
Abstract
Children with physical disabilities often have limited performance in daily activities, hindering their physical development, social development and mental health. Therefore, rehabilitation is essential to mitigate the adverse effects of the different causes of physical disabilities and improve independence and quality of life. In the last decade, robotic rehabilitation has shown the potential to augment traditional physical rehabilitation. However, to date, most robotic rehabilitation devices are designed for adult patients who differ in their needs compared to paediatric patients, limiting the devices’ potential because the paediatric patients’ needs are not adequately considered. With this in mind, the current work reviews the existing literature on robotic rehabilitation for children with physical disabilities, intending to summarise how the rehabilitation robots could fulfil children’s needs and inspire researchers to develop new devices. A literature search was conducted utilising the Web of Science, PubMed and Scopus databases. Based on the inclusion–exclusion criteria, 206 publications were included, and 58 robotic devices used by children with a physical disability were identified. Different design factors and the treated conditions using robotic technology were compared. Through the analyses, it was identified that weight, safety, operability and motivation were crucial factors to the successful design of devices for children. The majority of the current devices were used for lower limb rehabilitation. Neurological disorders, in particular cerebral palsy, were the most common conditions for which devices were designed. By far, the most common actuator was the electric motor. Usually, the devices present more than one training strategy being the assistive strategy the most used. The admittance/impedance method is the most popular to interface the robot with the children. Currently, there is a trend on developing exoskeletons, as they can assist children with daily life activities outside of the rehabilitation setting, propitiating a wider adoption of the technology. With this shift in focus, it appears likely that new technologies to actuate the system (e.g. serial elastic actuators) and to detect the intention (e.g. physiological signals) of children as they go about their daily activities will be required.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Mobility and exploration are essential in children’s development and contribute towards cognitive, physical, social and emotional development. However, children with physical disabilities present limitations when performing activities autonomously, which hinders their typical development [1]. Ongoing paediatric physical disability arose from many different causes, including neurological disorders like cerebral palsy (CP) [2], Stroke [3] and acquired brain injury (ABI) [4], neuromuscular diseases such as Duchenne muscular dystrophy (DMD) [5] and spinal muscular atrophy (SMA) [6], or traumatic injuries [7, 8] (Table 1).
Rehabilitation is essential to help the children recover or maintain functionality when interacting with their environment, improving the quality of life and autonomy [9, 10]. Furthermore, early access to rehabilitation is critical for children while they are in the stage of development. The gait pattern and motor abilities are still malleable [11], intending to reduce the probability of developing more severe levels of disability [12, 13].
The standard therapies to manage the musculoskeletal system’s deterioration and improve and maintain physical ability include passive orthoses, surgery, and physiotherapy [15, 16]. Physiotherapists prescribe, monitor, and guide exercise, which can prevent an unnecessarily sedentary or immobile lifestyle. The most extensively investigated aspect of physiotherapy is the effect of direct interventions on upper or lower limbs. Such interventions often involve intensive stretching and strengthening exercises facilitated by the physiotherapist [2] to improve motor skills. These interventions are often highly labour intensive and can be challenging to perform [17]. Furthermore, the effectiveness of physiotherapy often depends on the experience of the physiotherapist. Thus, it is not easy to achieve optimal consistency and repeatability between rehabilitation sessions [18, 19].
There is a growing interest in robots that can support the patient, the family and the medical professional in a wide range of activities used for the care of people with physical disabilities, for example, companion robots [20, 21], monitoring robots [22] and surgery robots [23], all of them can be considered as healthcare robots.
Healthcare robots can be divided into three main categories, clinical robots, assistive robots and rehabilitation robots [24, 25]. Clinical robots are focus on supportive care and cure process (e.g. help in surgery and diagnosis) in clinical environments; assistive robots primary function is to provide assistive help either to carers or directly to patients either in a hospital or in a specialist care facility (e.g. patient lifting and to assist in routine services); rehabilitation robots are robots design towards restoring the functionality and mobility of people with physical disabilities, in that case, the recovery of mobility could be achieved by assisting the patient during ADLs (e.g. walking and grasping objects) [17, 26] or with physical training therapy [24, 27,28,29,30], and are the main focus of this study.
Rehabilitation therapy for the recovery of mobility based on robots has been proposed as a new procedure for children with physical disabilities [31]. This robot-assisted rehabilitation therapy consists of a mechatronic device that provides highly repetitive and task-specific guided movements autonomously [32, 33]. The use of robots in rehabilitation therapies bring advantages over traditional therapies, as they allow extensive practice in children with substantial disabilities, reduced effort required of therapists during the exercises, and provide a quantitative assessment of the patient’s motor function (e.g. quantitative feedback of range of motion (ROM) and strength with each repetition) [34,35,36,37,38].
Rehabilitation robots are often classified by their mechanical structure and are generally divided into end-effectors and exoskeletons [28, 39]. End-effector devices work by applying forces to the distal segments of limbs, creating what is termed a “mechanical chain” that prompts movements of other parts of the limb generating a pattern of specific activity across different joints. If utilised on a single segment and joint, their simple structure makes it easier to adapt them to many patients and needs less complicated control algorithms. However, it is difficult to isolate specific joints since they produce complex movements that involve the whole limb [40].
Contrarily, robotic exoskeletons could be termed “wearable machines” that mirror the patient’s skeletal structure; therefore, they only move the joint of the limb where the exoskeleton is worn. This approach allows for independent and concurrent control of specific segments of the limb. However, it is essential to adjust the length of sections of the robot to the lengths of the segments of the patient limb. Moreover, when the joint is in motion, the position of the centre of rotation can change, creating discomfort in the user. Thus, increasing the number of degrees of freedom of the robot increases the control algorithm’s complexity, weight, mechanical complexity, and power requirements, making it unattainable for home use [18, 41].
Apart from mechanical structure, robots possess essential elements to ensure the systems’ reliability and robustness [42]. Actuators, training strategy and the Human–computer interface (HCI) are among these essential elements. The actuators play a crucial role because they determine the torque and movement provided by the robot and influence the total weight and compliance of the system [29, 43]. The training strategy and the HCI are an integral part of the robot-assisted rehabilitation since it determines how the patient interacts with the robot and the type of assistance that the robot can provide. Many authors have analysed these last two characteristics as part of the robots control [28, 30, 44]. However, control also involves “low level” considerations that are more related to the internal communication of the components (sensors, structures, microcontrollers, actuators, etc.) at a hardware level rather than how the device interacts with the patient [45,46,47,48,49].
Although multiple devices for the robotic rehabilitation of upper and lower limbs have been developed, at least in a proof-of-concept phase [24, 39, 42, 44, 45, 50, 51], most presented robots were designed for adult users, impeding their use on the paediatric population. For example, commercial exoskeletons are made for a subject 150 cm tall onwards [52], while the average height for a 5-year-old child will be around 110 cm [53].
However, to develop technology planned to be used on the paediatric population is not only a matter of reducing the size of the robots. But it should be tailored to their own capabilities and goals that differ from those of the adults. For instance, a simple downscaling of the robots is not enough as the normalised joint torques on adults are greater than those of a child [54, 55], making them potentially dangerous when used on small children. Additionally, in the case of children, as their cognitive abilities are still developing, it could be hard for them to fully understand how the technology works [52, 56]. Hence, it is hard to adapt a robot made for adults to be used by children since the robots do not fulfil the children’s needs [26, 57].
Consequently, to address the children’s needs adequately, it is essential to include them and other stakeholders (e.g. family members, clinicians, and health care providers) during the development process, providing feedback to identify possible issues of importance [1, 43]. Furthermore, it is essential to focus not only on addressing the impairment or limitation in users’ functional abilities, but also on other fundamental needs, like accessibility and aesthetics [58], to avoid the user abandoning the rehabilitation device due to frustration [59].
Despite the progressive development of robotic rehabilitation devices, their application to the paediatric population is still scarce. Consequently, the key features to design an optimal robotic rehabilitation device that better enhance children’s abilities with physical disabilities have not been well defined yet. Based on this framework, this review aims to address the following questions: (1) What are the design requirements for paediatric rehabilitation robots? (2) How does the current technology contribute to achieving the paediatric design requirements? And (3) How do the paediatric conditions impact the device design?
Methods
An in-depth literature search was performed to conduct the review, following the search strategy of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [60].
A literature search was conducted to identify literature associated with the topic based on searches in PubMed, Scopus, and Web of Science, using the combination of the following keywords: (pediatric OR kid* OR child*) AND (aid OR assist* OR improve* OR augment* OR enhance* OR reinforce* OR therap* OR rehabilitation) AND (active ortho* OR exoskeleton* OR wearable robot* OR portable robot* OR robot* suit OR robot*) AND (movement OR motion OR walk* OR gait OR grasp* OR handl*). To make our search as complete as possible, a search through the university library databases was also conducted.
