
Abstract
Background
Identifying how persons with dementia experience lived space is important for enabling supportive living environments and creating communities that compensate for the fading capabilities of these persons. Several single studies have explored this topic; however, few studies have attempted to explicitly review and synthesize this research literature. The aim of this systematic meta-synthesis was therefore to interpret and synthesize knowledge regarding persons with dementia’s experience of space.
Methods
A systematic, computerized search of AgeLine, CINAHL Complete, Embase, Medline and PsycINFO was conducted using a search strategy that combined MeSH terms and text words for different types of dementia with different descriptions of experience. Studies with 1) a sample of persons with dementia, 2) qualitative interviews as a research method and 3) a description of experiences of lived space were included. The search resulted in 1386 articles, of which 136 were identified as eligible and were read and assessed using the CASP criteria. The analysis was inspired by qualitative content analyses.
Results
This interpretative qualitative meta-synthesis included 45 articles encompassing interviews with 672 persons with dementia. The analysis showed that living in one’s own home and living in long-term care established different settings and posed diverse challenges for the experience of lived space in persons with dementia. The material revealed four main categories that described the experience of lived space: (1) belonging; (2) meaningfulness; (3) safety and security; and (4) autonomy. It showed how persons with dementia experienced a reduction in their lived space due to the progression of dementia. A comprehensive understanding of the categories led to the latent theme: “Living with dementia is like living in a space where the walls keep closing in”.
Conclusion
This meta-synthesis reveals a process whereby lived space gradually becomes smaller for persons with dementia. This underscores the importance of being aware of the experiences of persons with dementia and the spatial dimensions of their life-world. To sustain person-centred care and support the preservation of continuity and identity, one must acknowledge not only the physical and social environment but also space as an existential experience for persons with dementia.
Similar content being viewed by others


Background
Living with dementia involves enduring the loss of several mental and physical abilities [1], which leads to difficulties in handling everyday living [2], maintaining meaningful activities [3] and taking part in social life [4, 5]. Globally, at least 46.8 million people are living with dementia, and the number is rapidly rising [6]. As dementia is the leading cause of dependency and frailty among older people, delivering sufficient care services for persons with dementia constitutes one of the greatest challenges within health care systems [7].
Shifts in the perspectives of dementia care are urgently needed; this includes a shift in focus from symptoms and the disability and towards the capacities and potential of persons with dementia and their families [8, 9]. The World Health Organization’s “age-friendly” policy movement [10] and dementia awareness campaign [7] remind the general public of the importance of empowering persons with dementia to remain autonomous and active citizens of society. Understanding how persons with dementia experience the spatial dimensions of their day-to-day experiences of living with dementia is therefore important. This is necessary to both enable supportive living environments and create communities that compensate for the fading abilities of persons with dementia and allow them to maintain a meaningful life [9, 11]. Dutch philosopher Max Van Manen [12] described lived space as one of four existential attributes that he believed could guide reflections regarding the constitution of people’s lifeworld. These four attributes are (1) lived body, (2) lived others, (3) lived time, and (4) lived space. He conceptualized lived space as felt space and as a category for inquiring into the ways in which people experience the spatial dimensions of their daily experiences [12]. Thus, lived space, as conceptualized in this review, is more than the spatial characteristics of space and its geographies; it is also related to the feeling of being home or the conceptualization of “being in place” [13,14,15]. It refers to the meaning of space in relation to the experiences of living with dementia.
Because of the magnitude of its consequences, dementia is a syndrome that often requires individual care approaches and facilitated living environments [16]. Growing evidence suggests that housing- and environmental-design, in combination with psychosocial interventions, may have a positive impact on the functional level and quality of life of people with dementia [17,18,19]. These types of facilitating approaches are often described in the research literature and in policy documents through the concept of dementia-friendly or dementia-capable environments [20,21,22,23]. Person-centred care is commonly referred to as an important care approach [1, 24] that may promote this type of sustaining environment. Individualized care, recognition of the perspectives of the person with dementia, and the creation of social environments that support the well-being of the person are viewed as important cornerstones of person-centred care [25]. Although person-centred care has valuably influenced the development of dementia care, scholars have also called for more emphasis on how the physical and social environment can be adapted to support the preservation of continuity and identity for persons with dementia [26, 27].
Among the central principals for the design of dementia-friendly environments are safety and security, simplicity, good structure, and familiarity [11, 18, 28, 29]. Simple, structured and familiar environments may support wayfinding [21, 29,30,31]. The concept of familiarity refers to predictability and continuity; it is also important for creating a sense of being at home for persons with dementia in addition to supporting the maintenance of their social relationships, identity, autonomy and privacy [11, 32,33,34,35]. These are other important elements of the experience of lived space.
Although the majority of the existing guidelines describing design interventions for persons with dementia are founded on research conducted in institutional settings, similar design requirements are regarded as relevant for private homes and for accommodating the continued use and navigation of the outdoor environments [11, 21]. However, the guidelines largely reflect the spatial characteristics of the environment rather than reflecting the spatial dimensions and the feelings among persons with dementia regarding the use of the environment.
Identifying how persons with dementia might experience lived space is important not only to enable the physical environments and to compensate for their incapacities but also to facilitate their continuous engagement and activity in society. Several single studies have explored the perspectives of persons with dementia regarding how they experience lived spaces in different contexts, for example, the process of moving into residential care [36,37,38], living with dementia in long-term care [39,40,41,42,43], receiving community-based home care services [44] and living alone while having dementia [45,46,47,48,49]. Others have described the perspectives of lived space by investigating the experience of meaningful activity and the important aspects of life [43, 50,51,52], the use of everyday technology [53], the experience of the outdoor environment [54] and the accessibility to public space [55]. Literature on the experiences of lived space for persons with dementia is comprehensive and includes several different perspectives, but to our knowledge, few studies have attempted to explicitly review and synthesize this body of literature. Considering how important lived space is for identity and meaningful activities, there is a need for a systematic review that synthesizes the knowledge on this topic. Therefore, the aim of this systematic meta-synthesis was to interpret and synthesize the experience of lived space for persons with dementia.
Methods
Design
The research group conducted an interpretative qualitative meta-synthesis, inspired by the approaches and methods described by Paterson and colleagues and Zimmer [56, 57].
Search method
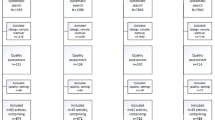
A systematic and computerized search of AgeLine, CINAHL Complete, Embase, Medline and PsycINFO were conducted . MeSH terms and text words for different types of dementia were combined with different descriptions of experience. The combinations of the search terms are shown in Table 1. Studies were limited to qualitative, peer-reviewed research articles of high methodological quality written in English and published between January 2004 and March 2017. The searches resulted in 1386 articles, of which 136 were identified as eligible. Figure 1 presents a flow chart for the selection of the articles.

