
Abstract
Background
Intraductal papillary carcinoma (IDPC) is a rare but fatal disease. Preoperative ultrasound diagnosis of IDPC remains challenging and meaningful. The aim of the study was to determine an effective ultrasound model to predict intraductal papillary carcinoma (IDPC) in patients with partially cystic breast lesions on ultrasound.
Methods
We reviewed female patients with breast nodules who underwent biopsy or surgery between 2004 and 2019, and pathological results were used as the reference standard. We finally included 21 IDPC patients with partially cystic lesions on preoperative ultrasound matched to 40 patients with intraductal papilloma. The association of ultrasound features with IDPC was analysed.
Results
Posterior echo enhancement (P < 0.001), tumour size (P = 0.002), irregular shape (P = 0.003), wide base (P = 0.003), solid-mainly component (P = 0.013), rich Doppler flow (P < 0.001) and multiple lesions (P = 0.044) were associated with IDPC by univariate analysis. Based on univariate analysis, variables were included in the regression analysis to obtain independent factors. The regression analysis showed that microcalcification, multiple lesions, posterior echo enhancement, wide base of solid components and rich colour Doppler flow were predictors for IDPC (P < 0.001). The collective model of the independent factors (microcalcification, multiple lesions, posterior echo enhancement, wide base of solid components and rich colour Doppler flow) could predict IDPC with an area under the curve (AUC) of 0.99 (95% CI 0.95–1.00). The collective model had a better net benefit demonstrated by the decision curve.
Conclusion
Ultrasonic features may be an applicable model for predicting IDPC with partially cystic breast lesions on ultrasound and has a better potential to facilitate decision-making preoperatively.
Similar content being viewed by others


Background
Breast cancer incidence has increased during the past 2 decades [1]. Intraductal papillary carcinoma (IDPC) is rare, accounting for < 2–5% of breast cancer cases. Although the sample size of malignant ductal breast lesions is very narrow, identify patients with a high likelihood of IDPC ability could develop a more accurate surgical planning and reduce potential risks to patients and the overall health care costs.
Ultrasound (US) because of its cost-effectiveness, non-radiation and high sensitivity is widely used for prediction of breast cancer [2]. In the assessment of intraductal masses, US is more specific than mammography and magnetic resonance imaging (MRI), and may be considered as the selective manner [3,4,5,6]. However, intraductal masses lack the classical ultrasound features of malignancy, such as taller-than-wide shape, and irregular margins (infiltrative, microlobulated). IDPC has some similarities with other intraductal breast masses in imaging and clinical manifestations, especially for those with partially cystic lesions on ultrasound, which is difficult to diagnose clinically. For the breast imaging reporting and data system (BI-RADS) system, intraductal lesions are one of the “special cases”. It is unclear whether all detected by US should be classified as BI-RADS 4a because there is no clear clinical and radiological prediction of malignancy. Whether biopsy is needed for all intraductal masses is still in debate [7, 8]. Moreover, there are possibilities of false-negative results from biopsy procedures, and patients may experience inadequate resection in the first operation.
To the best of our knowledge, none of the studies has evaluated the US features of IDPC with partially cystic lesions. Except for intraductal papillary carcinoma (IDPC), there are previous papers analysing the ultrasound features of other malignant lesions of intraductal masses (including ductal carcinoma in situ and invasive ductal carcinoma). These ultrasound features include filling the duct more completely and involving more branch ducts [7, 9]. Herein, we evaluated the US features of IDPC with the pathological results obtained after surgery, aiming to explore an effective ultrasound model of identifying intraductal papillary carcinoma with partially cystic lesions on US preoperatively.
Methods
Patients
We retrospectively studied female patients with breast nodules who underwent excisional biopsy or surgery between January 2004 and October 2019 at our centre. The final pathologic results were considered the diagnostic gold standard. A total of 99 patients were diagnosed with intraductal papillary carcinoma based on pathological examination with WHO classification in our centre. The following criteria were applied: (1) partially cystic lesions on preoperative ultrasound (solid lesions were excluded, N = 69); (2) patients younger than 18 years of age were excluded (N = 1); (3) patients who received treatments before surgery were excluded (N = 2); and (4) patients who had a history of breast cancer in the previous study were removed (N = 6). A total of 21 lesions from 21 patients were included. Using the same database who underwent excisional biopsy or surgery during the same period, patients with intraductal papilloma were enrolled as a control group. Patients who met the exclusion criteria were excluded. An age-matched control group comprising 40 lesions from 40 patients was randomly selected.