After the preliminary search, the following inclusion and exclusion criteria to narrow the literature search were used. The inclusion criteria were:
-
1)
Studies involving robotic devices for robot-assisted rehabilitation therapy,
-
2)
Studies involving robotic devices for assessment of patients with Physically disabilities,
-
3)
Studies involving devices designed for children or utilised with a paediatric population (< 18 years old),
-
4)
written in English,
-
5)
full-text articles.
And the exclusion criteria were:
-
1)
Studies that only present software solutions or simulations,
-
2)
Studies involving passive devices (do not have actuators),
-
3)
Studies involving postural change,
-
4)
Studies involving only the adult population and
-
5)
Studies involving robots that do not replace the movement itself (e.g. wheelchairs).
Findings
The outcome of this literature review is compiled in the following sections:
-
An overview of the literature search,
-
the paediatric robotic rehabilitation design requirements,
-
an analysis of the type of robots used in paediatric robotic rehabilitation;
-
the actuators to drive the robots;
-
training strategy of the robots;
-
the human–computer interface of the assistive systems, and
-
the treated conditions in children with physical disabilities.
Literature search
Based on the keywords mentioned in the methods section, 1604 publications were found, with:
-
811 publications from Web of Science,
-
547 publications from PubMed,
-
241 from Scopus, and
-
5 from a search on the University library.
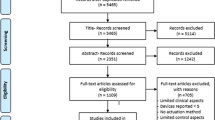
First, a check was made for duplicated publications. After this process, the abstracts of 1248 publications were screened, and 301 titles were selected for full-text reading. After carefully applying the inclusion–exclusion criteria to the full read papers, 206 publications were selected. Among the chosen publications, 10 were reviews, 42 only discussed a section of the design process of the rehabilitation robot, 138 presented a clinical application, and 16 included the design process plus a clinical application (Fig. 1 shows a flow diagram that illustrates the process of the selection of the papers).

Literature search flow diagram
The ten review articles examined a variety of rehabilitation robots for children with physical disabilities. They were focused on children with neurological problems (e.g. CP, ABI, and Stroke) or SCI and only investigated their use as part of physical therapy. In Fasoli et al. [35], Meyer et al. [61], and Bayon et al. [62], the robot assistive therapies for children with CP were examined. Vova et al. [63] reviewed the efficacy of functional electrical stimulation and exoskeletons in gait training to improve motor function and gait pattern in children with CP. Zwicker et al. [64] reviewed the efficiency of robot-assisted treadmill training compared to traditional treadmill training in children with CP. Chen et al. [65] examined the effectiveness of various devices for upper limb robotic therapy on children with CP. The effects of robotic gait training practices in individuals with CP were investigated in Carvalho et al. [31]. Falzarano et al. [10] and Mahamud et al. [66] investigated upper and lower limb rehabilitation devices for neurological diseases. Dannenberg et al. [67] compared different locomotor training, including robotic training, in children with SCI. Compared with the previous reviews, this work analyses a broader range of aspects of paediatric rehabilitation robots, focused on the design parameters to fulfil the paediatric needs and how the technology and different conditions affect the robot design.
Paediatric robotic rehabilitation design requirements
Fifteen different requirements were identified (Table 2). The requirements are based on those proposed by Batavia and Hammer for assistive devices [68] and expanded by proposed requirements for paediatric rehabilitation devices highlighted by Weightman et al. [69], Bützer et al. [26] and Keller et al. [57]. In paediatric rehabilitation, it was apparent that the stakeholder’s needs related to operability, weight, safety, and motivation factors were relevant.
In paediatric rehabilitation devices, operability is critical as children are in a continuous development phase during which their bodies, cognitive capabilities and physical abilities (e.g. skill levels) are changing, making them a “heterogeneous population” [52, 70]. Consequently, the device must adapt to different children’s abilities and sizes [71].
An important consideration is that the robot’s weight could obstruct the movement pattern of the limb and increase the child’s energy consumption [72, 73]. Furthermore, due to their musculoskeletal system’s immature development, their muscle strength and joint torque generation may not be adequate to assist in the movement being undertaken [74].
Concerning safety, children often cannot adequately assess the hazards of using complex technological devices [56]. Therefore, it is crucial to design safety mechanisms that minimise risky situations. These should be able to be activated remotely by adults with the child [57]. Furthermore, the use of compliant materials with shock-absorbing features (e.g. elastic elements like spring and Bowden cables) would be beneficial [17].
Finally, motivation is crucial because function recovery is not enough to engage children in the rehabilitation process [75]. Consequently, researchers have used strategies to engage children, like aesthetic designs attractive to the children [26, 76] or a virtual environment where they can interact with virtual objects [77, 78].
Type of robots used on paediatric robotic rehabilitation
Fifty-eight different devices were found that at least had a prototype in action. In Tables 3, 4, 5, 6, 7 (Figs. 2, 3, 4, 5, 6), the rehabilitation robots are presented chronologically and separated by their mechanical structure (end-effector or exoskeleton) and the anatomical part of the body where they are working (upper limb or lower limb). Furthermore, the tables summarise the characteristic features of the selected devices. This tabulated summary constitutes the reference for information provided in subsequent sections.



Reprinted from Biomedical Signal Processing and Control, Vol. 38, F. Chrif et al., Control design for a lower-limb paediatric therapy device using linear motor technology, Page 121, Copyright (2017), with permission from Elsevier


Picture of KPT Cycla [96] an end-effectors rehabilitation robot for both a lower and b upper limbs
In respect of the developmental stage of the devices, the stages were classified into four categories: (1) commercial in the case the robots are available for its commercialisation; (2) clinical trial when the robot undergo a study where the participants were assigned to groups undergoing similar forms of therapy, but at different intensities, using various devices or undergoing various forms of therapy in a different order, aiming to determine the efficiency of therapy [28]; (3) feasibility study when the experiments conducted with a low number of people, often using the prototype of a device, to evaluate its safety and clinical feasibility without showing the potential benefits of the device [28]; (4) prototypes when the robots had not performed any test that involves people. It can be observed that 18 of them reached the commercialisation phase, but only 9 of them are certified by the US Food and Drug Administration (FDA). However, only 5 of the commercially available devices present a paediatric version of the rehabilitation system. In the case of clinical studies, 34 systems conduct at least one clinical trial, 9 presented a feasibility study, and 15 are in the prototyping phase.
From the 58 devices, it was apparent that the majority (67%) were designed or had been redesigned for children. When it comes to the type of robot, more than half were an exoskeleton type structure. In the past five years, there is a trend (Tables 3, 4, 5, 6, 7) for this structure to be more popular with designers than end-effectors for this structure robotic rehabilitation in paediatrics. Additionally, it can be noted that the majority of robots not explicitly designed for children are end-effector devices. In the case of the exoskeletons, the degrees of freedom (DOFs) are related to the number of joints and limbs that are powered. Therefore, it is possible to find exoskeletons with passive DOFs, which means that those joints are not actuated, but allow the free movement of the children´s joint. In contrast, for the end-effectors, the relation of DOFs of the robot and the actuated joints is not linear and depends on the robot’s mechanical design.
Actuators
Rehabilitation robots are moved by devices called actuators. Actuators convert a source of energy (e.g. electrical, thermal, pneumatic) into mechanical motion. Commonly rehabilitation assisted robots are powered by electrical actuators. Among the compared systems in Tables 3, 4, 5, 6, 7, over 93% of the robots used electric motors as the actuator, and about 7% used pneumatic actuators.
Motor actuator
In robotic-assisted rehabilitation, the most common actuators are electrical motors with a rigid power transmission element such as a harmonic drive, ball-screws, timing belts, and chains. Unfortunately, their need for transmission negatively affects the back-drivability, efficiency, safety, size, and mass [97]. Nevertheless, they were likely chosen since they are efficient and easy to control. Some examples of paediatric robotic rehabilitation devices using electrical motors and rigid transmission are the Pedianklebot that used two brushless dc motors and a Rohlix linear traction device [98], the electric motor with timing belt used in ChARMin [99], or the motor with chain transmission used in P.REX [100].
Some researchers [64] used a cable-driven transmission to replace the rigid transmission for an elastic cable to improve the power to weight ratio and lower the inertia over the treated body segment. Examples include the ankle exoskeleton designed by The University of Arizona [101] or TPAD [102], an end-effector robot for gait rehabilitation that used Bowden cables attached to the hip to generate assistive forces. This change in the transmission brings other advantages like modularity, simple architecture and is convenient for reconfiguration, even though they present some disadvantages being unidirectional and difficult to model and control [97, 103, 104].
Following the concept of adding a flexible element in series with the actuator to improve the electric motors’ compliance, serial elastic actuators (SEAs) incorporate an elastic part in series with the electric actuator. This elastic element helps to decrease the actuator’s impedance and inertia and increases the back-drivability allowing better force control, even though they are limited by a large volume, heavy mass and complicated structure [17, 105]. An example of the use of this technology is the ATLAS exoskeleton [106].