Flow chart of the literature search
To ensure that there were always at least two authors selecting the articles in terms of screening, eligibility and inclusion, three pairs of authors (EKG and SE/LKJ and SE/LHF and SE) autonomously reviewed the titles, the abstracts, and, in some cases, the full articles of all of the identified studies. This was in accordance with the PRISMA standard of systematic reviews [58]. The authors resolved disagreements by discussion and, if needed, by consulting one of the other pairs of authors. The studies were included if they comprised the following components: (1) a sample of persons with dementia only; (2) a qualitative interview as a research method; (3) the explicit voices of persons with dementia; and (4) a description of experiences of the lived space. The exclusion criteria were as follows: (1) they used a mixed sample, or the dementia diagnosis of the sample was uncertain (i.e., probable or possible dementia), or (2) they studied a certain intervention.
Assessment of the quality of the studies
One hundred thirty-six full text articles were read and reviewed according to the Critical Appraisal Skills Programme (CASP) criteria for qualitative studies [59]. Pairs of authors (LKJ/EKG, KS/LHF, SE/ASH or EKG/SE) assessed the quality of all of the studies. The authors resolved disagreements by discussion and, if necessary, by consulting one of the other pairs of authors. The CASP appraisal tool includes the following nine criteria: (1) a precise statement of aims; (2) an applicable choice of method; (3) a suitable research design; (4) congruence between the recruitment strategy, aims and research; (5) the methods for data collection addressed the research issue; (6) the relationship between the researcher and the participant was considered; (7) ethical issues were reflected; (8) the process of data analysis was sufficiently rigorous; and (9) a clear statement of the findings. An equal weight (i.e., 1 point) was given each criterion, and maximum score was nine for each quality assessment of the studies. A score of 9 points indicated high methodological quality, whereas 7-8 points indicated moderate quality (see Table 2). This review only included studies with moderate and high quality. Seven studies had scores <7 and were therefore excluded due to low quality. This meta-synthesis is based on 45 articles; the studies included are presented in Table 3.
Interviews with 672 persons with dementia are included in this meta-synthesis. The participants are described in Table 4. Studies were reviewed to identify how the severity of dementia was assessed. However, overall, it appeared that the studies’ inclusion criteria gave more weight to participants’ ability to provide informed consent and verbally articulate their experiences of living with dementia than to formal assessments of cognitive impairment. Several of the studies did not provide descriptions of the stage of dementia. Therefore, we lacked complete data with which to determine participants’ severity of dementia. However, all studies provided information about participants’ housing situation. Eleven studies included participants living in nursing homes or other care facilities, thirty-two studies included participants living at home, and two studies had mixed sample. As relocation to long-term care can serve as an indicator of dementia progression and severity, information about the housing situation was described (Table 4) and applied throughout the analysis. Individual interviews with persons with dementia constituted the main data in 41 of the studies. One study was based on interviews with dyads or pairs, and three studies were based on focus group interviews.
Data abstraction and synthesis
The principles of interpretative synthesis [60] guided the abstraction process. It focused on developing concepts based on the data from primary studies and further developing and specifying theories that integrated those concepts [61]. The analysis was inspired by qualitative content analyses [62]. This procedure enabled explicit focus on content and context in the studies, and emphasis on the similarities and differences between categories and subcategories. It also facilitated analysis concentrating on both manifest, describing what the studies reported, and latent content, referring to the interpretation of the underlying meaning.
Five phases constituted the analysing process: Pairs of authors (LKJ/EKG, KS/LHF and SE/ASH) each read and reread one-third of the papers in the first phase. Phrases from each paper describing lived space, in line with van Manen [12], were extracted as direct citations into a table made for analysis and sorted depending on the housing situation for persons with dementia (living in own home or in nursing home). Two of the authors (LHF and SE) then performed a further analysis. In the second phase, the extracted text was divided into meaning units and condensed. Condensation refers to a process of shortening and abstracting meaning units while preserving the core of the manifest content [62]. The third phase comprised labelling condensed meaning units with codes. Several codes were discussed in this process. This phase provided insight into the existential meaning of lived space, such as the importance of having a sense of continuity, familiarity and experiencing autonomy. Such existential elements appeared important regardless of housing situation. Comparing codes, recognising parallels and variances, and organising the codes into subcategories constituted the fourth phase. It became apparent through this process how the existential meaning of space may change related to the housing situation of persons with dementia. Keeping the housing situation as subcategories was therefore meaningful. Further abstraction of the codes resulted in four categories describing the manifest meaning (see Table 5: Results). In the fifth phase, the comprehensive understanding phase, the four categories with subcategories were seen as a whole, condensed and reflected upon to identify the underlying meaning of the results as one overall latent theme [62]. The third, the fourth and the fifth phase of the analysis were discussed within the author group to make consensus.
Results
The material revealed four main categories describing the experience of space: (1) belonging; (2) meaningfulness; (3) safety and security; and (4) autonomy. The analysis showed that living in one’s own home and living in long-term care involved different settings and posed diverse challenges for the experience of lived space among persons with dementia. Therefore, the two settings constitute two subcategories. The descriptions were distinct and associated with the setting. The studies described the space of home or long-term care itself but also the space surrounding the place they lived (i.e., outdoor space). Some studies also included descriptions of the experience of public space and national space.
Belonging
Own home
Persons with dementia considered living at home and in their own home to be very important. They perceived home as a place for belonging and the key for living a good and meaningful life. They described their experience of home as feeling at home and being at home. Feeling at home included the feeling of belonging and being a part of something. Being at home represented the experience of being together with important people in their lives. It also embodied specific familiar objects, activities and experiences concretizing values, interests and status. Home and the symbol of home connected persons with dementia to their history. One participant said, “It mirrors the way we are” [63]. Engaging in social activities, being with friends and family, and attending socio-emotional preoccupations were important aspects of their experience of home. They described doing things with others in positive terms.
However, some persons with dementia experienced their daily life as uneventful, as they were not able to take the initiative to do things. They described that they sat around and did nothing; some described the experience of being idle. One participant said, “I sit here (at home) like a crow in her nest” [64].
In a wider sense, belonging at home also incorporated different levels of belonging to outside environments. The experience of being able to use the local neighbourhood and take part in the community and the feeling of belonging to the country were considered important. This contributed to a feeling of connectedness with the world. Outdoor environments were considered arenas for social activities and an essential source for sustaining identity. Familiarity with outdoor environments also seemed important for the ability to carry on with life and to maintain known activities. Being a part of a neighbourhood could prevent loneliness, encourage social activities, make living a typical life possible and lead to a more vivid life. Living close to sites such as churches or stores was therefore important. Nevertheless, some also described the experience of being vulnerable and the fear of being exposed when in public spaces, and others used terms such as being embarrassed or feeling shame.