Breast US examination
All US examinations were performed with Phillips HDI 5000, IU 22 (Philips Healthcare, Eindhoven, Netherlands), GE Logiq 9 or Logiq 7 (GE Healthcare, Milwaukee, WI, USA) devices equipped with either a 5–12 MHz or an 8–15 MHz linear-array transducer. US was performed by radiologists in our centre before surgery or biopsy, and US images were retrospectively evaluated by two radiologists who were experienced in breast US and were blinded to the patient clinical data for the study (staff radiologists with 8 and 12 years of experience). In cases involving a discrepancy between the assessments, a consensus was reached after discussion. The tumour size, tumour shape of solid component, single/multiple lesions, echogenicity of solid component, component (cyst-mainly or solid-mainly), homogeneity (homogeneity or heterogeneity), base of solid components (wide-basement or acute angle), presence of duct ectasia, posterior echo enhancement and microcalcifications were evaluated by B-mode US. Vascularity was classified as 4 patterns (no flow, minimal, moderate, or marked) by colour Doppler flow [10]. In cases involving a discrepancy between the assessments, a consensus was reached after discussion.
Statistical analysis
Categorical variables were presented as frequencies, and analyzed using the chi-squared test. Quantitative data were presented as the mean ± standard deviation (SD), and analyzed using the Mann–Whitney U test or the unpaired t-test. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy was calculated according to the pathological findings. Cutoff value of the model was determined according to the ROC (receiver operating characteristic). Based on the parameters from the statistically significant results of univariate analysis, a multivariate logistic regression model was established. Decision curve analysis of the case–control study was carried out to compare the clinical applicability of different models. All statistical analyses were performed with SPSS software version 19.0 (Chicago, IL, USA) and R version 3.5.0 (R Foundation for Statistical Computing, www.R-project.org). Differences with P < 0.05 were considered statistically significant.
Result
Sonographic features of PTC patients with partially cystic intraductal papillary carcinoma
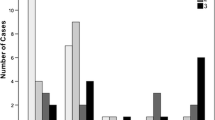
The correlation of US and clinical features between partially cystic IDPC and partially cystic intraductal papilloma is shown in Table 1. There were significant differences in tumour size (P = 0.002), tumour shape of solid components (P = 0.003), single/multiple lesions (P = 0.044), posterior echo enhancement (P < 0.001), component (P = 0.013), wide base of solid components (P = 0.003) and colour Doppler flow (P < 0.001) between the malignant and benign groups [Fig. 1]. However, microcalcification, homogeneity, echogenicity, and the presence of duct ectasia were not associated with IDPC (P > 0.05) [Table 1].

A breast masse from a young woman with intraductal papilloma. B-mode ultrasound showed a 2.0-cm narrow-base hypoechoic mass. The colour Doppler ultrasound image of the same mass reveals internal and peripheral blood flow signals (A,B). A breast masse from a young woman with intraductal papillary carcinoma, B-mode ultrasound showed a 0.9-cm wide-base hypoechoic mass. The colour Doppler ultrasound image of the same mass reveals internal and peripheral blood flow signals (C,D)
Diagnostic performance of the ultrasound characteristics
Among all the sonographic factors, receiver operating curve (ROC) analysis showed that posterior echo enhancement, tumour size (> 2 cm), irregular shape, wide base, and CDFI level are significant predictive factors for the diagnosis of IDPC. For the diagnosis of IDPC, the sensitivity, specificity, PPV, NPV, accuracy and AUC of posterior echo enhancement were 95.2%, 62.5%, 57.1%, 96.2%, 73.7% and 0.79 (95% CI 0.68–0.89), respectively. The sensitivity, specificity, PPV, NPV, accuracy and AUC of tumour size (> 2 cm) were 47.6%, 87.5%, 66.7%, 87.5%, 73.8% and 0.68 (95% CI 0.53–0.83), respectively. The sensitivity, specificity, PPV, NPV, accuracy and AUC of the irregular shape of solid components were 66.7%, 72.5%, 56.0%, 80.6%, 70.5% and 0.70 (95% CI 0.55–0.84), respectively. The sensitivity, specificity, PPV, NPV, accuracy and AUC of wide base solid components were 90.5%, 97.5%, 95.0%, 95.1%, 95.1% and 0.94 (95% CI 0.86–1.00), respectively. The sensitivity, specificity, PPV, NPV, accuracy and AUC of the CDFI level were 57.1%, 77.5%, 57.1%, 77.5%, 70.5% and 0.67 (95% CI 0.53–0.82), respectively [Table 2].