Pneumatic actuators
Some authors considered that the mechanical linkage of the electric actuators is too heavy and can generate resistance at the joints, making them inadequate for rehabilitation applications [74, 107]. Instead of electrical motors, they used pneumatic actuators, consisting of a simple air pressurisation mechanism in an expandable chamber, converting the energy from the compressed air to mechanical motion [18, 108, 109]. Their main advantage is improved back-drivability, and they are often lightweight at the site of actuation, have high power density, and can generate fast movements. They are not without limitations; firstly, poor portability because they need external compressors or fluid tanks as the power source. Secondly, it is challenging to create a good model and control strategy due to their nonlinear response to input pressure [109,110,111]. Among the devices analysed that used pneumatic actuators were the Rutgers ankle platform [112] for CP children and two gloves for hand rehabilitation PneuGlove [113] and Gloreha [33].
Training strategy
Devices for robotic rehabilitation may provide different training strategies depending on the type and severity of the patient’s impairment. These can be divided into passive, active, assistive, or resistive [42]. In general, the devices can offer more than one type of training.
In passive training, the force/motion is generated by the robot alone to perform the exercise. The advantage of this training is that patients with minimal muscle activity can receive therapy. For instance, through repetition of a movement, ROM can often be maintained with muscles and joint structures (e.g. ligaments) repeatedly stretched, ultimately maintaining their physiological length. Such movement reduces contractures at joints, which can finally be very useful to caregivers making a notable difference to the ease of transfers (e.g. sitting in a wheelchair to lying in bed). Examples of devices using passive training are Innowalk [114] and Intellistretch [115].
In the active training mode, the patient’s muscle can still generate activity on the affected limb. The robot does not help, making the patients perform the exercise by themselves at least partially. The active mode provides data concerning torques and the ROM produced, allowing assessments before and after therapy/surgery. For instance, Kinarm [116] and Lokomat [117] are devices that can perform active training.
For assistive or active-assistive training, the muscles of the affected body part can still be activated. Therefore, the patient can at least partially perform the exercise or movement without the robot. The assistance will be triggered after a particular event is detected through an HCI, allowing the patients to move further with the robot’s help. Assistive training is relevant as it involves the active participation of the children. Moreover, it improves the physiological responses needed to maintain and increase muscle strength and length, ultimately leading to improved ROM, in which the muscles provide some of the torque required. Due to these advantages, many designers have produced devices that use this training mode. Examples are Pedianklebot [118] and the wrist-robot [119].
As the name implies, the robot applies a force opposing the desired movement in resistive training, making the task more challenging. Resistive training is used to enhance muscle strength in the treated limb. This type of training was employed in the ankle device developed by the University of Arizona [120] and the upper limb end-effector NJIT-RAVR [121].
Human–computer interface (HCI)
The term HCI refers to methodologies to identify the user’s intent to move in the desired direction from different input sources and translate this intention into a command for the robot to move to facilitate the appropriate actions [122]. The designers who report upon the use of an HCI have primarily developed assistive training. Two main types of HCI inputs were identified: those associated with physical interactions and physiological signals [123]. In this aspect, the devices can rely upon only one signal as the input source or use two or more signals as input to start the desired movement.
The main physical interactions used on HCIs to control such robots are Impedance/admittance, body-powered control, and gait phases detectors. Impedance and admittance control are the two most commonly used HCI. They are based on the relation between position and force rather than controlling either force or position explicitly. Impedance control accepts position or velocity as the input and outputs force or torque, and admittance is the opposite of impedance. Hence, force or torque are inputs, and velocity or position the outputs. This method could provide a natural, comfortable, and safe touch interface [122]. Some examples of devices that used this HCI are the NJIT-RAVR [124] and Rehaptic [125] upper limb robots that employed admittance control or the robots for upper and lower limb Inmotion2 [126] and Pedianklebot [118] that applied impedance control.
When the children cannot generate an intention to move with the treated limb, body-powered control is applied. It consists of using the movement of a different body part as the trigger signal to initiate the rehabilitation robot. The main drawback of this approach is that it is hard to control many degrees of freedom due to the activation system’s simplicity. An example of this HCI is the Ekso robot, where the activation was made by moving one’s body weight laterally and then forward to trigger the assistance [127].
In assisted gait, a favoured approach for HCI is the use of gait phase detection. This technique identifies the different gait phases (heel strike, midstance, toe-off, and the swing phase) to apply forces to assist the children’s movement depending on the gait phase. Robots usually perform gait segmentation using inertial measurement units (IMUs) to detect angular velocities of the shank and/or the thigh, or footswitches to detect the foot’s ground reaction forces while the child is walking [128]. The main advantage is that splitting the gait cycle into discrete phases provides enhanced consistency and robustness to an inherently variable process and allows lower-level controllers’ implementation within each phase. The problem is that gait detection should be characterised for every target group, as the physical disability modifies the gait pattern [100]. An example of this type of system is the P.REX exoskeleton which utilised a combination of the footswitch and IMUs to detect the different gait phases to provide different levels of assistance within each phase [100].
Alternatively, for HCI based on physiological signals, Electromyograms (EMG) that measure electrical activity in the muscles and electroencephalograms (EEG), which measure electrical activity in the brain, are the main signals used. They are widely utilised because they can be obtained using non-invasive techniques without the need for medical intervention.
Concerning electromyograms, the primary type is surface electromyography (sEMG), a non-invasive and easy-to-configure procedure in which adhesive electrodes are placed on the skin above the muscle of interest. The benefit of using the EMG signal is that it allows detection of the user’s intent before the movement occurs. The electrical activity can be detected even if it is insufficient to generate movement of a joint. However, sEMG can suffer from contamination of the signal by electromagnetic interference, skin perspiration, movement of electrodes and crosstalk artefacts. Also, for each muscle group of interest, a single EMG channel only shows the activation of that group. So, to perform an activity where many muscles fibres are recruited, it is necessary to use multichannel sEMG. Some examples of this technology in paediatric rehabilitation robots are the lower limb exoskeleton HAL [129] and the device for upper elbow rehabilitation of the San Juan National University [130].
The electroencephalogram (EEG) signal is recorded using many small surface electrodes, often configured in a bathing like cap placed over the scalp that detects the underlying electrical signals. The main advantage of the EEG signal is that the physical disability level does not limit it. Even if the patient has lost all their ability to move the limb required for a task, the brain activity thought to be related to the intent to activate the muscles can be recorded. There are two main disadvantages to this system. Firstly, it is unsuitable for children with brain damage as they cannot generate standard brain patterns for limb activation. Secondly, the EEG signal has greater variability within it than the EMG signal, and it is also easily affected by changes in the patient’s mood and attention. Examples of the EEG signal use are the CP walker that used this signal as a part of its HCI to help children with a physical disability move their legs [120] and the Exohand-2 that used the EEG signal to interact with the exoskeleton [131].
Treated conditions
The majority of studies and devices were for children with neurological conditions (np = 183, 89%), CP being the most studied condition (np = 129, 63%). In contrast, other neurological disorders included ABI and strokes. Significantly few researchers investigated other conditions such as neuromuscular diseases (np = 15, 8%) and traumatic injuries to limbs and the spine (np = 6, 3%). The results obtained from the studies that perform clinical trials or a feasibility study suggests that robotic rehabilitation could benefit children with physical disabilities.
Neurological disorders
Concerning CP, there was evidence of improvement in physical disability using assisted rehabilitation robots. The benefits include an increase in muscle activity [120, 132], endurance for physical activities [133, 134], improvements of balance [114], walking speed [134, 135], the strength of the muscles [136, 137], ROM of the joints [84, 138], upper limb kinematics [139], and manual dexterity [33, 140].
For paediatric ABI, there were reports in the improvement of the walking ability [141], improvement of the lower limb motor performance [94], increase in the ROM of the wrist joint and force increase in the hand [142], improvement in motor function, and gait pattern [143, 144].
In children who suffer a stroke, three studies used rehabilitation robots while performing physical therapy. Marini et al. [119] demonstrated an improvement in wrist motion after the robotic therapy, and Bützer et al. [26] showed the possibility of using a wearable hand exoskeleton to assist children during task-oriented training could be helpful for rehabilitation therapies or assist children during ADLs.
Neuromuscular diseases
The neuromuscular disease presented a different scenario than neurological disorder due to the degeneration of their muscles as the disease progresses, making hard the use of rehabilitation robot due to stiffness in the robot’s joints, which can harm children’s weak muscles. Hence they require compliant actuation [145, 146]. Jansen et al. [145] found that robotic rehabilitation therapy on upper and lower limbs help prevent functional deterioration in children with DMD. Meanwhile, Ganguly et al. [147], Garcia et al. [148] and Sanz-Merodio et al. [146] showed an improvement in walking ability in children with SMA with the assistance of ATLAS, and the exoskeleton was designed to provide Robotic-assisted gait training for children with SMA. Moreover, Koo et al. [149] reported improved arm mobility in children with DMD while using a robotic arm device.