The feeling of unfamiliarity increased with the symptoms of dementia. In cases of concrete episodes of disorientation, persons with dementia perceived that outdoor space was automatically narrowed. Their ability to use public places decreased due to the development of dementia. For instance, not being able to drive increased this experience. In addition, they experienced outdoor environments as unfamiliar and their possibilities of participation as restricted. They described this experience as slipping away from the world and being left alone. Some stated that they managed to find their way back home even though the environment was less familiar than before; others were reluctant to leave home alone.
Long-term care
Persons with dementia living in long-term care described belonging as the experience of being familiar with the setting and being in the right place. Relocating into long-term care appeared to cause disorientation in some cases and challenged their overall sense of belonging. They described relocation in two ways: either as the beginning of the end or as the start of a new life that signalled an overall “winding down” [36].
Belonging, as an experience of being part of the new environment, appeared to be important. In some studies, persons with dementia reflected upon the long-term care environment and what would promote a sense of belonging. Persons with dementia were still able to sense, feel and appreciate lived spaces. However, the process of being familiar with a new place after relocation and experiencing belonging appeared to be time consuming and dependent on several influences. Being able to maintain contact with family and to uphold familiar activities were emphasized as important. Becoming familiar with the long-term care setting and its associated activities and being accepted and confirmed as a whole person by the other residents and health care personnel were essential aspects of developing a sense of belonging. Being in an unfamiliar setting with unknown people appeared to foster stress, confusion and anxiety. Lastly, some persons with dementia emphasized the ability to have a private life as important to sustain their experience of belonging to the place.
Persons with dementia who struggled to find their place and to experience belonging in the new environment related these difficulties to a number of issues. Some described their inability to view the long-term care facility as their home. Some also expressed being disillusioned by the noise and busyness in the long-term care environment, and they described the care environment as a place with rules and restrictions, which restrained their individuality. They experienced the long-term care setting as uncomfortable. Several studies described their struggle of homesickness, which appeared to be related to both the difficulties of experiencing hominess and belonging in the long-term care environment and to the longing for familiar others, their own home and familiar surroundings. Living everyday life among unfamiliar residents seemed to increase their feeling of homesickness.
Meaningfulness
Own home
Persons with dementia described home as a centre for meaning. They described it as a place for retreat, solitude, and rejuvenation; a centre for socialization, connectedness and affiliation; and a centre for meaningful activities of daily living. Home was supposed to be organized and presented in a particular manner. Some described the importance of a clean and neat home, even if it was sometimes described as difficult to keep up with the preferred standard for their home due to their dementia symptoms. Some persons with dementia felt ashamed when they were not able to take care of their home the way they wanted to and had before, for example, when next of kin took over all of the shopping. Persons with dementia described that life had shrunken after dementia came into their lives and that they felt that they were dependent on their next of kin. However, one woman described that her life had changed little after she received her dementia diagnosis because she had continued to do the things she used to, and she still felt like an independent and responsible woman.
Doing outdoor activities was considered central for the experience of meaning, even though some experienced that their interest in certain activities had changed after developing dementia. Some emphasized that it was important to do as much as they could do for as long as they were able to. Going outside, for instance, for a walk in a familiar environment allowed them to maintain a sense of coping and current status. To some, this was even an expression of hope in life. Going for a walk outside their home not only ensured physical exercise and fresh air but also created a sense of well-being. Additionally, when the environment was less familiar than before, going outdoors for a walk alone was important to participants in some of the studies.
Long-term care
Meaningfulness was related to the person’s ability to be occupied with interesting and relevant activities when living in long-term care. Some persons with dementia experienced long-term care as an important arena for social activities and a place where they could meet people and expand their social opportunities. However, to others, relocating to long-term care had the opposite effect, and they longed for privacy. Some also expressed that they were bored in this setting, that the long-term care lacked alternatives for activities, and that they longed for their own home and well-known activities.
Although their experiences clearly varied, many persons with dementia experienced that they were dependent on health care personnel to initiate activities. However, there was variation in how they experienced meaningfulness in relation to participating in the activities. While some expressed that they wanted to be left alone or preferred to stay in bed all day, others described that socializing with others led to a state of contentment and increased energy. Examples described in the articles were individual activities such as walking inside and outside the facility or doing familiar things such as cleaning and socializing (through, for instance, playing bingo or staying in the living room). Others stated that the activities offered in long-term care were limited or did not interest them. Others emphasized that they could choose whether they wanted to participate in activities. Persons with dementia highlighted that being familiar with the place was the key to empowering their maintenance of daily activities and retaining some sense of independent living.
Safety and security
Own home
Persons with dementia described home as a place for safety and security, a place where they could avoid stress and do things at their own pace. They also described home as an arena for coping, comfort and continuity in relation to traditions and social life. It was important for them to carry on as normal. However, home was also a setting for frustration and anger. With dementia, life became more home-centred and isolated. Some expressed a bad feeling of no longer being able to manage living at home because, for instance, everyday articles lost their meaning. It was also described as important to prepare and use systems to facilitate everyday coping as long as possible.
Some persons with dementia stated that continuing to maintain outdoor activities and to use public places was a useful coping strategy for handling their cognitive impairment. Others described that their feeling of anxiety constrained their outdoor activities. Some locked the door to the outside world in order to protect themselves and feel safe and secure.
Several studies emphasized the thoughts of persons with dementia about no longer being able to live in their own homes/in familiar places. “To stay home as long as I can” [48] was acknowledged as limited in duration. Phrases such as “to stay at home” [47] and “being moved from home” [34] were used to describe the possibility of going to long-term care. Some expressed worries about others reporting that they had difficulties living in their homes alone. They tried to avoid “making mistakes” [49] and attempted to hide their difficulties from their next of kin. Some expressed that the burden on their families, their worsening condition and their family members’ exhaustion were factors facilitating the endpoint of their living in their own home.
In some studies, persons with dementia emphasized the importance of being outdoors despite getting lost, misunderstanding and forgetting. Some still felt safe and were not afraid of doing activities. They trusted that someone would find them, take care of them and lead them home. Doing activities on their own and going to well-known places allowed them to maintain a sense of self. In other cases, performing activities independently and out of the house was infeasible. Others preferred staying in their homes to feel safe.
Long-term care
Safety in long-term care was related to the sense of being safe and comforted. Persons with dementia described long-term care as a place for hospitality and rest, as it relieved them of household responsibilities, cleaning and cooking. It was also expected that they were cared for and provided with company when residing in long-term care. Familiar, calm and peaceful surroundings were associated with a feeling of safety and comfort. They described an “old-style” [65] interior setting as a way of providing a sense of security and continuity.