Diagnostic performance of the sonographic prediction of partially cystic intraductal papillary carcinoma
Based on univariate analysis, variables were included in the logistic regression analysis. Microcalcification, multiple lesions, posterior echo enhancement, wide base of solid components and rich colour Doppler flow were found to be independent factors. The malignant group was more likely to have tumours with microcalcification (X1, P < 0.001), posterior echo enhancement (X2, P < 0.001), wide base of solid components (X3, P < 0.001) and rich colour Doppler flow (X4, P < 0.001), and multiple lesions (X5, P < 0.001). The multivariate regression model was established as follows: Y = -69.05 + 18.61 * X1 + 17.01 * X2 + 52.73 * X3 + 17.91 * X4 + 33.43 * X5.
Factors including microcalcification, multiple lesions, posterior echo enhancement, wide base of solid components and rich colour Doppler flow were finally involved in the collective model. The collective model could predict malignancy with an AUC of 0.99 (95% CI 0.95–1.00) [Fig. 2]. The decision curve showed that the collective model had a better net benefit with a wider range of threshold probabilities [Fig. 3].

Receiver operating curve (ROC) analysis for the prediction models of intraductal papillary carcinoma

Decision curve analysis of the collective model including risk factors for microcalcification, multiple lesions, posterior echo enhancement, wide base of solid components and rich colour Doppler flow
Discussion
In this study, aiming to analyse the ultrasound features of IDPC lesions, we compared the US features between IDPC and intraductal papilloma. A collective model (including microcalcification, multiple lesions, posterior echo enhancement, wide base of solid components and rich colour Doppler flow) was proposed as a reference for patient diagnosis. The collective model could predict malignancy with an AUC of 0.99 (95% CI 0.95–1.00). The collective model had a better net benefit demonstrated by the decision curve.
On the basis of the results of the present study, the partially cystic IDPC showed several differences from the known malignant sonographic features of solid breast nodules [11]. The findings of this study showed that hypoechogenicity was observed in 37 (92.5%) benign and 17 (81.0%) malignant groups. Therefore, hypoechogenicity was considered unhelpful in the differentiation of partially cystic IDPC from benign IDPC. In the study, microcalcifications and rich colour Doppler flow within the solid component of partly cystic lesions are considered the US features that raise the likelihood of IDPC. 3/21 IDPC had microcalcification on breast sonography, and there was only one microcalcification in the intraductal papilloma group. Twelve of 21 IDPCs had rich colour Doppler flow on breast sonography, and 9/40 with intraductal papilloma had rich colour Doppler flow. Similarly, colour Doppler ultrasound and microcalcifications are helpful for distinguishing between benign and malignant breast lesions [12, 13]. In BI-RADS Fifth Edition, microcalcification and colour Doppler flow imaging features are also important US characteristics of breast lesions to consider when stratification a nodule [11]. Since none of the studies has evaluated the US features of IDPC with partially cystic lesions, we found that traditional US features, such as microcalcifications and rich colour Doppler flow, are still helpful.
For diagnosing IDPC, the sensitivity, specificity, PPV, NPV, accuracy and AUC of a wide base of solid components were 90.5%, 97.5%, 95.0%, 95.1%, 95.1% and 0.94 (95% CI 0.86–1.00), respectively, which indicated good diagnostic value. Previous studies showed that the solid component of papilloma usually presents as a focal mass arising from the ductal wall, with a relatively narrow base for attachment [10, 14]. In our study, the component of intraductal papilloma was identified to have a narrow base arising from the wall. The wide or narrow base configuration means an acute angle or blunt angle, depending on the angle degree between the solid component and the adjacent cyst wall on real-time sonography. A previous study also showed that malignant intraductal masses tended to fill the duct more completely [7]. In total, 19/21 IDPCs had a wide base of the solid component on US, but only one lesion (1/40) had a wide base in the intraductal papilloma group. This may be due to the intracystic components of carcinomas requiring multiple vascular poles emerging from the base of the papillary projections [15].