Traumatic injuries
Even if traumatic injuries are common in the paediatric population, robot rehabilitation has not been applied widely in injuries that differ from those at the head. Only scarce information was found related to these conditions. A study of hands robotic rehabilitation was found, highlighting the possibility of using robotic devices to treat burns [150]. Additionally, a study observed a significant improvement in the arm movement and elbowed angle after physical therapy using an upper-limb exoskeleton for 3 months in children that suffer a car accident [130]. Finally, another case reported improving walking ability after robotic-assisted gait training in a girl with SCI [151].
Discussion
It is possible to see that various novel rehabilitation robots have become available to rehabilitation professionals and clients in recent years. And this trend will continue as is possible to incorporate them in activity programs aimed at improving independent function [34,35,36,37] where they offer advantages over the traditional rehabilitation therapies, as they reduced the required effort of therapists during the exercises of the therapies, allowed massed practice in children with substantial limitations and provide information of the patient. Furthermore, they have the potential to be used as assistive devices to aid functional performance for users when they are worn. These possibilities will lead to a new variety of ways for assessment and intervention impacting users’ abilities, task demands, or the environment to promote functional performance and participation.
The findings of this review indicate that the design and development of robotic technologies for the physical rehabilitation of children is in a preliminary stage of development, as many of the devices were designed for adult patients. However, there is a trend toward creating robots specifically for children [17, 26, 57, 148]. Yet less has been done to prove the benefits and constraints of such a system.
Traditionally, rehabilitation robot designers have focused solely on improving physical function [58], which can lead to rejection of the devices as not all the needs of children with disabilities are considered. Thus, to ensure successful adoption of the technology, the rehabilitation robots should cover these needs of the children. Hence, stakeholders’ cooperation is essential through their integration within the design and production process by providing feedback. Designers can use this feedback to validate that the robot meets the stakeholder’s needs. However, the fulfilment of these needs has strong relationships to the chosen technology, mainly the type of robot, the actuator, the training strategy and the HCI. Thus, it is essential to know the advantages and disadvantages of the technology.
Type of robot
When it comes to the type of robot, we can see a trend to migrate from end-effector to exoskeletons. However, most of the devices that had performed clinical trials were end-effector robots designed for adults. This relation could be because the end-effector robot works on the distal part of the limb, guiding the children limb through a movement [152]. This property is helpful in the case of operability as it does not require adaptation to match the children limb’s size, making it easy to be used by a diverse group of children. Furthermore, the bulky frames over the patient limbs are avoided, helping to reduce the weight that the children need to handle. These advantages come with the problem of the systems requiring bulky and heavy external structures, reducing the device’s portability, constraining its use to medical facilities or specific spaces inside a building. Thus, limiting the amount of therapy that the children can have [153]. Additionally, the activity is restricted to a workspace constraining the number of possible movements [40], which could reduce motivation.
On the other hand, exoskeletons work in parallel to the patient limb to perform the activity. Hence, they can be portable devices with the possibility to provide assistive help during activities of ADLs and robotic-assisted rehabilitation therapy in a single device [26]. This advantage will help to provide free movement to enhance the subject’s motivation and autonomously practise their movement training for longer periods [17, 154]. Furthermore, as technology advance, this freedom in mobility will help to increase the participation of children with physical disabilities in different social activities [155]. However, as the technology moves from clinical facilities to open spaces and robots interact more closely with the children, designers will face notable challenges (e.g. the irregularities of the surfaces on which one walks and how the robot reacts to perturbations outdoors environment). Consequently, the requirements of weight, comfort, safety, portability and social acceptability for the exoskeletons will be harder to achieve.
Actuators
The paediatric robotic rehabilitation technology is moving from end-effectors to exoskeletons due to their versatility to be used as a rehabilitation tool or an assistive device [26]. Consequently, actuation technology starts to be a critical part of the design as it negatively influences the weight and the size of the robot.
For the end-effectors robots, actuators are not as critical as with the exoskeletons because they could be placed in external structures. This advantage makes it possible to use bulky and heavy actuators like electric motors. However, using electric motors is hard to achieve compliance that is an important property to increase safety as it is needed to avoid opposing forces that can injure the children. In end-effector robots, compliance was achieved using sensors and a control strategy [146] or using a soft material like the Bowden cables [103].
On the other hand, for exoskeletons, the robot design requirements are hard to enhance with the currently used technology. The actuation system components such as motor and rigid elements are designed for industrial applications not to interact with and to be worn by children. However, they are still the standard as they have the advantages of efficiency, are easy to control, and are readably available in the market. Therefore, the choice of the actuation system is crucial to improve the weight, portability and safety of the exoskeleton.
The first exoskeletons relied on electric motors with rigid transmissions, making them bulky and heavy, reducing their compliance as they generate high resistive torque from the metallic links of the exoskeleton. Therefore, making it difficult to move and less safe can cause non-desirable inertial movements [156, 157]. Furthermore, they require external structures to manage the weight of the exoskeleton.
As the rehabilitation robots move from rehabilitation therapies inside a medical facility to assist the children during ADLs, new actuation technology is needed. This challenge led to using SEA actuators and cable transmission since they have the advantage of been intrinsically complaints as they incorporate soft materials, making the device safer.
Using Bowden cables in the transmissions brings other advantages like simple architecture, low weight on the limb’s distal part, and easy to reconfigure. This last advantage is significant in paediatric rehabilitation as it allows to change the motor easily depending on the abilities and size of the children [26, 73], even though they present some disadvantages because they become unidirectional and difficult to model and control. Instead, in the case of SEAs, which still require rigid links, they were highlighted on the use for children with neuromuscular diseases, as some children are not only weak on the affected joint but the entire body. Thus the exoskeleton must hold the children, but at the same time being compliant to avoid inertial forces that can harm the weak muscles of the children [146].
Another type of actuator used on the robots was the pneumatic. Their attributes of low weight and easy-to-manufacture actuators of different shapes and sizes [158, 159] make them a desirable technology in this field. They are easy to adapt to children with various conditions. However, their main constraint is that they are typically connected to external mechanisms like compressors and pumps cumbersome and noisy. Thus, reducing their portability and appealing making them impractical to use outside clinical facilities.
In Table 8, the advantages and disadvantages of the current actuator technology are presented. It is possible to notice that there is no perfect actuator technology, so more research in this area is needed. Moreover, in the future will be interesting to see devices that use different soft actuators technologies that are inherent compliant and lightweight, such as the already mention SEAs, pneumatic, and Bowden cables. But also new technologies that are under research to be used on rehabilitation robots, like shape memory alloys [160], dielectric elastomer [161], or twisted and coiled polymers actuators [162], as they will reduce the overall weight and increase the compliance. Furthermore, this new technology can be manufactured in different sizes and shapes [163] that could be easily adapted to robots for children of varying height and ability conditions.
Training strategy
In the case of the training strategy, there is no best strategy, but it rather depends on many factors like the abilities and disease that the children have. For example, passive training is suitable for patients with limited mobility; however, when the children are able to generate movements, it tends to decrease children’s participation during the exercise, thus reducing the efficiency of the training [164]. That is why most of the research on the training strategy is centred on assistive training, where the children’s participation is needed. This engagement with the therapy increases the motivation of the children to perform the activities, enhancing the benefits from the therapy [165]. Another advantage of assistive training is that it is used together with video games to increase children’s motivation and social interaction [166]. In addition, this strategy is required for assistive devices. It needs to provide the required intensity to generate the movement safely, efficiently, and reliably, depending on the applied force by the user [167]. However, there is no clear which is the best strategy to provide assistive movement, where some examples of different assistive strategies are guidance force, path control, and locomotion strategy [57, 154, 165, 166].
Alternatively, some researchers suggest that resistive training could be more beneficial for rehabilitation therapy than an assistive force, as it increases the engagement of the children, which can help drive motor learning [120, 168]. Hence, further research is required on the optimal training strategy to increase the benefits from the rehabilitation therapies.
Human–computer interface
The HCIs are essential in developing robotic rehabilitation robots, as they are the medium for the interaction between the children and the robot, impacting the functioning of the actuators and training strategies directly. Thus, HICs are a crucial factor for safety and motivation needs, as it is how the children “communicate” their intention to the robot. Consequently, If the HCI is complex to use, it could lead to the rejection of the device [52]. Furthermore, for safety reasons, the HCI must detect the trigger signal properly and discern between intended movements and involuntary movements, as it can generate undesirable responses [41, 169]. For instance, in the case of CP patients presenting increased muscle tone, rapidly occurring muscle spasms, and severe jerks, which can be considered as a deviation of pattern, causing the robot to apply undesired forces to correct for it or turn off the device suddenly [170].
Consequently, selecting the best HCI for every case needs to be evaluated depending on the capabilities of the children. For example, it could be challenging for patients with advanced muscular dystrophy to use EMG and admittance/impedance interfaces as their muscles progressively deteriorate, turning unable to activate the muscles to generate a movement or a detectable signal [149, 171]. On the other hand, EEG could lead to a better motor function recovery for children with CP as it integrates the central nervous system into rehabilitation therapy [154]. However, this technology could be hard to implement in patients with a cognitive deficit, requiring concentration [131, 172]. For HCIs, it would be interesting to see more devices using physiological signals as they can also evaluate the efficiency of the therapy [154], novel approaches of body-powered control to address children with limited mobility of limbs [173], and devices that integrate different HCI strategies to make the system more robust and adaptable [71, 167, 174].