Living in long-term care facilities were described as providing an experience of safety and security. Safety and security were emphasized in numerous studies. In some cases, persons with dementia expressed a need to feel secure and safe while living in long-term care. However, in other studies, they highlighted the tension between their need for safety and security and their need for independence.
Autonomy
Own home
Many persons with dementia perceived that living in their own home was the locus of autonomy, control, choice and the freedom to act. They experienced home as a place for preserving autonomy, and they highlighted the importance of being able to take care of themselves and to use aids such as technology. They expected themselves to be able to use helpful technology. The loss of former and valued activities, such as the ability to drive, was described as difficult.
Being outdoors alone and being able to drive provided autonomy and were experienced as a sense of relief, escape, wellbeing, pleasure and freedom. In the studies, persons with dementia described restrictions related to going out on their own, being dependent on others to go out, a loss of ability to go to new places, and others’ concern about their getting lost. Some persons with dementia also emphasized the importance of accessibility to the outside environment and said that signs and landmarks were promoting factors. It was often difficult for them to find their way in a public space, and using a map did not help. In addition, public spaces may be less accessible at certain times of the day. Another obstacle to accessibility cited by persons with dementia was the replacement of service personnel with technology. They could no longer just buy a ticket from service personnel, as tickets were to be bought from ticket machines. The loss of the possibility to go out and to drive increased their dependency and prevented them from moving around freely.
In studies focusing on the relocation from home to long-term care, several persons with dementia described the experience of losing their autonomy. Relocation was not their preference, and they did not look forward to it; it was paralleled with “giving up” [47], “being putted away” [50], and “letting somebody be over you” [38]. They also experienced relocating to residential care as a shift from being an active and independent person to living in a more structured, protected and supported life collectively with others.
Long-term care
Lack of autonomy was related not only to relocation but also to everyday life in long-term care. Living in long-term care was associated with monotonous living, a loss of abilities and freedom, fewer opportunities for individual choices, a lack of privacy and uncertainty. Some experienced that they had poor social interactions and felt isolated from friends and family.
In several studies, persons with dementia emphasized that in long-term care, they were involved in shaping their own services, were informed and had their needs appreciated. However, in some cases, persons with dementia experienced having little control over their own life. They experienced restrictions in relation to the long-term care environment, the organization of the ward and the rules and routines operated by the staff. They described that being dependent on the staff to be able to maintain well-known activities and being held indoors (not being allowed to go outdoors) inhibited their autonomy. In one study, living in long-term care was described as “living in a prison without bars” [66]; another study described a feeling of being trapped [67].
A space where the walls keep closing in
The comprehensive understanding of the categories described is captured in the latent theme: “Living with dementia is similar to living in a space where the walls keep closing in.” Our findings show that lived space is reduced as dementia develops. This indicates a process whereby lived space gradually becomes smaller. A space where the walls keep closing in can be understood through the metaphor of the Russian “babushka doll,” which is a set of dolls of decreasing sizes that all fit inside one another one by one. Similar to the “person within a similar person” of the babushka doll, people with dementia experience the walls closing in, and step-by-step, the experience of lived space is reduced from large and wide to small and restricted. Thus, the findings indicate the strong connection between the experience of lived space and the importance of sustaining feelings of belonging, meaningfulness, safety and security and autonomy among persons with dementia. All of these aspects can be considered existential in nature. These are all feelings that might support the ability to preserve a sense of continuity, maintain self-identity and sustain a sense of attachment to a place.
Discussion
The aim of this systematic meta-synthesis was to interpret and synthesize the experiences of space in persons with dementia. The main findings indicate a process whereby lived space continually decreases due to the progression of dementia. The metaphor of the Russian babushka doll can be used to describe the experiences of persons with dementia living in a space where the walls keep closing in. Regardless of the progression of dementia, they continue to experience the spatial dimensions of life through lived space. According to van Manen [12], lived space is one of the cornerstones of the lifeworld experience, and it influences and is influenced by other lifeworld perspectives.
Research within the field of environmental gerontology, i.e., [13, 68,69,70], has emphasized the importance of supporting the ability to preserve a sense of continuity, maintain self-identity and sustain attachment to a place for maintaining a sense of being in place, or, in van Manens’ [12] words, maintaining a sense of space. Our findings show that belonging, meaningfulness, security and autonomy are essential elements of the experience of lived space among persons with dementia. Despite the differing use of the terms, the essence can be understood as compatible with the findings in our study.
With the progression of dementia, patients’ cognitive abilities decrease [71]. As indicated in this study and others, i.e., [18, 29,30,31, 72], the diminishing cognitive capacity might challenge persons’ capability of familiarizing themselves even with well-known environments, making their own choices and taking advantage of possible opportunities. Due to progression of dementia, persons’ physical capability will also often change. This change of lived body, in accordance with van Manen [12], leads to a decrease in the room of action; both the experience of the space and the environment grow smaller. However, to maintain safety and security, meaning, belonging and autonomy as essential dimensions of space, it appears that a reduction of the environment is a necessity.
The progression of dementia often leads to a need for relocation from one’s own home to a long-term care facility [73]. Thirteen studies described participants’ experiences of lived space while living nursing home or other facilities. Within our data, moving into a long-term care facility was described as “giving up”, a loss of freedom, a lack of privacy, being in prison and living a structured, protected life in a collective living environment. Fear of relocation was often expressed long before it actually occurred. This fear can be understood as a fear of facing a new and unknown life situation and as a fear of being taken away from a well-known daily life. The replacement of the lived space might threaten all of the essential dimensions of belonging, meaningfulness, safety and security, and autonomy. One might see lived space as an expression of existence. According to Goyal et al. [74], anxiety symptoms among persons with dementia could be a reaction to loss and worry, especially the experience of dealing with a new situation, i.e., relocation. Goyal [74] stated that anxiety among these persons must therefore be understood as existential in nature. Anxiety symptoms are common among persons with dementia and might lead to negative impacts such as decreased function in activities of daily living [75], increased dependency [76] behaviour problems [77, 78] and an additional burden on the patients and caregivers [79]. Nonetheless, anxiety symptoms in patients with dementia are often overlooked by caregivers and health care personnel [80].
The results of this study suggest that facing new environments threatens a person’s existence, such as the ability to uphold a sense of control over one’s own life, protecting privacy, and making choices of importance. When relocating into a residential facility, persons need to reconstruct their sense of space. They have to convert a place that is neutral into a place that has meaning in the context of their ongoing life [13,14,15]. Lived space is closely related to a person’s maintenance of his or her self-identity and sense of attachment to the place [13,14,15]. The metaphor of the Babushka doll pictures the recognition of oneself, being oneself and feeling connected to one’s self-identity despite decreasing environmental space.
