Health & Human Services 2020. (Accessed March 30, 2021, at https://www.cdc.gov/chronicdisease/resources/publications/aag/diabetes.htm.)
National Institute of Diabetes and Digestive and Kidney Diseases: Diabetic Kidney Disease. National Institutes of Health, 2017. (Accessed March 30, 2021, at https://www.niddk.nih.gov/health-information/diabetes/overview/preventing-problems/diabetic-kidney-disease.)
Tuttle KR, Bakris GL, Bilous RW, et al. Diabetic kidney disease: a report from an ADA consensus conference. Diabetes Care. 2014;37:2864–83.
Rabkin R, Ryan MP, Duckworth WC. The renal metabolism of insulin. Diabetologia. 1984;27:351–7.
Biesenbach G, Raml A, Schmekal B, Eichbauer-Sturm G. Decreased insulin requirement in relation to GFR in nephropathic type 1 and insulin-treated type 2 diabetic patients. Diabet Med. 2003;20:642–5.
Grandfils N, Detournay B, Attali C, et al. Glucose lowering therapeutic strategies for type 2 diabetic patients with chronic kidney disease in primary care setting in France: a cross-sectional study. Int J Endocrinol. 2013;2013:640632.
Busch M, Nadal J, Schmid M, et al. Glycaemic control and antidiabetic therapy in patients with diabetes mellitus and chronic kidney disease - cross-sectional data from the German chronic kidney disease (GCKD) cohort. BMC Nephrol. 2016;17:59.
Gor D, Gerber BS, Walton SM, Lee TA, Nutescu EA, Touchette DR. Antidiabetic drug use trends in patients with type 2 diabetes mellitus and chronic kidney disease: a cross-sectional analysis of the National Health and nutrition examination survey. J Diabetes. 2020;12:385–95.
Ahmad I, Zelnick LR, Batacchi Z, et al. Hypoglycemia in people with type 2 diabetes and CKD. Clin J Am Soc Nephrol. 2019;14:844–53.
Shih CJ, Wu YL, Lo YH, et al. Association of hypoglycemia with incident chronic kidney disease in patients with type 2 diabetes: a nationwide population-based study. Medicine (Baltimore). 2015;94:e771.
Yu TM, Lin CL, Chang SN, Sung FC, Kao CH. Increased risk of stroke in patients with chronic kidney disease after recurrent hypoglycemia. Neurology. 2014;83:686–94.
Kong AP, Yang X, Luk A, et al. Hypoglycaemia, chronic kidney disease and death in type 2 diabetes: the Hong Kong diabetes registry. BMC Endocr Disord. 2014;14:48.
Hsiao CC, Tu HT, Lin CH, Chen KH, Yeh YH, See LC. Temporal trends of severe hypoglycemia and subsequent mortality in patients with advanced diabetic kidney diseases transitioning to Dialysis. J Clin Med. 2019;8:420.
Health Services Research & Development, Veterans Affairs Informatics and Computing Infrastructure (VINCI). (Accessed May 12, 2021, at https://www.hsrd.research.va.gov/for_researchers/vinci/.)
Veteran Affairs Corporate Data Warehouse (CDW). (Accessed May 12, 2021, at https://www.hsrd.research.va.gov/for_researchers/vinci/cdw.cfm.)
VIReC Research User Guide; VHA Medical SAS Outpatient Datasets FY2006. Hines, IL: U.S. Department of Veterans Affairs. VA Information Resource Center 2007. 2007. (Accessed May 20, 2021, at https://vaww.virec.research.va.gov/RUGs/MedSAS/Archive/OP/RUG-MedSAS-OP-FY06-RA.pdf.)
VIReC Research User Guide; VHA Medical SAS Inpatient Datasets FY2006. Hines, IL: U.S. Department of Veterans Affairs. VA Information Resource Center 2007. 2007. (Accessed May 20, 2021, at https://vaww.virec.research.va.gov/RUGs/MedSAS/Archive/IP/RUG-MedSAS-IP-FY06-RA.pdf.)
US Department of Veterans Affairs, VA Information Resource Center (VIReC) VHA Pharmacy Prescription Data. 2nd Edition. Hines, IL: VIReC; 2008. VIReC Research User Guide 2008. (Accessed May 20, 2021, at https://vaww.virec.research.va.gov/RUGs/RUGs-Index.htm.)