Treated condition
To better understand how the technology can positively impact children’s lives, it is essential to analyse how the rehabilitation robot’s technology has addressed the different paediatric conditions that can generate physical disability. Because, even if they share in common the deterioration of the musculoskeletal system, each one of the conditions presents certain specific characteristics that need to be considered.
Most of the research has focused on children with neurological conditions, particularly children with CP. However, it seems likely that many of the designed robots that currently work with neurological conditions could also be utilised in traumatic injury scenarios, especially because they have been designed for rehabilitation therapies that can improve common problems across both neurological and traumatic injuries like ROM deficits and a lack of ability to generate muscle force [80, 150]. Contrarily, neuromuscular diseases present a different scenario than neurological disorders and traumatic injuries as the diseases are progressive, making it hard to obtain a permanent improvement on the children skills. Thus, the designs have been focused on design devices capable of assisting with exercise and helping with the ADLs to maintain specific abilities (e.g. walking) for a longer period of time [122, 155].
Unfortunately, the outcomes proving the efficiency of rehabilitation robot in children is still scarce, as the pieces of evidence are low and weak. Hence, the information coming from these studies should be asses carefully, as there are very few randomised controlled trials, with small sample sizes and variability in children’s ability, outcomes measures, treatment protocols, and used devices [31, 65]. Thus, to better understand if the designed robots fulfil the paediatric needs properly by improving their quality of life and physical ability, more studies and robots designed especially for them are needed. Furthermore, more studies with children presenting different conditions from neurological ones are needed, as it can be noticed that the treated condition impacts the requirements design of the rehabilitation robot.
Limitations
It was apparent that some studies were conducted with participants from a wide range of ages; therefore, it was difficult to target all the articles that include paediatric participants. Another problem was the upper bound on the paediatric population’s age as some papers with the term young adults included paediatric participants.
Conclusion
While robotic rehabilitation is gaining momentum with increasing numbers of devices being produced for adults, there is a lack of well-designed and effective products available for children. Early examples of robots have often been created by scaling downsize to meet the smaller stature of children. Few robots have been specifically designed and produced, with children being the focus of the project/program. It is apparent that children have special needs, and these need to be incorporated into designs early in the development program. And even if the fulfilment of these needs is closely related to the chosen structural and technological components like the actuator, training strategy and HCI, they go beyond them. Consideration must also be given to the aesthetics that appeal to children and the need for the robot’s structure to be as unobtrusive as possible. Without such needs being met, no matter how effective the robot works from an engineering perspective, it will not be utilised well by the child.
It is apparent that there is still a lack of understanding of what the most effective therapy is to improve function and quality of life in specific paediatric conditions (e.g. CP or Stroke). Nevertheless, common impairments (e.g. ROM, strength) must be addressed across numerous clinical conditions if patients improve function in everyday tasks. Hence, there is much opportunity for robots to play a role in assisting paediatric rehabilitation. A much more difficult goal to achieve is the development of robots to assist children. At the same time, they do function-related tasks like walking, sitting, lying, and assisting when the child moves from one posture to another. This demand increased complexity throughout the various engineering systems of the robot. After that, a further challenge lies in the robot being able to assist indoors within a relatively safe environment and outdoors where the “lay of the land” is notably different and less predictable. Hence, exploring new technologies to actuate the system and detect children’s intentions when they want to move is necessary.
Availability of data and materials
Not applicable.
Abbreviations
- WHO:
-
World Health Organization
- FDA:
-
US Food and Drug Administration
- CP:
-
Cerebral palsy
- ABI:
-
Acquired brain injury
- DMD:
-
Duchenne muscular dystrophy
- SMA:
-
Spinal muscular atrophy
- SCI:
-
Spinal cord injury
- np:
-
Number of papers
- ROM:
-
Range of motion
- ADL:
-
Activities of daily life
- HCI:
-
Human–computer interface
- EMG:
-
Electromyography
- EEG:
-
Electroencephalogram
- LRF:
-
Laser range finder
- DOF:
-
Degree of freedom
- AC:
-
Alternate current
- DC:
-
Direct current
- SEA:
-
Serial elastic actuator
References
Hall ML, Lobo MA. Design and development of the first exoskeletal garment to enhance arm mobility for children with movement impairments. Assist Technol. 2018;30(5):251–8.
Graham HK, Rosenbaum P, Paneth N, Dan B, Lin JP, Damiano DL, et al. Cerebral palsy. Nat Rev Dis Primers. 2016;2:15082.
Tsze DS, Valente JH. Pediatric stroke: a review. Emerg Med Int. 2011;2011: 734506.
Beretta E, Cesareo A, Biffi E, Schafer C, Galbiati S, Strazzer S. Rehabilitation of upper limb in children with acquired brain injury: a preliminary comparative study. J Healthc Eng. 2018;2018: 4208492.
Ryder S, Leadley RM, Armstrong N, Westwood M, de Kock S, Butt T, et al. The burden, epidemiology, costs and treatment for Duchenne muscular dystrophy: an evidence review. Orphanet J Rare Dis. 2017;12(1):79.
Robinson MT, Estupinan D. Neuromuscular diseases. In: Creutzfeldt CJ, Kluger BM, Holloway RG, editors. Neuropalliative care. Cham: Springer; 2019. p. 101–15.
Thurman DJ. The epidemiology of traumatic brain injury in children and youths: a review of research since 1990. J Child Neurol. 2016;31(1):20–7.
Umraw N, Chan Y, Gomez M, Cartotto RC, Fish JS. Effective hand function assessment after burn injuries. J Burn Care Res. 2004;25(1):134–9; discussion 28.
Case LE, Apkon SD, Eagle M, Gulyas A, Juel L, Matthews D, et al. Rehabilitation management of the patient with Duchenne muscular dystrophy. Pediatrics. 2018;142(Supplement 2):S17–33.
Falzarano V, Marini F, Morasso P, Zenzeri J. Devices and protocols for upper limb robot-assisted rehabilitation of children with neuromotor disorders. Appl Sci. 2019;9(13):2689.
Beretta E, Storm FA, Strazzer S, Frascarelli F, Petrarca M, Colazza A, et al. Effect of robot-assisted gait training in a large population of children with motor impairment due to cerebral palsy or acquired brain injury. Arch Phys Med Rehabil. 2020;101(1):106–12.
Roberts G, Howard K, Spittle AJ, Brown NC, Anderson PJ, Doyle LW. Rates of early intervention services in very preterm children with developmental disabilities at age 2 years. J Paediatr Child Health. 2008;44(5):276–80.
MEDICINE COPE. Management of pediatric trauma. Pediatrics. 2016;138(2):e20161569.
McDonald CM, Mercuri E. Evidence-based care in Duchenne muscular dystrophy. Lancet Neurol. 2018;17(5):389–91.
Lerner ZF, Harvey TA, Lawson JL. A battery-powered ankle exoskeleton improves gait mechanics in a feasibility study of individuals with cerebral palsy. Ann Biomed Eng. 2019;47(6):1345–56.
Abresch RT, Han JJ, Carter GT. Rehabilitation management of neuromuscular disease: the role of exercise training. J Clin Neuromuscul Dis. 2009;11(1):7–21.
Patane F, Rossi S, Del Sette F, Taborri J, Cappa P. WAKE-Up exoskeleton to assist children with cerebral palsy: design and preliminary evaluation in level walking. IEEE Trans Neural Syst Rehabil Eng. 2017;25(7):906–16.
Shi B, Chen X, Yue Z, Yin S, Weng Q, Zhang X, et al. Wearable ankle robots in post-stroke rehabilitation of gait: a systematic review. Front Neurorobot. 2019;13:63.
Low K, editor. Robot-assisted gait rehabilitation: from exoskeletons to gait systems. 2011 Defense Science Research Conference and Expo (DSR); 2011: IEEE.
Shishehgar M, Kerr D, Blake J. A systematic review of research into how robotic technology can help older people. Smart Health. 2018;7:1–18.
Khan A, Anwar Y, editors. Robots in healthcare: a survey. Science and information conference. Springer; 2019.
Martinez-Martin E, Costa A, Cazorla M. PHAROS 2.0—A PHysical assistant RObot system improved. Sensors. 2019;19(20):4531.
Lippross S, Jünemann K-P, Osmonov D, Peh S, Alkatout I, Finn J, et al. Robot assisted spinal surgery—a technical report on the use of DaVinci in orthopaedics. J Orthop. 2020;19:50–3.
Ona ED, Cano-de la Cuerda R, Sanchez-Herrera P, Balaguer C, Jardon A. A review of robotics in neurorehabilitation: towards an automated process for upper limb. J Healthc Eng. 2018;2018:9758939.
