
Abstract
Background
The aim of our study was to investigate the prevalence and natural long-term progression of gallbladder polyps in a random sample of the general population.
Methods
Four hundred and thirteen subjects (190 women, 223 men; aged 29–75 years) were studied first in 2002 and again eleven years later in 2013. All subjects were interviewed using a standardised questionnaire, anthropometric data were recorded, and an abdominal ultrasound scan was carried out.
Results
The prevalence of gallbladder polyps was 6.1% (115/1880) in the 2002 study and 12.1% (50/413) in the 2013 follow-up study. After eleven years, 36 subjects (8.7%, 36/413) had developed new polyps, thirteen subjects (48.1%, 13/27) no longer had gallbladder polyps, and 14 subjects (51.9%, 14/27) still had polyps. The number of polyps had increased in six of these subjects (43%, 6/14), decreased in a further six (43%, 6/14), and remained unchanged in two (14%, 2/14). The mean polyp size was 4.7 mm (± 2.2 mm, range 2–20 mm) in 2002 and 4.0 mm (± 1.9 mm, range 0.5–11 mm) at follow-up. A decrease in polyp size was noted in seven (50%) of the 14 subjects, an increase in size in five subjects (35.7%), and no change in two subjects (14.3%). The shape of the polyps had changed from pedunculated to sessile in two subjects (14.3%, 2/14) and from sessile to pedunculated in one subject (7.1%, 1/14).
Conclusions
In long-term follow-up, the prevalence of gallbladder polyps increased, with new lesions developing in 8.7% of the population. Polyps persisted in 51.9% of the subjects who had them in the original study and disappeared in the other 48.1%.
Similar content being viewed by others

Background
Gallbladder polyps are a common incidental finding on abdominal ultrasonography [1, 2]. The growth and management algorithm of small polyps measuring less than 10 mm remained unclear for a long time [1, 3, 4]. In 2017 there were established current guidelines on the treatment and follow-up of gallbladder-polyps [5]. Earlier studies have given very different figures for prevalence, ranging from 0.32 to 26.5% [6, 7]. This discrepancy can be attributed mainly to the differences in study populations and study designs, which greatly restrict the possibilities of comparison. Ultrasound studies on random population samples in Germany have given prevalences of 1.4 and 6.1% [8, 9].
At the present time, only a limited number of studies addressing the long-term progression of gallbladder polyps in non-selected populations are available [2, 3, 7,8,9,10,11,12,13,14,15,16,17,18,19,20]. One follow-up study in a random population sample over an observation period of 30 months showed that 81% of the polyps did not change in size, while 14% had increased and 5% had decreased. At follow-up, gallbladder polyps were no longer demonstrated in 23% of the subjects [8]. After 84 months, 77% of the polyps investigated were the same size, while 8% had become smaller [8].
The aim of our study was to investigate the prevalence and natural long-term progression of gallbladder polyps in a random sample of the general population.
Methods
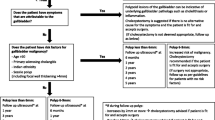
The original Echinococcus multilocularis in Leutkirch (EMIL) study in the general population was carried out in 2002 [21]. In that year, 4000 people aged between 10 and 65 years randomly selected from the residents’ registration office in Leutkirch were contacted for the study, of whom 2445 subjects formed the study population. In 2013, following data analysis and matching cases and controls according to gender, age, body mass index (BMI), and the presence or absence of hepatic steatosis, we recruited a subpopulation of 484 out of the original EMIL subjects for the follow-up study. After persons with incomplete datasets had been excluded, we ultimately had an EMIL subpopulation of 413 subjects aged between 29 and 75 years taking part in the follow-up study (Fig. 1). Participation was voluntary. The follow-up study population consisted of 190 (46%) women and 223 (54%) men (Table 1). Using a standardised questionnaire, we asked the subjects about personal details, leisure activities, past medical history, dietary habits, smoking, alcohol consumption and recreational drug use, and family history. Height and weight were measured on the spot. Each subject had an ultrasound scan of the upper abdomen. The gallbladder was measured in three planes, the wall was described as unremarkable or thickened (thickening > 3 mm), and the lumen examined for sludge, stones and polyps. If stones or polyps were detected, we documented the number, site, maximum size in three planes, presence of acoustic shadowing, echogenicity, shape, and contours. Further examinations such as computed tomography scanning or histological analysis have not been performed. It isn’t known whether subjects underwent cholecystectomy in the course.