Several studies described the outdoor environment as an important factor for lived space while living in one’s own home. Going outdoors was connected to emotional well-being, prevention of loneliness, being physically active and having a feeling of freedom. To some, doing the same things and going to the same places as before helped them maintain a sense of self. Taking part in the local environment and community was also described as central to some. Others described that going outdoors was difficult due to the orientation and memory impairment and they felt isolated in their own homes. In most of the studies that interviewed persons with dementia living in their own homes, the outdoor environment was a topic even when they did not make use of it. In contrast, this was not emphasized in most of the studies interviewing persons with dementia living in long-term care facilities, where outdoor space was not a topic at all.
In our study, persons appeared to have adapted themselves to their situation as a conscious or unconscious strategy by reducing their environment. As dementia progresses, persons become increasingly dependent on others. This includes help with outdoor activities, finding one’s way around and taking the initiative to go outdoors. Whear et al. [81] stated that persons with dementia living in long-term care facilities often spend all of their time or most of their time in doors. Others have found that spending time in a garden could have an impact on the agitation in care home residents [82]. Even so, being outdoors in nature or a garden might have positive consequences for persons with dementia. In a review, Gonzalez and Kirkevold [83] found that targeted use of plants might have a positive influence on the function, behaviour and well-being of people with dementia.
The experience of lived space can be seen in relation to the concept of ‘at-homeness’, which refers to a place where the person feels safe, connected, respected, understood and loved [84]. Öhlen et al. [85] shows in a review how older persons construct ‘at-homeness’ despite illness and disease as a particular aspect of wellness. At-homeness is a feeling that is created in partnership with others. The maintenance of meaningful social relations, meaningful lived relations, are therefore considered important dimensions of space and as prerequisites for feeling at home and being connected to place, whether the persons are living in their own homes or in long-term care facilities [33, 86, 87]. The frameworks of person-centred dementia care emphasize the importance of sustaining social needs [88]. Based upon these values, McChance et al. [89] describe the importance of setting individuals free in a flourishing environment where they are confirmed and respected as unique individual persons, whether they are living at home or in a nursing home.
Strengths and limitations
We performed a systematic meta-synthesis with transparent descriptions of the selection process for the included articles. However, we acknowledge that a complete overview was not attainable. The value of both individual reviewers and the use of pairs of researchers to evaluate the studies should be acknowledged.
The systematic approach taken to source and analyse the available qualitative data is a considerable strength of this meta-synthesis. Qualitative content analysis facilitated explicit attention on the manifest descriptions of the experiences of persons with dementia provided through the primary studies. Through combining manifest descriptions with interpretation of the latent meaning of their experiences, we believe that this meta-synthesis provides new and important contribution to the field. However, data comprising descriptions of people’s experiences always involves multiple meanings depending on subjective interpretation. The dialogue among the authors throughout the analysing process was therefore valuable to seek agreement of the way in which data was sorted and labelled. Together with a high level of transparency through the rich presentation of findings and the condensed meaning units provided in Table 5, this contributed to the credibility of the study. To facilitate transferability, providing description of the context of study was important. Classification of dementia severity among participants was important to appraise dementia progression in relation to experiences of lived space. However, it appeared difficult because several articles lacked descriptions of dementia severity. The synthesis of results depending on the participants’ housing situation still provided valuable insight into how progression of dementia may influence the experiences of lived space. Adopting the same search strategy as the earlier systematic review, which studied the experience of the lived relation in persons with dementia [5], has enabled direct comparison for a more in-depth understanding.
Only studies published in scientific journals were included in the systematic review. The voices of persons with dementia published in the “grey literature” were not explored in this article. An analysis of the different interviewing guides could explore different views of persons with dementia and were not always fully described in the included studies.
Conclusion
This meta-synthesis revealed four main categories: (1) belonging; (2) meaningfulness; (3) safety and security; and (4) autonomy. The categories illustrate how the experience of lived space may change with the living situation of persons with dementia. Through interpreting relocation to nursing home as a measure of dementia progression, our findings show that persons with dementia experience a reduction in their lived space as dementia develops. This indicates a process where lived space gradually becomes smaller. The Russian babushka doll serves as a metaphor describing the comprehensive understanding of the categories leading to the latent theme: “Living with dementia is like living in a space where the walls keep closing in.”
This meta-synthesis indicates the importance of being aware of the experiences of the spatial dimensions in the lifeworld of persons with dementia. To sustain person-centred care and to support the preservation of continuity and identity, one has to acknowledge not only the physical and social environment but also space as an existential experience for persons with dementia.
Abbreviations
- CASP:
-
Critical Appraisal Skills Programme
References
Kenigsberg P-A, Aquino J-P, Bérard A, Gzil F, Andrieu S, Banerjee S, Brémond F, Buée L, Cohen-Mansfield J, Mangialasche F, et al. Dementia beyond 2025: Knowledge and uncertainties. Dementia. 2016;15(1):6–21.
Giebel CM, Sutcliffe C, Stolt M, Karlsson S, Renom-Guiteras A, Soto M, Verbeek H, Zabalegui A, Challis D. Deterioration of basic activities of daily living and their impact on quality of life across different cognitive stages of dementia: a European study. Int Psychogeriatr. 2014;26(8):1283–93.
Han A, Radel J, McDowd JM, Sabata D. Perspectives of People with Dementia About Meaningful Activities. Am J Alzheimers Dis Other Demen. 2016;31(2):115–23.
Patterson KM, Clarke C, Wolverson EL, Moniz-Cook ED. Through the eyes of others – the social experiences of people with dementia: a systematic literature review and synthesis. Int Psychogeriatr. 2017:1–15. https://doi.org/10.1017/S1041610216002374.
Eriksen S, Helvik AS, Juvet LK, Skovdahl K, Førsund LH, Grov EK. The Experience of Relations in Persons with Dementia: A Systematic Meta-Synthesis. Dement Geriatr Cogn Disord. 2016;42(5-6):342–68.
Prince M, Wimo A, Guerchet M, Ali G-C, Wu Y-T, Prina M. World Alzheimer Report 2015. An analysis of prevalence, incidence, cost and trends. London: Alzheimer’s Disease International; 2015.
World Health Organization. Dementia: a public health priority. 2012. http://apps.who.int/iris/bitstream/10665/75263/1/9789241564458_eng.pdf?ua=1 Accessed 20 Feb 2017
de Vugt M, Dröes R-M. Social health in dementia. Towards a positive dementia discourse. Aging Ment Health. 2017;21(1):1–3.
Wolverson EL, Clarke C, Moniz-Cook ED. Living positively with dementia: a systematic review and synthesis of the qualitative literature. Aging Ment Health. 2016;20(7):676–99.