SPARC ER. Robotics 2020 Multi-Annual Roadmap for Robotics in Europe, Call 2 ICT24–Horizon 2020. Initial Release B. 2015;15(01):2014.
Bützer T, Dittli J, Lieber J, van Hedel HJ, Meyer-Heim A, Lambercy O, et al., editors. PEXO—a pediatric whole hand exoskeleton for grasping assistance in task-oriented training. 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR); 2019: IEEE.
Shahid T, Gouwanda D, Nurzaman SG, Gopalai AA. Moving toward soft robotics: a decade review of the design of hand exoskeletons. Biomimetics. 2018. https://doi.org/10.3390/biomimetics3030017.
Maciejasz P, Eschweiler J, Gerlach-Hahn K, Jansen-Troy A, Leonhardt S. A survey on robotic devices for upper limb rehabilitation. J Neuroeng Rehabil. 2014;11(1):3.
del Carmen S-V, Gonzalez-Vargas J, Torricelli D, Moreno JC, Pons JL. Compliant lower limb exoskeletons: a comprehensive review on mechanical design principles. J Neuroeng Rehabil. 2019;16(1):55.
Narayan J, Kalita B, Dwivedy SK. Development of robot-based upper limb devices for rehabilitation purposes: a systematic review. Augment Hum Res. 2021;6(1):1–33.
Carvalho I, Pinto SM, das Virgens Chagas D, dos Santos JLP, de Sousa Oliveira T, Batista LA. Robotic gait training for individuals with cerebral palsy: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2017;98(11):2332–44.
Cook A, Encarnação P, Adams K. Robots: assistive technologies for play, learning and cognitive development. Technol Disabil. 2010;22(3):127–45.
Kuo F, Lee H, Hsiao H, Lin J. Robotic-assisted hand therapy for improvement of hand function in children with cerebral palsy: a case series study. Eur J Phys Rehabil Med. 2020. https://doi.org/10.23736/S1973-9087.20.05926-2.
Zhang X, Yue Z, Wang J. Robotics in lower-limb rehabilitation after stroke. Behav Neurol. 2017;2017:3731802.
Fasoli SE, Ladenheim B, Mast J, Krebs HI. New horizons for robot-assisted therapy in pediatrics. Am J Phys Med Rehabil. 2012;91(11 Suppl 3):S280–9.
Hawe RL, Kuczynski AM, Kirton A, Dukelow SP. Assessment of bilateral motor skills and visuospatial attention in children with perinatal stroke using a robotic object hitting task. J Neuroeng Rehabil. 2020;17(1):1–12.
Mehrholz J, Thomas S, Werner C, Kugler J, Pohl M, Elsner B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst Rev. 2017;5: CD006185.
Martelli F, Rossi S, Frascarelli F, Germanotta M, Petrarca M, Castelli E, et al., editors. Estimation of multivariable dynamic ankle impedance after botulinum toxin injection in children with cerebral palsy. 2016 IEEE international symposium on medical measurements and applications (MeMeA); 2016: IEEE.
Alvarez-Perez MG, Garcia-Murillo MA, Cervantes-Sanchez JJ. Robot-assisted ankle rehabilitation: a review. Disabil Rehabil Assist Technol. 2019. https://doi.org/10.1080/17483107.2019.1578424.
McDaid AJ. Design, analysis, and multicriteria optimization of an overground pediatric robotic gait trainer. IEEE/ASME Trans Mechatron. 2017;22(4):1674–84.
He Y, Eguren D, Luu TP, Contreras-Vidal JL. Risk management and regulations for lower limb medical exoskeletons: a review. Med Devices Evid Res. 2017;10:89–107.
Chu CY, Patterson RM. Soft robotic devices for hand rehabilitation and assistance: a narrative review. J Neuroeng Rehabil. 2018;15(1):9.
Veale AJ, Xie SQ. Towards compliant and wearable robotic orthoses: a review of current and emerging actuator technologies. Med Eng Phys. 2016;38(4):317–25.
Kapsalyamov A, Hussain S, Jamwal PK. State-of-the-art assistive powered upper limb exoskeletons for elderly. IEEE Access. 2020;8:178991–9001.
Yan T, Cempini M, Oddo CM, Vitiello N. Review of assistive strategies in powered lower-limb orthoses and exoskeletons. Robot Auton Syst. 2015;64:120–36.
Maalej B, Medhaffar H, Chemori A, Derbel N, editors. A fuzzy sliding mode controller for reducing torques applied to a rehabilitation robot. 2020 17th International multi-conference on systems, signals & devices (SSD); 2020: IEEE.
Jribi R, Maalej B, Derbel N. Exoskeletons control via computed torque for lower limb rehabilitation. New trends in robot control. Springer; 2020. p. 131–51.
Chen J, Damiano DL, Lerner ZF, Bulea TC, editors. Validating model-based prediction of biological knee moment during walking with an exoskeleton in crouch gait: potential application for exoskeleton control. 2019 IEEE 16th international conference on rehabilitation robotics (ICORR); 2019: IEEE.
Narayan J, Dwivedy SK. Towards neuro-fuzzy compensated pid control of lower extremity exoskeleton system for passive gait rehabilitation. IETE J Res. 2020:1–18.
Zeng X, Zhu G, Zhang M, Xie SQ. Reviewing clinical effectiveness of active training strategies of platform-based ankle rehabilitation robots. J Healthc Eng. 2018;2018:2858294.
Plaza A, Hernandez M, Puyuelo G, Garces E, Garcia E. Lower-limb medical and rehabilitation exoskeletons: a review of the current designs. IEEE Rev Biomed Eng. 2021. https://doi.org/10.1109/RBME.2021.3078001.
Fosch-Villaronga E, Čartolovni A, Pierce RL. Promoting inclusiveness in exoskeleton robotics: addressing challenges for pediatric access. Paladyn, J Behav Robot. 2020;11(1):327–39.
Onis MD, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. 2007;85:660–7.
Keller U, Klamroth V, van Hedel HJ, Riener R, editors. ChARMin: a robot for pediatric arm rehabilitation. 2013 IEEE International conference on robotics and automation; 2013: IEEE.
Ganley KJ, Powers CM. Gait kinematics and kinetics of 7-year-old children: a comparison to adults using age-specific anthropometric data. Gait Posture. 2005;21(2):141–5.
Borenstein J, Wagner AR, Howard A. Overtrust of pediatric health-care robots: a preliminary survey of parent perspectives. IEEE Robot Autom Mag. 2018;25(1):46–54.
Keller U, van Hedel HJA, Klamroth-Marganska V, Riener R. ChARMin: the first actuated exoskeleton robot for pediatric arm rehabilitation. IEEE/ASME Trans Mechatron. 2016;21(5):2201–13.
Lobo MA, Hall ML, Greenspan B, Rohloff P, Prosser LA, Smith BA. Wearables for pediatric rehabilitation: how to optimally design and use products to meet the needs of users. Phys Ther. 2019;99(6):647–57.
Wessels R, Dijcks B, Soede M, Gelderblom G, De Witte L. Non-use of provided assistive technology devices, a literature overview. Technol Disabil. 2003;15(4):231–8.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1–34.
Meyer-Heim A, van Hedel HJ, editors. Robot-assisted and computer-enhanced therapies for children with cerebral palsy: current state and clinical implementation. Semin Pediatr Neurol; 2013. https://doi.org/10.1016/j.spen.2013.06.006.
Bayon C, Raya R. Robotic therapies for children with cerebral palsy: a systematic review. Transl Biomed. 2016. https://doi.org/10.21767/2172-0479.100044.
Vova JA, Eggebrecht EM. Utilizing functional electrical stimulation and exoskeletons in pediatrics: a closer look at their roles in gait and functional changes in cerebral palsy. Curr Phys Med Rehabil Rep. 2019;7(2):57–66.
Zwicker JG, Mayson TA. Effectiveness of treadmill training in children with motor impairments: an overview of systematic reviews. Pediatr Phys Ther. 2010;22(4):361–77.
Chen Y-P, Howard AM. Effects of robotic therapy on upper-extremity function in children with cerebral palsy: a systematic review. Dev Neurorehabil. 2016;19(1):64–71.
Mahamud F, Anuar A, editors. Usage of robotic rehabilitation technology for lower limbs therapy of children with cerebral palsy-a review. 2014 IEEE international symposium on robotics and manufacturing automation (ROMA); 2014: IEEE.
Donenberg JG, Fetters L, Johnson R. The effects of locomotor training in children with spinal cord injury: a systematic review. Dev Neurorehabil. 2019;22(4):272–87.
Andrew I, Batavia J, Guy SH. Toward the development of consumer-based criteria for the evaluation of assistive devices. J Rehabil Res Dev. 1990;27(4):425.
Weightman APH, Preston N, Holt R, Allsop M, Levesley M, Bhakta B. Engaging children in healthcare technology design: developing rehabilitation technology for children with cerebral palsy. J Eng Des. 2009;21(5):579–600.