Flow chart showing the inclusion and exclusion of subjects in the gallbladder polyp study from the random sample of the general population (EMIL-I study in 2002 and follow-up EMIL-II study in 2013)
The statistical analysis was performed with SAS Version 9.2. Dichotomous variables as well as variables on ordinal and nominal scales were first presented descriptively. After the presentation of sites and extent of distribution, we calculated the age-specific and gender-specific prevalence rates.
Results
Prevalence of gallbladder polyps
The prevalence of gallbladder polyps was 6.1% (115/1880 subjects) in the original 2002 study: 6.2% for women and 6.0% for men. There was a trend towards an increasing prevalence of polyps with age, although the rate was already somewhat elevated in the group aged 31–40 (Fig. 2).

Relative frequency of gallbladder polyps according to age in the original EMIL study in 2002 and the follow-up study in 2013
In the 2013 follow-up study, the prevalence was 12.1% (50/413 subjects) with women and men being affected in relatively equal proportions (12.1%). The highest prevalence was seen in the 31–40 age group, but there was also an upwards trend with increasing age in the older age groups (Fig. 2). The mean age of the cohort (n = 413) was 57.8 ± 11.7 years. The youngest person was 31 years of age and the oldest 74. There were 23 subjects (5.6%) in the 31–40 age group and 124 (30.0%) in the over-65 s. Most of the patients (167; 40.4%) were aged 51–65 years. The mean BMI (body mass index) was 29.2 ± 4.3, ranging from 20.7 to 41.1 (Table 1).
Progression of gallbladder polyps
In the 2013 follow-up study, we examined 27 subjects who had already had gallbladder polyps in 2002. Fourteen of these subjects (51.9%) still had polyps, while 13 subjects (48.1%) no longer had any evidence of gallbladder polyps on ultrasound scanning. In addition, 36 subjects (8.7%) who did not have polyps in 2002 had developed them by 2013.
The natural progression of gallbladder polyps could be observed in the 14 patients who had polyps in the original study in 2002 and also participated in 2013 (referred to in the following as ‘follow-up subjects’). The number of polyps increased in six subjects (42.9%), decreased in a further six subjects (42.9%), and was unchanged in the remaining two (14.3%). Polyp size decreased in seven subjects (50.0%), increased in five subjects (35.7%), and stayed the same in the other two (14.3%).
Ultrasound scan characteristics
In general, the majority of polyps were hyperechoic. Over time, the echogenicity had changed from hyperechoic to hypoechoic in one subject. Table 2 shows the observations made in the 14 follow-up subjects with respect to the shape of the polyps. In eight of the 14 subjects (57.1%) the polyps had not changed in shape. The description of the polyps had changed from pedunculated to sessile in two subjects (14.3%) and vice versa from sessile to pedunculated in one subject (7.1%). In two cases, polyps identified in 2013 were described as pedunculated, although it had not been possible to assess them in the original 2002 study. One polyp, reported as pedunculated in the original study could not be assessed in 2013. The gallbladder polyps mostly showed regular contours but had become irregular in two of the subjects in the follow-up group.