Ginde AA, Blanc PG, Lieberman RM, Camargo CA Jr. Validation of ICD-9-CM coding algorithm for improved identification of hypoglycemia visits. BMC Endocr Disord. 2008;8:4.
Hung AM, Siew ED, Wilson OD, et al. Risk of hypoglycemia following hospital discharge in patients with diabetes and acute kidney injury. Diabetes Care. 2018;41:503–12.
Leuven E, Sianesi B. PSMATCH2: Stata Module to Perform Full Mahalanobis and Propensity Score Matching, Common Support Graphing, and Covariate Imbalance Testing. Version 300; 2003.
Kobayashi S, Maesato K, Moriya H, Ohtake T, Ikeda T. Insulin resistance in patients with chronic kidney disease. Am J Kidney Dis. 2005;45:275–80.
Nerpin E, Risérus U, Ingelsson E, et al. Insulin sensitivity measured with Euglycemic clamp is independently associated with glomerular filtration rate in a community-based cohort. Diabetes Care. 2008;31:1550–5.
Spoto B, Leonardis D, Parlongo RM, et al. Plasma cytokines, glomerular filtration rate and adipose tissue cytokines gene expression in chronic kidney disease (CKD) patients. Nutr Metab Cardiovasc Dis. 2012;22:981–8.
Wassmann S, Stumpf M, Strehlow K, et al. Interleukin-6 induces oxidative stress and endothelial dysfunction by overexpression of the angiotensin II type 1 receptor. Circ Res. 2004;94:534–41.
Kaneto H, Xu G, Fujii N, Kim S, Bonner-Weir S, Weir GC. Involvement of c-Jun N-terminal kinase in oxidative stress-mediated suppression of insulin gene expression*. J Biol Chem. 2002;277:30010–8.
Gassaway BM, Petersen MC, Surovtseva YV, et al. PKCε contributes to lipid-induced insulin resistance through cross talk with p70S6K and through previously unknown regulators of insulin signaling. Proc Natl Acad Sci. 2018;115:E8996–9005.
Senn JJ, Klover PJ, Nowak IA, Mooney RA. Interleukin-6 induces cellular insulin resistance in hepatocytes. Diabetes. 2002;51:3391–9.
Lagathu C, Bastard J-P, Auclair M, Maachi M, Capeau J, Caron M. Chronic interleukin-6 (IL-6) treatment increased IL-6 secretion and induced insulin resistance in adipocyte: prevention by rosiglitazone. Biochem Biophys Res Commun. 2003;311:372–9.
Feinstein R, Kanety H, Papa MZ, Lunenfeld B, Karasik A. Tumor necrosis factor-alpha suppresses insulin-induced tyrosine phosphorylation of insulin receptor and its substrates. J Biol Chem. 1993;268:26055–8.
Hotamisligil GS, Murray DL, Choy LN, Spiegelman BM. Tumor necrosis factor alpha inhibits signaling from the insulin receptor. Proc Natl Acad Sci U S A. 1994;91:4854–8.
Kanety H, Feinstein R, Papa MZ, Hemi R, Karasik A. Tumor necrosis factor α-induced phosphorylation of insulin receptor Substrate-1 (IRS-1): possible mechanism for suppression of insulin-stimulated tyrosine Phosporylation of IRS-1. J Biol Chem. 1995;270:23780–4.
Thomas SS, Dong Y, Zhang L, Mitch WE. Signal regulatory protein-α interacts with the insulin receptor contributing to muscle wasting in chronic kidney disease. Kidney Int. 2013;84:308–16.
Lenzen S, Drinkgern J, Tiedge M. Low antioxidant enzyme gene expression in pancreatic islets compared with various other mouse tissues. Free Radic Biol Med. 1996;20:463–6.
Tiedge M, Lortz S, Drinkgern J, Lenzen S. Relation between antioxidant enzyme gene expression and antioxidative defense status of insulin-producing cells. Diabetes. 1997;46:1733–42.
Drews G, Krippeit-drews P, Düfer M. Oxidative stress and beta-cell dysfunction. Pflugers Arch - Eur J Physiol. 2010;460:703–18.
Koppe L, Nyam E, Vivot K, et al. Urea impairs β cell glycolysis and insulin secretion in chronic kidney disease. J Clin Invest. 2016;126:3598–612.