Organization WH. International classification of functioning, disability, and health: children & youth version: ICF-CY: World Health Organization; 2007.
Eguren D, Cestari M, Luu TP, Kilicarslan A, Steele A, Contreras-Vidal JL, editors. Design of a customizable, modular pediatric exoskeleton for rehabilitation and mobility. 2019 IEEE international conference on systems, man and cybernetics (SMC); 2019: IEEE.
Rossi S, Colazza A, Petrarca M, Castelli E, Cappa P, Krebs HI. Feasibility study of a wearable exoskeleton for children: is the gait altered by adding masses on lower limbs? PLoS ONE. 2013. https://doi.org/10.1371/journal.pone.0073139.
Lerner ZF, Gasparri GM, Bair MO, Lawson JL, Luque J, Harvey TA, et al. An untethered ankle exoskeleton improves walking economy in a pilot study of individuals with cerebral palsy. IEEE Trans Neural Syst Rehabil Eng. 2018;26(10):1985–93.
Yamada T, Kadone H, Shimizu Y, Suzuki K, editors. An exoskeleton brake unit for children with crouch gait supporting the knee joint during stance. 2018 International symposium on micro-nanomechatronics and human science (MHS); 2018: IEEE.
Michmizos KP, Krebs HI. Pediatric robotic rehabilitation: Current knowledge and future trends in treating children with sensorimotor impairments. NeuroRehabilitation. 2017;41(1):69–76.
Hall ML, Orzada BT. Expressive prostheses: meaning and significance. Fash Pract. 2013;5(1):9–32.
Schuler T, Brütsch K, Müller R, van Hedel HJ, Meyer-Heim A. Virtual realities as motivational tools for robotic assisted gait training in children: a surface electromyography study. NeuroRehabilitation. 2011;28(4):401–11.
Bulea TC, Lerner ZF, Gravunder AJ, Damiano DL, editors. Exergaming with a pediatric exoskeleton: facilitating rehabilitation and research in children with cerebral palsy. 2017 International Conference on Rehabilitation Robotics (ICORR); 2017: IEEE.
Frascarelli F, Masia L, Di Rosa G, Petrarca M, Cappa P, Castelli E. Robot-mediated and clinical scales evaluation after upper limb botulinum toxin type A injection in children with hemiplegia. J Rehabil Med. 2009;41(12):988–94.
Marini F, Squeri V, Morasso P, Campus C, Konczak J, Masia L. Robot-aided developmental assessment of wrist proprioception in children. J Neuroeng Rehabil. 2017;14(1):3.
Dehem S, Gilliaux M, Lejeune T, Detrembleur C, Galinski D, Sapin J, et al. Assessment of upper limb spasticity in stroke patients using the robotic device REAplan. J Rehabil Med. 2017;49(7):565–71.
Kuczynski AM, Kirton A, Semrau JA, Dukelow SP. Bilateral reaching deficits after unilateral perinatal ischemic stroke: a population-based case-control study. J Neuroeng Rehabil. 2018;15(1):77.
Varalta V, Picelli A, Fonte C, Montemezzi G, La Marchina E, Smania N. Effects of contralesional robot-assisted hand training in patients with unilateral spatial neglect following stroke: a case series study. J Neuroeng Rehabil. 2014;11(1):160.
Shimizu Y, Kadone H, Kubota S, Ueno T, Sankai Y, Hada Y, et al. Voluntary elbow extension-flexion using single joint hybrid assistive limb (HAL) for patients of spastic cerebral palsy: two cases report. Front Neurol. 2019;10:2.
Thielbar KO, Lord TJ, Fischer HC, Lazzaro EC, Barth KC, Stoykov ME, et al. Training finger individuation with a mechatronic-virtual reality system leads to improved fine motor control post-stroke. J Neuroeng Rehabil. 2014;11(1):171.
Tornberg AB, Lauruschkus K. Non-ambulatory children with cerebral palsy: effects of four months of static and dynamic standing exercise on passive range of motion and spasticity in the hip. PeerJ. 2020;8: e8561.
Volpini M, Bartenbach V, Pinotti M, Riener R. Clinical evaluation of a low-cost robot for use in physiotherapy and gait training. J Rehabil Assist Technol Eng. 2017;4: 2055668316688410.
Wu M, Kim J, Arora P, Gaebler-Spira DJ, Zhang Y. Kinematic and EMG responses to pelvis and leg assistance force during treadmill walking in children with cerebral palsy. Neural Plast. 2016;2016:5020348.
Chrif F, Nef T, Lungarella M, Dravid R, Hunt KJ. Control design for a lower-limb paediatric therapy device using linear motor technology. Biomed Signal Process Control. 2017;38:119–27.
Ricklin S, Meyer-Heim A, van Hedel HJA. Dual-task training of children with neuromotor disorders during robot-assisted gait therapy: prerequisites of patients and influence on leg muscle activity. J Neuroeng Rehabil. 2018;15(1):82.
Nakagawa S, Mutsuzaki H, Mataki Y, Endo Y, Matsuda M, Yoshikawa K, et al. Newly developed hybrid assistive limb for pediatric patients with cerebral palsy: a case report. J Phys Ther Sci. 2019;31(8):702–7.
Aycardi LF, Cifuentes CA, Munera M, Bayon C, Ramirez O, Lerma S, et al. Evaluation of biomechanical gait parameters of patients with cerebral palsy at three different levels of gait assistance using the CPWalker. J Neuroeng Rehabil. 2019;16(1):15.
Germanotta M, Taborri J, Rossi S, Frascarelli F, Palermo E, Cappa P, et al. Spasticity measurement based on tonic stretch reflex threshold in children with cerebral palsy using the PediAnklebot. Front Hum Neurosci. 2017;11:277.
Chen K, Xiong B, Ren Y, Dvorkin AY, Gaebler-Spira D, Sisung CE, et al. Ankle passive and active movement training in children with acute brain injury using a wearable robot. J Rehabil Med. 2018;50(1):30–6.
Lerner ZF, Damiano DL, Bulea TC. The effects of exoskeleton assisted knee extension on lower-extremity gait kinematics, kinetics, and muscle activity in children with cerebral palsy. Sci Rep. 2017;7(1):1–12.
Jansen M, de Groot IJ, van Alfen N, Geurts AC. Physical training in boys with Duchenne muscular dystrophy: the protocol of the no use is disuse study. BMC Pediatr. 2010;10(1):55.
Wu M, Landry JM. Toward flexible assistance for locomotor training: design and clinical testing of a cable-driven robot for stroke, spinal cord injury, and cerebral palsy. In: Reinkensmeyer DJ, Dietz V, editors. Neurorehabilitation technology. Cham: Springer; 2016. p. 435–59.
Krebs HI, Michmizos KP, Monterosso L, Mast J, editors. Pediatric anklebot: pilot clinical trial. 2016 6th IEEE international conference on biomedical robotics and biomechatronics (BioRob); 2016: IEEE.
Keller U, Riener R, editors. Design of the pediatric arm rehabilitation robot ChARMin. 5th IEEE RAS/EMBS international conference on biomedical robotics and biomechatronics; 2014: IEEE.
Lerner ZF, Damiano DL, Park HS, Gravunder AJ, Bulea TC. A robotic exoskeleton for treatment of crouch gait in children with cerebral palsy: design and initial application. IEEE Trans Neural Syst Rehabil Eng. 2017;25(6):650–9.
Gasparri GM, Bair MO, Libby RP, Lerner ZF, editors. Verification of a robotic ankle exoskeleton control scheme for gait assistance in individuals with cerebral palsy. 2018 IEEE/RSJ international conference on intelligent robots and systems (IROS); 2018: IEEE.
Kang J, Martelli D, Vashista V, Martinez-Hernandez I, Kim H, Agrawal SK. Robot-driven downward pelvic pull to improve crouch gait in children with cerebral palsy. Sci Robot. 2017;2(8): eaan2634.
Vashista V, Jin X, Agrawal SK, editors. Active tethered pelvic assist device (a-tpad) to study force adaptation in human walking. 2014 IEEE international conference on robotics and automation (ICRA); 2014: IEEE.
Xiong H, Diao X. A review of cable-driven rehabilitation devices. Disabil Rehabil Assist Technol. 2020;15(8):885–97.
Cestari M, Sanz-Merodio D, Garcia E. A new and versatile adjustable rigidity actuator with add-on locking mechanism (ARES-XL). Actuators. 2018;7(1):1.
Sanz-Merodio D, Cestari M, Arevalo JC, Garcia E, editors. A lower-limb exoskeleton for gait assistance in quadriplegia. 2012 IEEE international conference on robotics and biomimetics (ROBIO); 2012.
Borboni A, Mor M, Faglia R. Gloreha—hand robotic rehabilitation: design, mechanical model, and experiments. J Dyn Syst Meas Control. 2016;138(11).
Mirvakili SM, Hunter IW. Artificial muscles: mechanisms, applications, and challenges. Adv. Mater. 2018;30(6):1704407.