Discussion
In comparison with other population-based studies, the EMIL follow-up study in 2013 showed a higher prevalence (12.1%) of gallbladder polyps. Most of the earlier population-based studies come from Asia [22,23,24,25,26,27]. Population-based studies from Germany have so far yielded prevalences of 1.4% (incidental findings when ascertaining the prevalence of gallbladder stones) and 6.1% [8, 9]. In Europe, apart from these German studies, only Jørgensen in Denmark has determined population-based prevalences of 4.6 and 4.3% in the up to 60-year-old men and women, respectively, and of 5.9 and 5.8% in 70-year-old men and women [28, 29]. Comparing the population-based studies worldwide, a general increase in the prevalence can be seen over the years from 1990 to date: Jørgensen (1990) 4.6%/4.3%, Segawa (1992) 5.6%, Chen (1997) 6.9%, Okamoto (2002) 8.1%, Kratzer (2010) 6.1%, Park (2013) 8.5% and EMIL (2013) 12.1% [9, 22, 24,25,26,27,28,29]. In the first instance, this increase may be due to improvements in the ultrasound technology.
Apart from the general population-based studies, there have been many studies on selected populations, for example, during healthcare screening [16, 27, 30,31,32], oil industry workers in China [33], officers aged between 48 and 56 years in Japan [34], and patient populations [2, 6, 15, 35,36,37]. While population-based studies have given prevalences in the range of 1.4 to 8.5% – and 12.1% in the EMIL follow-up study – studies on selected subjects have given values between 6.1 and 12.3%, while studies on patient populations have given values of 0.06 to 26.5%. The majority of the values obtained have been below 7% [2, 6,7,8,9, 12, 14,15,16, 22,23,24,25,26,27,28,29,30,31, 33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66]. The large differences in the results may be attributed in part to different study designs and methods. Previous prevalence data obtained by ultrasound ranged from 0.32 to 9.96%; data obtained by surgery and pathology were between 0.06 and 21.3% and tended to be somewhat higher than the ultrasound data [2, 6, 8, 9, 12, 15, 16, 22,23,24,25,26,27,28,29,30,31, 33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66]. This deviation may demonstrate the fact that not all existing polyps were detected on ultrasound scans in the past, as the technology was not so highly developed. The results of the EMIL follow-up, with 12.1%, are in the same order of magnitude as the surgical/pathological results. For example, Toda et al. found a polyp prevalence of 14.8% and the study by Furukawa et al. gave a corresponding figure of 10.4% [42, 63].
In the EMIL study, we did not find a gender-specific difference in the prevalence of polyps. Csendes and co-workers, as well as Cantürk et al. also found the prevalence to be similar in men and women [3, 35]. In our study, the 31–40 age group showed the highest prevalence at 17.4%. In the original study, too, the group aged 31–40 at that time had a higher prevalence than the following age group. Lin and co-workers reported an increased frequency of gallbladder polyps in 41 to 50-year-olds [31]. Hayashi et al. found the highest prevalence in 40 to 49-year-old men and 50 to 59-year-old women [30]. The presence of gallbladder polyps therefore particularly affects middle-aged people. One explanation for the reduced prevalence of polyps in the older age groups compared with the middle-aged group may be the simultaneous occurrence of gallstones, which possibly leads to the automatic removal of the polyps [32, 35].
In total, 27 subjects with gallbladder polyps from the original study in 2002 were also examined in 2013: polyps were still present in 14 (51.9%) of these subjects but were no longer to be found in 13 (48.1%). Corwin et al. determined a similarly high proportion of polyps that had disappeared (34%) in their follow-up study after 65 months [13]. One German study showed that 22.6% of the polyps had disappeared after 30 months [8], while the follow-up study by Csendes et al. found that 18% of gallbladder polyps could no longer be demonstrated after 48 months [3].