Betônico CCR, Titan SMO, Correa-Giannella MLC, Nery M, Queiroz M. Management of diabetes mellitus in individuals with chronic kidney disease: therapeutic perspectives and glycemic control. Clinics (Sao Paulo). 2016;71:47–53.
Lubowsky ND, Siegel R, Pittas AG. Management of glycemia in patients with diabetes mellitus and CKD. Am J Kidney Dis. 2007;50:865–79.
Snyder RW, Berns JS. Reviews: use of insulin and Oral hypoglycemic medications in patients with diabetes mellitus and advanced kidney disease. Semin Dial. 2004;17:365–70.
Cersosimo E, Garlick P, Ferretti J. Renal substrate metabolism and gluconeogenesis during hypoglycemia in humans. Diabetes. 2000;49:1186–93.
Legouis D, Faivre A, Cippà PE, de Seigneux S. Renal gluconeogenesis: an underestimated role of the kidney in systemic glucose metabolism. Nephrol Dial Transplant. 2020;28:gfaa302.
Gerich JE, Meyer C, Woerle HJ, Stumvoll M. Renal gluconeogenesis: its importance in human glucose homeostasis. Diabetes Care. 2001;24:382–91.
Alsahli M, Gerich JE. Hypoglycemia, chronic kidney disease, and diabetes mellitus. Mayo Clin Proc. 2014;89:1564–71.
Busch M, Lehmann T, Wolf G, Günster C, Müller UA, Müller N. Antidiabetic therapy and rate of severe Hypoglycaemia in patients with type 2 diabetes and chronic kidney disease of different stages - a follow-up analysis of health insurance data from Germany. Exp Clin Endocrinol Diabetes. 2020;129:821-30.
Moen MF, Zhan M, Hsu VD, et al. Frequency of hypoglycemia and its significance in chronic kidney disease. Clin J Am Soc Nephrol. 2009;4:1121–7.
McCoy RG, Van Houten HK, Ziegenfuss JY, Shah ND, Wermers RA, Smith SA. Increased mortality of patients with diabetes reporting severe hypoglycemia. Diabetes Care. 2012;35:1897–901.
Davis SN, Duckworth W, Emanuele N, et al. Effects of severe hypoglycemia on cardiovascular outcomes and death in the veterans affairs diabetes trial. Diabetes Care. 2019;42:157–63.
Lee Y-L, Yen S-J, Shin S-J, Huang Y-C, He JS, Lin K-D. Severe hypoglycemia as a predictor of end-stage renal disease in type 2 diabetes: a National Cohort Study. Int J Environ Res Public Health. 2019;16:681.
Lacy ME, Gilsanz P, Eng C, Beeri MS, Karter AJ, Whitmer RA. Severe hypoglycemia and cognitive function in older adults with type 1 diabetes: the study of longevity in diabetes (SOLID). Diabetes Care. 2020;43:541–8.
Acknowledgements
The VA Informatics and Computing Infrastructure (VINCI) provided access to the national VA database, SQL, SAS and Stata programs. This study does not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Funding
Statistical analyses and preparation of this manuscript were funded by grants to SB from Veterans Administration Office of Rural Health (VA ORH-14398), National Institute of Diabetes, Digestive and Kidney Diseases (R01DK118219) and National Heart, Lung and Blood Institute (R21HL145494).
Author information
Authors and Affiliations
Contributions
DG was a major contributor in writing of the manuscript. GW and RB analyzed and interpreted the patient data. NA, NZ, VG, JC, and DS were contributors in writing and editing the manuscript. SB contributed to writing the manuscript and designing the research. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Research was conducted in accordance with the Declaration of Helsinki and has been approved by the University of Utah Institutional Review Board. We obtained a waiver of informed consent from the University of Utah Institutional Review Board because this study was a retrospective chart review.
Consent for publication
Not applicable.
Competing interests
There are no conflicts of interest for any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplemental Table 1.
ICD-9 codes used to define medical conditions. Supplemental Table 2. ICD-9/10 codes used to define hypoglycemic events. Supplemental Figure 1. Standardized % bias across covariates by baseline insulin use before and after propensity score matching.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Grube, D., Wei, G., Boucher, R. et al. Insulin use in chronic kidney disease and the risk of hypoglycemic events. BMC Nephrol 23, 73 (2022). https://doi.org/10.1186/s12882-022-02687-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-022-02687-w