World Health Organization. World report on ageing and health. 2015. http://apps.who.int/iris/bitstream/10665/186463/1/9789240694811_eng.pdf?ua=1 Accessed 20 Feb 2017
van Hoof J, Kort HSM, van Waarde H, Blom MM. Environmental Interventions and the Design of Homes for Older Adults With Dementia: An Overview. Am J Alzheimers Dis Other Demen. 2010;25(3):202–32.
van Manen M. Researhing Lived Experience. Human Science for an Action Sensitive Pedagogy. 2nd ed. Ontario: The Althouse Press; 1997.
Rowles GD, Bernard M. The Meaning and Significance of Place in Old Age. In: Rowles GD, Bernard M, editors. Environmental Gerontology. New York: Springer Publishing Company; 2013. p. 3–24.
Aminzadeh F, Molnar FJ, Dalziel WB, Garcia LJ. An Exploration of Adjustment Needs and Efforts of Persons with Dementia After Relocation to a Residential Care Facility. J Hous Elder. 2013;27(1-2):221–40.
Rubinstein R, Parmelee P. Attachment to Place and the Representation of the Life Course by the Elderly. In: Altman I, Low S, editors. Place Attachment. New York, NY: Springer US; 1992. p. 139-163.
Van Hoof J, Kort HSM. Supportive living environments: A first concept of a dwelling designed for older adults with dementia. Dementia. 2009;8(2):293–316.
Fleming R, Goodenough B, Low L-F, Chenoweth L, Brodaty H. The relationship between the quality of the built environment and the quality of life of people with dementia in residential care. Dementia. 2016;15(4):663–80.
Calkins MP. Evidence-based long term care design. Neurorehabilitation. 2009;25(3):145–54.
Høyland K, Kirkevold Ø, Woods R, Haugan G. Er smått alltid godt i demensomsorgen? Om bo- og tjenestetilbud for personer med demens [In Norwegian] [Is small always the best in dementia care? About public housing solutions for persons with dementia]. In: SINTEF Fag 33; 2015. http://www.ks.no/contentassets/1392e8fff1a847eb8b632ac582afa98a/rapport.pdf. Accessed 19 Feb 2017.
Davis S, Byers S, Nay R, Koch S. Guiding design of dementia friendly environments in residential care settings: Considering the living experiences. Dementia. 2009;8(2):185–203.
Mitchell L, Burton E, Raman S, Blackman T, Jenks M, Williams K. Making the outside world dementia-friendly: design issues and considerations. Environ Planning B Plann Design. 2003;30(4):605–32.
Lin S-Y, Lewis FM. Dementia Friendly, Dementia Capable, and Dementia Positive: Concepts to Prepare for the Future. Gerontologist. 2015;55(2):237–44.
Europe A. Is Europe becoming more dementia friendly? In: Dementia in Europe Yearbook 2015. http://www.alzheimer-europe.org/content/download/128795/803875/file/2015%20Yearbook%20-%20Dementia-friendly.pdf. Accessed 19 Feb 2017.
Edvardsson D, Fetherstonhaugh D, Nay R. Promoting a continuation of self and normality: person-centred care as described by people with dementia, their family members and aged care staff. J Clin Nurs. 2010;19(17-18):2611–8.
Brooker D. What is person-centred care in dementia? Rev Clin Gerontol. 2004;13(3):215–22.
Harmer BJ, Orrell M. What is meaningful activity for people with dementia living in care homes? A comparison of the views of older people with dementia, staff and family carers. Aging Ment Health. 2008;12(5):548–58.
Sherman E, Dacher J. Cherished Objects and the Home: Their Meaning and Roles in Later Life. In: Rowles GD, Chaudbury H, editors. Home and Identity in Late Life, International persepectives. New York: Springer Publishing Company; 2005. p. 63–79.
Day K, Carreon D, Stump C. The therapeutic design of environments for people with dementia a review of the empirical research. Gerontologist. 2000;40(4):397–416.
Marquardt GP, Bueter KMA, Motzek TM. Impact of the Design of the Built Environment on People with Dementia: An Evidence-Based Review. HERD. 2014;8(1):127–57.
Marquardt G. Wayfinding for People with Dementia: A Review of the Role of Architectural Design. HERD. 2011;4(2):75–90.
Marquardt G, Schmieg P. Dementia-Friendly Architecture: Environments That Facilitate Wayfinding in Nursing Homes. Am J Alzheimers Dis Other Demen. 2009;24(4):333–40.
Cutchin MP. The Complex Process of Becoming At-Home in Assisted Living. In: Rowles GD, Bernard M, editors. Environmental Gerontology. New York: Springer Publishing Company; 2013. p. 105–23.
Falk H, Wijk H, Persson LO, Falk K. A sense of home in residential care. Scand J Caring Sci. 2013;27(4):999–1009.
Fleming R, Kelly F, Stillfried G. I want to feel at home’: establishing what aspects of environmental design are important to people with dementia nearing the end of life. BMC Palliat Care. 2015;14:26.
Verbeek v RE, Zwakhalen SM, Kempen GI, Hamers JP. Small, homelike care environments for older people with dementia: a literature review. Int Psychogeriatr. 2009;21(02):252–64.
Aminzadeh F, Dalziel WB, MF GLJ. Symbolic meaning of relocation to a residential care facility for persons with dementia. Aging Ment Health. 2009;13(3):487–96.
Aminzadeh F, Molnar FJ, Dalziel WB, Garcia LJ. Meanings, functions, and experiences of living at home for individuals with dementia at the critical point of relocation. J Gerontol Nurs. 2010;36(6):28–35.
Thein NW, D'Souza G, Sheehan B. Expectations and experience of moving to a care home: Perceptions of older people with dementia. Dementia. 2011;10(1):7–18.
Tak SH, Kedia S, Tongumpun TM, Hong SE. Activity Engagement: Perspectives from Nursing Home Residents with Dementia. Educ Gerontol. 2015;41(3):182–92.
van Zadelhoff E, Verbeek H, Widdershoven G, van Rossum E, Abma T. Good care in group home living for people with dementia. Experiences of residents, family and nursing staff. J Clin Nurs. 2011;20(17-18):2490–500.
Mjørud M, Engedal K, Røsvik J, Kirkevold M. Living with dementia in a nursing home, as described by persons with dementia: a phenomenological hermeneutic study. BMC Health Serv Res. 2017;17(1):93.
Hedman R, Hansebo G, Ternestedt B-M, Hellström I, Norberg A. How people with Alzheimer’s disease express their sense of self: Analysis using Rom Harré’s theory of selfhood. Dementia. 2013;12(6):713–33.