The mean size of the polyps in our 14 follow-up-subjects was slightly larger in 2013 (4.7 ± 1.9 mm) than in 2002 (4.1 ± 1.1 mm) [9]. Collett and Choi et al. also published results showing a maximum growth of about one millimetre [12, 32]. Just as fewer polyps (35.7%) had increased in size and a greater proportion (50%) had reduced in size in the EMIL study, studies carried out in England by Cairns et al. and Corwin et al. showed a similar picture [10, 13]. Most other follow-up-studies have shown that the diameter does not change in the majority of polyps. For example, Park et al. found 75% unchanged, 15% enlarged and 10% decreased in size [16]. Colecchia and co-workers reported polyps that were 91% unchanged, 5.7% enlarged and 3.8% decreased in size [11]. In contrast, Wolpers published findings showing that in subjects with multiple polyps only 11% remained unchanged after a period of about seven years: 28% had grown and 13% had shrunk [7]. The EMIL follow-up study in 2013 also showed a higher proportion of multiple gallbladder polyps. These correlations allow us to conclude that the small number of subjects with unchanged gallbladder polyps could simply be due to the larger number of polyps per subject.
At the end of the follow-up period in the EMIL study, the number of gallbladder polyps was the same in only two subjects (14.3%). Half of the remaining follow-up subjects had more (42.9%) gallbladder polyps in 2013 while the other half (42.9%) had fewer polyps. Other follow-up-studies – provided that data on the number of polyps over time are available – have shown an increase rather than a decrease in the number of polyps [3, 7, 10]. Wolpers, for example, reported an increase in number in 21% of subjects with multiple polyps compared with a reduction in number in 14% [7]. After 48 and 96 months, Csendes et al. found an increase in 20 and 24% of subjects, respectively, while the corresponding figures for a reduction in the number of polyps were just 6 and 3% [3].
Observation of the gallbladder polyps with respect to echogenicity, shape, and contours showed very little change with time. Echogenicity changed from hyperechoic to hypoechoic in only one subject, and the previously regular contours became irregular in two subjects.
The polyps changed from pedunculated to sessile in two of the 14 subjects and, vice versa in three cases, with polyps becoming pedunculated which had previously been sessile or impossible to assess.
These changes may be attributed to improvements in ultrasound technology with greater resolution. Our follow-up population is too small for us to make more precise statements on the relevance of these changes. Previous follow-up studies on gallbladder polyps have not recorded any data on changes in echogenicity, shape or contours with time, so that we are unable to say more at the present time [2, 3, 7,8,9,10,11,12,13,14,15,16,17,18,19,20].
Conclusions
In our 2013 follow-up study, we found the prevalence of gallbladder polyps to be considerably higher than in the original 2002 study. Looking at other studies as well, there has been a progressive increase in the prevalence over the years from 1990 to the present. One possible reason for the increase may be improvements in ultrasound technology. In the long term, new polyps developed in 8.7% of our study population, existing polyps persisted in 51.9% of subjects and disappeared in 48.1%. The improved ultrasound technology seems to be the reason for the higher prevalence. We have confirmed a higher prevalence in middle-aged subjects.
Abbreviations
- %:
-
percent
- BMI:
-
Body mass index
- EMIL:
-
Echinococcus multilocularis in Leutkirch
- mm:
-
millimetre
- SAS:
-
Statistical analysis system
References
Arikanoglu Z, Taskesen F, Aliosmanoglu I, Gul M, Gumus H, Celik Y, Tas I, Keles A, Girgin S. Continuing diagnostic and therapeutic challenges in gallbladder polyps. Am Surg. 2013;79:446–8.
Moriguchi H, Tazawa J, Hayashi Y, Takenawa H, Nakayama E, Marumo F, Sato C. Natural history of polypoid lesions in the gall bladder. Gut. 1996;39:860–2.
Csendes A, Burgos AM, Csendes P, Smok G, Rojas J. Late follow-up of polypoid lesions of the gallbladder smaller than 10 mm. Ann Surg. 2001;234:657–60.
Babu BI, Dennison AR, Garcea G. Management and diagnosis of gallbladder polyps: a systematic review. Langenbeck's Arch Surg. 2015;400:455–62.