In a previous study, posterior acoustic shadowing of a solid mass was suggestive of invasive carcinoma, but this feature is not a reliable indicator for malignancy [11, 14]. Unlike in these retrospective studies, the results of this study showed that posterior echo enhancement of a partially cystic mass increased the risk of IDPC. To our knowledge, there has been no other study on the diagnostic efficacy of posterior echo shadowing for partially cystic IDPC. This result may be explained by the fact that compared with the surrounding normal tissue, some tumours have a uniform internal structure. When close to the normal tissue, the boundary of the tissue is obvious, so repeated reflections occur, and the posterior echo is enhanced.
Malignancy rates of complex cystic and solid breast lesions contain 0.3%–50%, as reported in previous studies [16]. A range of malignant pathologic results has been detected, and the most common malignancies include intraductal carcinoma in situ (DCIS), invasive ductal carcinoma (IDC), intraductal papillary carcinoma (IDPC) [7, 16]. US appearance of DCIS are nonspecific. Calcified DCIS most commonly manifests as echogenic foci located within a mass or duct, associated with internal microlobulations, or distributed in a branch pattern. Noncalcified DCIS may manifest as a hypoechoic mass with microlobulated margins and no posterior acoustic features, or it may have a “pseudomicrocystic” appearance. Harmonic imaging and coronal reconstruction may improve the detection of noncalcified DCIS [17]. The typical US appearance of IDC was irregular hypoechoic lesions with microcalcification, and it may have posterior echo attenuation [18].
There are several limitations to our study. First, different radiologists performed the primary ultrasound examinations, which may lead to interobserver differences. Second, our study included a small number of patients with intraductal papillary carcinoma, and further studies with a larger patient population and prospective inclusion of intraductal masses with subjective criteria are needed to confirm our findings. Finally, only colour Doppler sonography was used to evaluate the vascularity of breast lesions.
Conclusions
The ultrasound characteristics of partially cystic IDPC lesions included microcalcification, multiple lesions, posterior echo enhancement, wide base of solid components and rich colour Doppler flow. A collective model of all combinations of was highly reliable and careful correlation in terms of these sonographic features is needed. With improved technology, recognizing the US features of DCIS will become increasingly important for the detection of early-stage breast cancer.
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CDFI:
-
Colour Doppler flow imaging
- ROC:
-
Receiver operating curve
- IDPC:
-
Intraductal papillary carcinoma
- BI-RADS:
-
Breast imaging reporting and data system
- MRI:
-
Magnetic resonance imaging
- US:
-
Ultrasound
- AUC:
-
Area under the curve
- PPV:
-
Positive predictive value
- NPV:
-
Negative predictive value
- SD:
-
Standard deviation
References
Fan L, Strasser-Weippl K, Li JJ, St Louis J, Finkelstein DM, Yu KD, Chen WQ, Shao ZM, Goss PE. Breast cancer in China. Lancet Oncol. 2014;15:e279–89.
Guo R, Lu G, Qin B, Fei B. Ultrasound imaging technologies for breast cancer detection and management: a review. Ultrasound Med Biol. 2017. https://doi.org/10.1016/j.ultrasmedbio.2017.09.012.
Park CJ, Kim EK, Moon HJ, Yoon JH, Kim MJ. Reliability of breast ultrasound BI-RADS final assessment in mammographically negative patients with nipple discharge and radiologic predictors of malignancy. J Breast Cancer. 2016;19:308–15.
Kim H, Kang BJ, Kim SH, Lee JM. Second-look breast ultrasonography after galactography in patients with nipple discharge. Med Ultrason. 2020;22:58–64.
Yoon H, Yoon JH, Kim EK, Moon HJ, Park BW, Kim MJ. Adding ultrasound to the evaluation of patients with pathologic nipple discharge to diagnose additional breast cancers: preliminary data. Ultrasound Med Biol. 2015;41:2099–107.