Moyle W, Venturto L, Griffiths S, Grimbeek P, McAllister M, Oxlade D, Murfield J. Factors influencing quality of life for people with dementia: a qualitative perspective. Aging Ment Health. 2011;15:970–7.
Gill L, White L, Cameron ID. Service co-creation in community-based aged healthcare. Manag Serv Qual. 2011;21(2):152–77.
Nygård L. The meaning of everyday technology as experienced by people with dementia who live alone. Dementia. 2008;7(4):481–502.
Svanström R, Johansson Sundler A. Gradually losing one’s foothold – A fragmented existence when living alone with dementia. Dementia. 2015;14(2):145–63.
Frazer SM, Oyebode JR, Cleary A. How older women who live alone with dementia make sense of their experiences: An interpretative phenomenological analysis. Dementia. 2012;11(5):677–93.
De Witt L, Ploeg J, Black M. Living alone with dementia: an interpretive phenomenological study with older women. J Adv Nurs. 2010;66(8):1698–707.
De Witt L, Ploeg J, Black M. Living on the threshold: The spatial experience of living alone with dementia. Dementia. 2009;8(2):263–91.
Phinney A. Family Strategies for Supporting Involvement in Meaningful Activity by Persons With Dementia. J Fam Nurs. 2006;12(1):80–101.
Phinney A. Horizons of Meaning in Dementia: Retained and Shifting Narratives. J Relig Spiritual Aging. 2011;23(3):254–68.
Wolverson EL, Clarke C, Moniz-Cook E. Remaining hopeful in early-stage dementia: A qualitative study. Aging Ment Health. 2010;14(4):450–60.
Brittain K, Corner L, Robinson L, Bond J. Ageing in place and technologies of place: the lived experience of people with dementia in changing social, physical and technological environments. Sociology of Health & Illness. 2010;32(2):272–87.
Duggan S, Blackman T, Martyr A, Van Schaik P. The impact of early dementia on outdoor life. Dementia. 2008;7(2):191–204.
Brorsson A, Öhman A, Lundberg S, Nygård L. Accessibility in public space as perceived by people with Alzheimer’s disease. Dementia. 2011;10(4):587–602.
Paterson B, Thorne S, Canam C, Jillings C. Meta-study of Qualitative Health Research: A Practical Guide to Meta-analysis and Meta-synthesis. Thousand Oaks: Sage Publications; 2001.
Zimmer L. Qualitative meta-synthesis: a question of dialoguing with texts. J Adv Nurs. 2006;53(3):311–8.
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart L. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;350:g7647.
Critical Appraisal Skills Programme (CASP). Qualitative Research Checklist. In: Critical Appraisal Skills Programme (CASP); 2014. http://www.casp-uk.net/#!checklists/cb36. Accessed 1 Mar 2015.
Dixon-Woods M, Agarwal S, Jones D, Young B, Sutton A. Synthesising qualitative and quantitative evidence: a review of possible methods. J Health Serv Res Policy. 2005;10:45–53.
Eilertsen G, Ormstad H, Kirkevold M. Experiences of poststroke fatigue: a qualitative meta-synthesis. J Adv Nurs. 2013;69(3):514–25.
Graneheim U, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–12.
Keller HH, Martin LS, Dupuis S, Genoe R, Edward HG, Cassolato C. Mealtimes and being connected in the community-based dementia context. Dementia. 2010;9(2):191–213.
Vikström S, Josephsson S, Stigsdotter-Neely A, Nygård L. Engagement in activities. Dementia. 2008;7(2):251–70.
Liou CL, Jarrott SE. Taiwanese Experiences: Elders with Dementia in Two Different Adult Day Service (ADS) Environments. Aging Ment Health. 2013;17(8):942–51.
Heggestad AK, Nortvedt P, Slettebo A. Like a prison without bars’: dementia and experiences of dignity. Nurs Ethics. 2013;20:881–92.
Nowell ZC, Thornton A, Simpson J. The subjective experience of personhood in dementia care settings. Dementia. 2013;12(4):394–409.
Rubinstein RL, de Medeiros K. Home, self and identity. In: Rowles GD, Chaudbury H, editors. Home and Identity in Late Life, International Perspectives. New York: Springer Publishing Company; 2005. p. 47–62.
Wahl H-W, Weisman GD. Environmental Gerontology at the Beginning of the New Millennium: Reflections on Its Historical, Empirical, and Theoretical Development. The Gerontologist. 2003;43(5):616–27.
Oswald F, Wahl H-W. Dimensions of the meaning of Home in Later Life. In: Rowles GD, Chaudhury H, editors. Home and Identity in Late Life, International perspectives. New York: Springer Publishing Company; 2005. p. 21–47.
Mitchell SL, Black BS, Ersek M, Hanson LC, Miller SC, Sachs GA, Teno JM, Morrison RS. Advanced dementia: state of the art and priorities for the next decade. Ann Intern Med. 2012;156(1):45–51.
Fleming R, Purandare N. Long-term care for people with dementia: environmental design guidelines. Int Psychogeriatr. 2010;22(7):1084–96.
Broda A, Bieber A, Meyer G, Hopper L, Joyce R, Irving K. The ActifCare Consortium. Perspectives of policy and political decision makers on access to formal dementia care: expert interviews in eight European countries. BMC Health Serv Res. 2017;17:518. http://doi.org/10.1186/s12913-017-2456-0.
Goyal AR, Engedal K, Eriksen S. Clinicians’ experiences of anxiety in patients with dementia. Dementia. 2016; https://doi.org/10.1177/1471301216659770.
Teri L, Ferretti LE, Gibbons LE, Logsdon RG, McCurry SM, Kukull WA, McCormick WC, Bowen JD, Larson EB. Anxiety in Alzheimer's Disease: Prevalence and Comorbidity. The Journals of Gerontology: Series A. 1999;54(7):348–52.
Orrell M, Bebbington P. Psychosocial stress and anxiety in senile dementia. J Affect Disord. 1996;39(3):165–73.
Gibbons LE, Teri L, Logsdon R, Mc Curry SM, Kukull W, Bowen J, Mc Cormick W, Larson E. Anxiety Symptoms as Predictors of Nursing Home Placement in Patients with Alzheimer's Disease. J Clin Geropsychol. 2002;8(4):335–42.
Ownby RL, Harwood DG, Barker WW, Duara R. Predictors of anxiety in patients with Alzheimer's disease. Depression and Anxiety. 2000;11(1):38–42.
Cooper C, Balamurali TBS, Livingston G. A systematic review of the prevalence and covariates of anxiety in caregivers of people with dementia. Int Psychogeriatr. 2006;19(2):175–95.