Wiles R, Thoeni RF, Barbu ST, Vashist YK, Rafaelsen SR, Dewhurst C, Arvanitakis M, Lahaye M, Soltes M, Perinel J, Roberts SA. Management and follow-up of gallbladder polyps: joint guidelines between the European Society of Gastrointestinal and Abdominal Radiology (ESGAR), European Association for Endoscopic Surgery and other interventional techniques (EAES), International Society of Digestive Surgery - European federation (EFISDS) and European Society of Gastrointestinal Endoscopy (ESGE). Eur Radiol. 2017;27:3856–66.
Pandey M, Khatri AK, Sood BP, Shukla RC, Shukla VK. Cholecystosonographic evaluation of the prevalence of gallbladder diseases. A university hospital experience. Clin Imaging. 1996;20:269–72.
Wolpers C. Gallenblasenpolypen und Gallenblasensteine. Dtsch Med Wochenschr. 1989;114:1905–12.
Kratzer W, Haenle MM, Voegtle A, Mason RA, Akinli AS, Hirschbuehl K, Schuler A, Kaechele V. The Roemerstein study group: Ultrasonographically detected gallbladder polyps: a reason for concern? A seven-year follow-up study. BMC Gastroenterol. 2008;8.
Kratzer W, Schmid A, Akinli AS, Thiel R, Mason RA, Schuler A, Haenle MM: Gallenblasenpolypen: Prävalenz und Risikofaktoren. Gallbladder Polyps: Prevalence and Risk Factors. Ultraschall in Med 2011;32:68–73.
Cairns V, Neal CP, Dennison AR, Garcea G. Risk and cost-effectiveness of surveillance followed by cholecystectomy for gallbladder polyps. Arch Surg. 2012;147:1078–83.
Colecchia A, Larocca A, Scaioli E, Bacchi-Reggiani ML, Di Biase AR, Azzaroli F, Gualandi R, Simoni P, Vestitio A, Festi D. Natural history of small gallbladder polyps is benign: evidence from a clinical and Pathogenetic study. Am J Gastroenterol. 2009;104:624–9.
Collett JA, Allan RB, Chisholm RJ, Wilson IR, Burt MJ, Chapman BA. Gallbladder polyps: prospective study. J Ultrasound Med. 1998;17:207–11.
Corwin MT, Siewert B, Sheiman RG, Kane RA. Incidentally detected gallbladder polyps: is follow-up necessary? – long-term clinical and US analysis of 346 patients. Radiology. 2011;258:277–82.
Eelkema HH, Hodgson JR, Stauffer MH. Fifteen-year follow-up of polypoid lesions of the gall bladder diagnosed by cholecystography. Gastroenterology. 1962;42:144–7.
Heyder N, Günter E, Giedl J, Obenauf A, Hahn EG. Polypoide Läsionen der Gallenblase. Dtsch Med Wschr. 1990;115:243–7.
Park JK, Yoon YB, Kim YT, Ryu JK, Yoon WJ, Lee SH, Yu SJ, Kang HY, Park MJ. Management strategies for gallbladder polyps: is it possible to predict malignant gallbladder polyps? Gut and Liver. 2008;2:88–94.
Park JY, Hong SP, Kim YJ, Kim HJ, Kim HM, Cho JH, Park SW, Song SY, Chung JB, Bang S. Long-term follow-up of gallbladder polyps. J Gastroenterol Hepatol. 2008;24:219–22.
Pedersen MRV, Dam C, Rafaelsen SR. Ultrasound follow-up for gallbladder polyps less than 6 mm may not be necessary. Dan Med J. 2012;59:A4503.
Shin SR, Lee JK, Lee KH, Lee KT, Rhee JC, Jang KT, Kim SH, Choi DW. Can the growth rate of a gallbladder polyp predict a neoplastic polyp? J Clin Gastroenterol. 2009;43:865–8.
Sugiyama M, Atomi Y, Yamato T. Endoscopic ultrasonography for differential diagnosis of polypoid gall bladder lesions: analysis in surgical and follow up series. Gut. 2000;46:250–4.