Shen S, Zhou Y, Xu Y, Zhang B, Duan X, Huang R, Li B, Shi Y, Shao Z, Liao H, Jiang J, Shen N, Zhang J, Yu C, Jiang H, Li S, Han S, Ma J, Sun Q. A multi-centre randomized trial comparing ultrasound vs mammography for screening breast cancer in high-risk Chinese women. Br J Cancer. 2015;112:998–1004.
Kim WH, Chang JM, Moon WK, Cho N, Yi A, Koo HR, Kim SJ. Intraductal mass on breast ultrasound: final outcomes and predictors of malignancy. AJR Am J Roentgenol. 2013;200:932–7.
El Sheikh H, Almetaher HA, Abdalla HS, Shareef MM. Intraductal breast masses: Sonographic and mammographic predictors of malignancy. Egypt J Radiol Nuclear Med. 2015;46:S0378603X15001400.
Ganesan S, Karthik G, Joshi M, Damodaran V. Ultrasound spectrum in intraductal papillary neoplasms of breast. Br J Radiol. 2014;79:843–9.
Japan Association of Breast and Thyroid Sonography. Guideline for breast ultrasound management and diagnosis. 2nd ed. Tokyo: Nankodo Co.; 2008. p. 104–5.
American College of Radiology. Breast imaging reporting and data system. Breast imaging atlas. 5th ed. Reston, VA: Author; 2013.
Machado P, Eisenbrey JR, Stanczak M, Cavanaugh BC, Zorn LM, Forsberg F. Ultrasound detection of microcalcifications in surgical breast specimens. Ultrasound Med Biol. 2018;44:1286–90.
Watanabe T, Kaoku S, Yamaguchi T, Izumori A, Konno S, Okuno T, Tsunoda H, Ban K, Hirokaga K, Sawada T, Ito T, Nakatani S, Yasuda H, Tsuruoka M, Ueno E, Tohno E, Umemoto T, Shirakawa T. Multicentre prospective study of colour Doppler ultrasound for breast masses: utility of our colour Doppler method. Ultrasound Med Biol. 2019;45:1367–79.
Brooks MJ, Bourke AG. Radiological appearances of papillary breast lesions. Clin Radiol. 2008;63:1265–73.
Kato K, Nogi H, Ohta T, Kamio M, Toriumi Y, Nakata N, Uchida K, Miyamoto Y, Takeyama H. Usefulness of contrast-enhanced ultrasonography for intracystic breast tumours: a report of three cases. J Med Ultrason. 2014;41:389–96.
Kulali F, Guner G. Outcomes in sonographically categorized complex cystic breast lesions. J Ultrasound Med. 2022;41:2071–7.
Wang LC, Sullivan M, Du H, Feldman MI, Mendelson EB. US appearance of ductal carcinoma in situ. Radiographics. 2013;33:213–28.
Pointon KS, Cunningham DA. Ultrasound findings in pure invasive lobular carcinoma of the breast: comparison with matched cases of invasive ductal carcinoma of the breast. Breast. 1999;8:188–90.
Acknowledgements
Not applicable.
Funding
This study was supported by a grant from the CAMS Innovation Fund for Medical Sciences (2018-I2M-3-003), Peking Union Medical College Hospital (0104170) and National Natural Science Foundation of China (82171967). The funding bodies played no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
LYG carried out the selection and collection of samples, performed the statistical analysis, and drafted the manuscript. YXJ and JCL conceived of the study, participated in its design. XJL and JZ participated in the study design, carried out the identification of complex performed the statistical analysis, and review the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This retrospective study was approved by the Ethics Committee of Peking Union Medical College Hospital. The requirement for informed consent was waived by the Ethics Committee of Peking Union Medical College Hospital because of the retrospective nature of the study. We confirmed that all methods were performed in accordance with the relevant guidelines and regulations (For example: Declarations of Helsinki). The Ethics Committee of Peking Union Medical College Hospital granted permission to access the clinical/personal patient data used in the research.
Consent for publish
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gao, L., Lai, X., Zhang, J. et al. Sonographic prediction of intraductal papillary carcinoma with partially cystic breast lesions. BMC Med Imaging 23, 3 (2023). https://doi.org/10.1186/s12880-022-00934-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12880-022-00934-y