Seignourel PJ, Kunik ME, Snow L, Wilson N, Stanley M. Anxiety in dementia: A critical review. Clin Psychol Rev. 2008;28(7):1071–82.
Whear R, Coon JT, Bethel A, Abbott R, Stein K, Garside R. What Is the Impact of Using Outdoor Spaces Such as Gardens on the Physical and Mental Well-Being of Those With Dementia? A Systematic Review of Quantitative and Qualitative Evidence. J Am Med Dir Assoc. 2014;15(10):697–705.
Detweiler MB, Murphy PF, Myers LC, Kim KY. Does a Wander Garden Influence Inappropriate Behaviors in Dementia Residents? Am J Alzheimers Dis Other Demen. 2008;23(1):31–45.
Gonzalez MT, Kirkevold M. Benefits of sensory garden and horticultural activities in dementia care: a modified scoping review. J Clin Nurs. 2014;23(19-20):2698–715.
Österlind J, Ternestedt B-M, Hansebo G, Hellström I. Feeling lonely in an unfamiliar place: older people’s experiences of life close to death in a nursing home. Int J Older People Nursing. 2017;12(1):e12129.
Öhlen J, Ekman I, Zingmark K, Bolmsjö I, B E. Conceptual development of “at-homeness” despite illness and disease: A review. Int J Qual Stud Health Well-being. 2014;9(1):23677.
Førsund LH, Ytrehus S. Finding a place to connect: A qualitative study exploring the influences of the physical and social environments on spouses’ opportunities to maintain relationships when visiting a partner with dementia living in long-term care. Dementia. 2016; https://doi.org/10.1177/1471301216656087.
Sixsmith J. The meaning of home: An exploratory study of environmental experience. J Environ Psychol. 1986;6(4):281–98.
McCormack B, McCance T. Underpinning principles of person-centred practice. In: McCormack B, McCance T, editors. Person-Centred Practice in Nursing and Health Care: Theory and Practice. 2nd ed. Oxford: Wiley-Blackwell; 2017. p. 13–36.
Mc Cance T, Mc Cormack B, Dewing J. An Exploration of Person-Centredness in Practice. Online J Issues Nurs. 2011;16(2):1.
Beattie A, Daker-White G, Gilliard J, Means R. ‘How can they tell?’ A qualitative study of the views of younger people about their dementia and dementia care services. Health Soc Care Community. 2004;12(4):359–68.
Bronner K, Perneczky R, Mc Cabe R, Kurz A, Hamann J. Which medical and social decision topics are important after early diagnosis of Alzheimer’s Disease from the perspectives of people with Alzheimer’s Disease, spouses and professionals? BMC Res Notes. 2016;9(1):149.
Clare L, Rowlands J, Bruce E, Surr C, Downs M. The experience of living with dementia in residential care: an interpretative phenomenological analysis. Gerontologist. 2008;48(6):711–20.
Digby R, Moss C, Bloomer M. Transferring from an acute hospital and settling into a subacute facility: the experience of patients with dementia. Int J Older People Nursing. 2012;7(1):57–64.
Digby R, Bloomer MJ. People with dementia and the hospital environment: the view of patients and family carers. Int J Older People Nursing. 2014;9(1):34–43.
Gilmour JA, Huntington AD. Finding the balance: Living with memory loss. Int J Nurs Pract. 2005;11(3):118–24.
Goodman C, Amador S, Elmore N, Machen I, Mathie E. Preferences and priorities for ongoing and end-of-life care: A qualitative study of older people with dementia resident in care homes. Int J Nurs Stud. 2013;50(12):1639–47.
Hulko W. From ‘not a big deal’ to ‘hellish’: Experiences of older people with dementia. J Aging Stud. 2009;23(3):131–44.
Johannessen A, Möller A. Experiences of persons with early-onset dementia: A qualitative study. Dementia. 2011;12(4):410–24.
Lawrence V, Samsi K, Banerjee S, Morgan C, Murray J. Threat to valued elements of life: the experience of dementia across three ethnic groups. Gerontologist. 2011;51(1):39–50.
Mazaheri M, Eriksson LE, Nasrabadi AN, Sunvisson H, Heikkilä K. Experiences of dementia in a foreign country: qualitative content analysis of interviews with people with dementia. BMC Public Health. 2014;14(1):794.
Mok E, Lai CKY, Wong FLF, Wan P. Living with early-stage dementia: the perspective of older Chinese people. J Adv Nurs. 2007;59(6):591–600.
Molyneaux VJ, Butchard S, Simpson J, Murray C. The co-construction of couplehood in dementia. Dementia. 2012;11(4):483–502.
Mushi D, Rongai A, Paddick S-M, Dotchin C, Mtuya C, Walker R. Social representation and practices related to dementia in Hai District of Tanzania. BMC Public Health. 2014;14(1):260.
Öhman A, Nygård L. Meanings and Motives for Engagement in Self-Chosen Daily Life Occupations among Individuals with Alzheimer's Disease. OTJR. 2005;25(3):89–97.
Pesonen H-M, Remes AM, Isola A. Diagnosis of dementia as a turning point among Finnish families: A qualitative study. Nurs Health Sci. 2013;15(4):489–96.
Pipon-Young FE, Lee KM, Jones F, Guss R. I’m not all gone, I can still speak: The experiences of younger people with dementia. An action research study. Dementia. 2012;11(5):597–616.
Rostad D, Hellzén O, Enmarker I. The meaning of being young with dementia and living at home. Nurs Rep. 2013;3:1.
Samsi K, Manthorpe J. Everyday decision-making in dementia: findings from a longitudinal interview study of people with dementia and family carers. Int Psychogeriatr. 2013;25(6):949–61.
Acknowledgement
We would like to thank university librarian Marit Gjone Sandsleth for providing essential help and advice for the computer-aided search.
Funding
Each author’s employer has funded the work conducted in this study. No external funding or grant were used to perform the work.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Author information
Authors and Affiliations
Contributions
All authors contributed substantially and according to the ICMJE guidelines to be recognized as authors. Study concept and design: SE and EKG. Data acquisition: SE in cooperation with librarian Mari Gjone Sandsleth. Identification of studies: LHF, EKG, KS, LKJ, ASH, SE. Quality assessment of studies: LHF, EKG, KS, LKJ, ASH, SE. Data analysis and interpretation: LHF and SE in cooperation EKG, KS, LKJ and ASH. Manuscript preparation: LHF, KS and SE. Manuscript editing: LHF, EKG, KS, LKJ, ASH, SE. All authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Authors’ information
Not applicable
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Førsund, L.H., Grov, E.K., Helvik, AS. et al. The experience of lived space in persons with dementia: a systematic meta-synthesis. BMC Geriatr 18, 33 (2018). https://doi.org/10.1186/s12877-018-0728-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-018-0728-0