Haenle MM, Brockmann SO, Kron M, Bertling U, Mason RA, Steinbach G, Boehm BO, Koenig W, Kern P, Piechotowski I, Kratzer W. EMIL-study group: overweight, physical activity, tobacco and alcohol consumption in a cross-sectional random sample of German adults. BMC Public Health. 2006;6:233.
Chen CY, Lu CL, Chang FY, Lee SD. Risk factors for gallbladder polyps in the Chinese population. Am J Gastroenterol. 1997;92:2066–8.
Okamoto M, Okamoto H, Kitahara F, Kobayashi K, Karikome K, Miura K, Matsumoto Y, Fujino MA. Ultrasonographic evidence of Association of Polyps and Stones with gallbladder Cancer. Am J Gastroenterol. 1999;94:446–50.
Okamoto M, Yamagata Z, Takeda Y, Yoda Y, Kobayashi K, Fujino MA. The relationship between gallbladder disease and smoking and drinking habits in middle-aged Japanese. J Gastroenterol. 2002;37:455–62.
Park EJ, Lee HS, Lee SH, Chun HJ, Kim SY, Choi YK, Ryu HJ, Shim KW. Association between metabolic syndrome and gallbladder polyps in healthy Korean adults. J Korean Med Sci. 2013;28:876–80.
Segawa K, Arisawa T, Niwa Y, Suzuki T, Tsukamoto Y, Goto H, Hamajima E, Shimodaira M, Ohmiya N. Prevalence of gallbladder polyps among apparently healthy Japanese: Ultrasonographic study. Am J Gastroenterol. 1992;87:630–3.
Choi YS, Do JH, Seo SW, Lee SE, Oh HC, Min YJ, Kang H. Prevalence and risk factors of gallbladder polypoid lesions in a healthy population. Yonsei Med J. 2016;57:1370–5.
Jørgensen T, Jensen KH. Polyps in the gallbladder. A prevalence study. Scand J Gastroenterol. 1990;25:281–6.
Jørgensen T, Kay L, Schultz-Larsen K. The epidemiology of gallstones in a 70-year-old Danish population. Scand J Gastroenterol. 1990;25:335–40.
Hayashi Y, Liu JH, Moriguchi H, Takenawa H, Tazawa J, Nakayama E, Marumo F, Sato C. Prevalence of polypoid lesions of the gallbladder in urban and rural areas of Japan: comparison between 1988 and 1993. J Clin Gastroenterol. 1996;23:158–9.
Lin WR, Lin DY, Tai DI, Hsieh SY, Lin CY, Sheen IS, Chiu CT. Prevalence of and risk factors for gallbladder polyps detected by ultrasonography among healthy Chinese: analysis of 34669 cases. J Gastroenterol Hepatol. 2008;23:965–9.
Choi SY, Kim TS, Kim HJ, Park JH, Park DI, Cho YK, Sohn CI, Jeon WK, Kim BI. Is it necessary to perform prophylactic cholecystectomy for asymptomatic subjects with gallbladder polyps and gallstones? J Gastroenterol Hepatol. 2010;25:1099–104.
Mao YS, Mai YF, Li FJ, Zhang YM, Hu KM, Hong ZL, Zhu ZW. Prevalence and risk factors of gallbladder polypoid lesions in Chinese petrochemical employees. World J Gastroenterol. 2013;19:4393–9.
Shinchi K, Kono S, Honjo S, Imanishi K, Hirohata T. Epidemiology of gallbladder polyps: an Ultrasonographic study of male self-defense officials in Japan. Scand J Gastroenterol. 1994;29:7–10.
Cantürk Z, Sentürk Ö, Cantürk NZ, Anik YA. Prevalence and risk factors for gall bladder polyps. East African Med J. 2007;84:336–41.
Konstantinidis IT, Bajpai S, Kambadakone AR, Tanabe KK, Berger DL, Zheng H, Sahani DV, Lauwers GY, Fernandez-del Castillo C, Warshaw AL, Ferrone CR. Gallbladder lesions identified on ultrasound. Lessons from the last 10 years. J Gastrointest Surg. 2012;16:549–53.
Lorenz R, Beyer D, Junginger T, Arnold G. Bildgebende Diagnostik fokaler Läsionen der Gallenblasenwand. Fortschr Roentgenstr. 1982;137:495–502.
Chattopadhyay D, Lochan R, Balupuri S, Gopinath BR, Wynne KS. Outcome of gall bladder polypoidal lesions detected by transabdominal ultrasound scanning: a nine-year experience. World J Gastroenterol. 2005;11:2171–3.
Chijiiwa K, Tanaka M. Polypoid lesion of the gallbladder: indications of carcinoma and outcome after surgery for malignant polypoid lesion. Int Surg. 1994;79:106–9.
Damore LJ, Cook CH, Fernandez KL, Cunningham J, Ellison C, Melvin WS. Ultrasonography incorrectly diagnoses gallbladder polyps. Surg Laparosc Endosc Percutan Tech. 2001;11:88–91.
De Lacey G, Gajjar B, Twomey B, Levi J, Cox AG. Should cholecystography or ultrasound be the primary investigation for gallbladder disease? Lancet. 1984;1:205–7.
Furukawa H, Takayasu K, Mukai K, Inoue K, Kyokane T, Shimada K, Kosuge T, Ushio K. CT evaluation of small polypoid lesions of the gallbladder. Hepatogastroenterology. 1995;42:800–10.
Il'chenko AA, Orlova IN, Bystrovskaia EV, Vasnev EV, Khomeriki SG. Vorob’eva NN: Adenomyomatosis of the gallbladder the analysis of 328 operating cases. Eksp Klin Gastroenterol. 2013;5:114–20.
Koga A, Watanabe K, Fukuyama T, Takiguchi S, Nakayama F. Diagnosis and operative indications for polypoid lesions of the gallbladder. Arch Surg. 1988;123:26–9.
Kozuka S, Tsubone M, Yasui A, Hachisuka K. Relation of adenoma to carcinoma in the gallbladder. Cancer. 1982;50:2226–34.
Levy AD, Murakata LA, Abbott RM, Rohrmann CA. Benign tumors and Tumorlike lesions of the gallbladder and extrahepatic bile ducts: radiologic-pathologic correlation. RadioGraphics. 2002;22:387–413.
Lindström CG. Frequency of gallstone disease in a well-defined Swedish population. A prospective necropsy study in Malmö. Scand J Gastroenterol. 1977;12:341–6.
Maciejewski P, Strzelczyk J. Is gall-bladder polyp equivalent to cancer? An analysis of material from 1196 cholecystectomies – a comparison of the ultrasound and histopathological results. Pol Przegl Chir. 2014;86:218–22.
Mainprize KS, Gould SWT, Gilbert JM. Surgical management of polypoid lesions of the gallbladder. Br J Surg. 2000;87:414–7.
Matłok M, Migaczewski M, Major P, Pędziwiatr M, Budzyński P, Winiarski M, Ostachowski M, Budzyński A, Rembiasz K. Laparoscopic cholecystectomy in the treatment of gallbladder polypoid lesions – 15 years of experience. Pol Przegl Chir. 2013;85:625–9.
Myers RP, Shaffer EA, Beck PL. Gallbladder polyps: epidemiology, natural history and management. Can J Gastroenterol. 2002;16:187–94.
Ochsner SF, Ochsner A. Benign neoplasms of the gallbladder: diagnosis and surgical implications. Ann Surg. 1960;151:630–7.
Oestmann A. Gallenblasenpolypen. Praxis. 2012;101:581–4.
Ozmen MM, Patankar RV, Hengrimen S, Terzi MC. Epidemiology of gallbladder polyps. Letter to the editor. Scand J Gastroenterol. 1994;29:480.
Reck T, Köckerling F, Heyder N, Gall FP. Polypoide Läsionen der Gallenblase - prophylaktische Cholecystektomie? Chirurg. 1992;63:506–10.
Sarkut P, Kilicturgay S, Ozer A, Ozturk E, Yilmazlar T. Gallbladder polyps: factors affecting surgical decision. World J Gastroenterol. 2013;28:4526–30.
Spaziani E, Di Filippo A, Picchio M, Lucarelli M, Pattaro G, De Angelis F, Francioni P, Vestri A, Petrozza V, Narilli F, Drudi F, Stagnitti F. Prevalence of adenoma of gallbladder, ultrasonographic and histological assessment in a retrospective series of 450 cholecystectomy. Ann Ital Chir. 2013;84:159–64.
Ten Eyck EA. Fixed defects in the Gallbladder Wall. Radiology. 1958;71:840–6.
Terada T. Histopathologic features and frequency of gall bladder lesions in consecutive 540 cholecystectomies. Int J Clin Exp Pathol. 2013;6:91–6.
Terzi C, Sökmen S, Seçkin S, Albayrak L, Uğurlu M. Polypoid lesions of the gallbladder: report of 100 cases with special reference to operative indications. Surgery. 2000;127:622–7.
The Southern Surgeons Club. A prospective analysis of 1518 laparoscopic cholecystectomies. New Engl J Med. 1991;324:1073–8.
Tinsley AR, Mulkerin LE, Van der Linde JM, Todd DW. Polypoid lesions of the Acalculous gallbladder. South Med J. 1975;68:958–62.
Toda K, Souda S, Yoshikawa Y, Momiyama T, Ohshima M. Significance of laparoscopic excisional biopsy for polypoid lesions of the gallbladder. Surg Laparosc Endosc. 1995;5:267–71.
Wiles R, Varadpande M, Muly S, Webb J. Growth rate and malignant potential of small gallbladder polyps – systematic review of evidence. Surgeon. 2014;12:221–6.
Xu Q, Tao LY, Wu Q, Gao F, Zhang FL, Yuan L, He XD. Prevalences of and risk factors for biliary stones and gallbladder polyps in a large Chinese population. HPB. 2012;14:373–81.
Yang HL, Kong L, Hou LL, Shen HF, Wang Y, Gu XG, Qin JM, Yin PH, Li Q. Analysis of risk factors for polypoid lesions of gallbladder among health examinees. World J Gastroenterol. 2012;18:3015–9.
Acknowledgements
Members of the EMIL I and II study groups in alphabetical order: Adler G, Armsen A, Banzhaf H-M, Bauerdick M, Bernhardt P, Bertling U, Boehm BO, Brandner BO, Brockmann SO, Deckert M, Dingler C, Eggink S, Fuchs M, Gaus W, Goussis H, Gruener B, Gruenert A, Haenle MM, Hampl W, Haug C, Hay B, Heitz L, Huetter M-L, Iftikhar N, Imhof A, Kaltenbach T, Kern P, Kimmig P, Kirch A, Klass D, Koenig W, Kratzer W, Kron M, Manfras B, Meitinger K, Mertens T, Oehme R, Pfaff G, Piechotowski I, Reuter S, Romig T, von Schmiesing AFA, Stanosek S, Steinbach G, Tourbier M, Voegtle A, Walcher T, Wolff S, Schlingeloff P.
Funding
Not applicable.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Consortia
Contributions
LH, JS and WK designed the study. LH, TG, WK and JS collected the data. The analysis was done by WK and JS. LH, WK, TG and JS wrote the paper. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethics Committee of the Baden-Württemberg Medical Association approved both the EMIL-I study in 2002 and the EMIL-II study in 2013 (Application numbers 133/02 and 244/13, respectively). The participating patients gave their written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Heitz, L., Kratzer, W., Gräter, T. et al. Gallbladder polyps – a follow-up study after 11 years. BMC Gastroenterol 19, 42 (2019). https://doi.org/10.1186/s12876-019-0959-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-019-0959-3