Zhang J, Sheng J, ONeill CT, Walsh CJ, Wood RJ, Ryu JH, et al. Robotic artificial muscles: current progress and future perspectives. IEEE transactions on robotics. 2019.
Wirekoh J, Valle L, Pol N, Park YL. Sensorized, flat, pneumatic artificial muscle embedded with biomimetic microfluidic sensors for proprioceptive feedback. Soft Robot. 2019;6(6):768–77.
Ugurlu B, Forni P, Doppmann C, Sariyildiz E, Morimoto J. Stable control of force, position, and stiffness for robot joints powered via pneumatic muscles. IEEE Trans Industr Inf. 2019;15(12):6270–9.
Cioi D, Kale A, Burdea G, Engsberg J, Janes W, Ross S, editors. Ankle control and strength training for children with cerebral palsy using the Rutgers Ankle CP. 2011 IEEE international conference on rehabilitation robotics; 2011: IEEE.
McCall JV, Ludovice MC, Blaylock JA, Kamper DG, editors. A platform for rehabilitation of finger individuation in children with hemiplegic cerebral palsy. 2019 IEEE 16th international conference on rehabilitation robotics (ICORR); 2019: IEEE.
Yazici M, Livanelioglu A, Gucuyener K, Tekin L, Sumer E, Yakut Y. Effects of robotic rehabilitation on walking and balance in pediatric patients with hemiparetic cerebral palsy. Gait Posture. 2019;70:397–402.
Wu YN, Hwang M, Ren Y, Gaebler-Spira D, Zhang LQ. Combined passive stretching and active movement rehabilitation of lower-limb impairments in children with cerebral palsy using a portable robot. Neurorehabil Neural Repair. 2011;25(4):378–85.
Kuczynski AM, Carlson HL, Lebel C, Hodge JA, Dukelow SP, Semrau JA, et al. Sensory tractography and robot-quantified proprioception in hemiparetic children with perinatal stroke. Hum Brain Mapp. 2017;38(5):2424–40.
Cherni Y, Girardin-Vignola G, Ballaz L, Begon M. Reliability of maximum isometric hip and knee torque measurements in children with cerebral palsy using a paediatric exoskeleton–Lokomat. Neurophysiol Clin. 2019;49(4):335–42.
Michmizos KP, Rossi S, Castelli E, Cappa P, Krebs HI. Robot-aided neurorehabilitation: a pediatric robot for ankle rehabilitation. IEEE Trans Neural Syst Rehabil Eng. 2015;23(6):1056–67.
Marini F, Hughes CML, Squeri V, Doglio L, Moretti P, Morasso P, et al. Robotic wrist training after stroke: adaptive modulation of assistance in pediatric rehabilitation. Robot Auton Syst. 2017;91:169–78.
Conner BC, Luque J, Lerner ZF. Adaptive ankle resistance from a wearable robotic device to improve muscle recruitment in cerebral palsy. Ann Biomed Eng. 2020;48(4):1309–21.
Qiu Q, Adamovich S, Saleh S, Lafond I, Merians AS, Fluet GG, editors. A comparison of motor adaptations to robotically facilitated upper extremity task practice demonstrated by children with cerebral palsy and adults with stroke. 2011 IEEE international conference on rehabilitation robotics; 2011: IEEE.
Nizamis K, Stienen AHA, Kamper DG, Keller T, Plettenburg DH, Rouse EJ, et al. Transferrable expertise from bionic arms to robotic exoskeletons: perspectives for stroke and duchenne muscular dystrophy. IEEE Trans Med Robot Bionics. 2019;1(2):88–96.
Chandrasiri M, Ranaweera R, Gopura R, editors. Development of a surface muscle pressure monitoring system for wearable robotic devices. 2019 Moratuwa engineering research conference (MERCon); 2019: IEEE.
Qiu Q, Ramirez DA, Saleh S, Fluet GG, Parikh HD, Kelly D, et al. The New Jersey Institute of Technology Robot-Assisted Virtual Rehabilitation (NJIT-RAVR) system for children with cerebral palsy: a feasibility study. J Neuroeng Rehabil. 2009;6:40.
Zhu TL, Klein J, Dual SA, Leong TC, Burdet E, editors. reachMAN2: a compact rehabilitation robot to train reaching and manipulation. 2014 IEEE/RSJ international conference on intelligent robots and systems; 2014: IEEE.
Krebs HI, Hogan N, Aisen ML, Volpe BT. Robot-aided neurorehabilitation. IEEE Trans Rehabil Eng. 1998;6(1):75–87.
Molteni F, Gasperini G, Gaffuri M, Colombo M, Giovanzana C, Lorenzon C, et al. Wearable robotic exoskeleton for overground gait training in sub-acute and chronic hemiparetic stroke patients: preliminary results. Eur J Phys Rehabil Med. 2017;53(5):676–84.
Taborri J, Rossi S, Palermo E, Cappa P, editors. A HMM distributed classifier to control robotic knee module of an active orthosis. 2015 IEEE international conference on rehabilitation robotics (ICORR); 2015: IEEE.
Suzuki K, Mito G, Kawamoto H, Hasegawa Y, Sankai Y. Intention-based walking support for paraplegia patients with Robot Suit HAL. Adv Robot. 2007;21(12):1441–69.
Lopez NM, de Diego N, Hernandez R, Perez E, Ensinck G, Valentinuzzi ME. Customized device for pediatric upper limb rehabilitation in obstetric brachial palsy. Am J Phys Med Rehabil. 2014;93(3):263–6.
Bobrov P, Biryukova E, Polyaev B, Lajsheva O, Usachjova E, Sokolova A, et al. Rehabilitation of patients with cerebral palsy using hand exoskeleton controlled by brain–computer interface. Bull Russ State Med Univ. 2020. https://doi.org/10.24075/brsmu.2020.047.
Bulea TC, Lerner ZF, Damiano DL, editors. Repeatability of EMG activity during exoskeleton assisted walking in children with cerebral palsy: implications for real time adaptable control. 2018 40th Annual international conference of the IEEE engineering in medicine and biology society (EMBC); 2018: IEEE.
Digiacomo F, Tamburin S, Tebaldi S, Pezzani M, Tagliafierro M, Casale R, et al. Improvement of motor performance in children with cerebral palsy treated with exoskeleton robotic training: a retrospective explorative analysis. Restor Neurol Neurosci. 2019;37(3):239–44.
Wu M, Kim J, Arora P, Gaebler-Spira DJ, Zhang Y. Effects of the integration of dynamic weight shifting training into treadmill training on walking function of children with cerebral palsy: a randomized controlled study. Am J Phys Med Rehabil. 2017;96(11):765–72.
Lee SJ, Jin D, Kang SH, Gaebler-Spira D, Zhang LQ. Combined ankle/knee stretching and pivoting stepping training for children with cerebral palsy. IEEE Trans Neural Syst Rehabil Eng. 2019;27(9):1743–52.
Bayon C, Martin-Lorenzo T, Moral-Saiz B, Ramirez O, Perez-Somarriba A, Lerma-Lara S, et al. A robot-based gait training therapy for pediatric population with cerebral palsy: goal setting, proposal and preliminary clinical implementation. J Neuroeng Rehabil. 2018;15(1):69.
Burdea GC, Cioi D, Kale A, Janes WE, Ross SA, Engsberg JR. Robotics and gaming to improve ankle strength, motor control, and function in children with cerebral palsy—a case study series. IEEE Trans Neural Syst Rehabil Eng. 2013;21(2):165–73.
Druzbicki M, Rusek W, Snela S, Dudek J, Szczepanik M, Zak E, et al. Functional effects of robotic-assisted locomotor treadmill thearapy in children with cerebral palsy. J Rehabil Med. 2013;45(4):358–63.
Gilliaux M, Renders A, Dispa D, Holvoet D, Sapin J, Dehez B, et al. Upper limb robot-assisted therapy in cerebral palsy: a single-blind randomized controlled trial. Neurorehabil Neural Repair. 2015;29(2):183–92.
Fasoli SE, Fragala-Pinkham M, Hughes R, Krebs HI, Hogan N, Stein J. Robotic therapy and botulinum toxin type A: a novel intervention approach for cerebral palsy. Am J Phys Med Rehabil. 2008;87(12):1022–6.
Beretta E, Molteni E, Biffi E, Morganti R, Avantaggiato P, Strazzer S. Robotically-driven orthoses exert proximal-to-distal differential recovery on the lower limbs in children with hemiplegia, early after acquired brain injury. Eur J Paediatr Neurol. 2018;22(4):652–61.
Marini F, Squeri V, Cappello L, Morasso P, Riva A, Doglio L, et al., editors. Adaptive wrist robot training in pediatric rehabilitation. 2015 IEEE international conference on rehabilitation robotics (ICORR); 2015: IEEE.
Molteni E, Beretta E, Altomonte D, Formica F, Strazzer S, editors. Combined robotic-aided gait training and 3D gait analysis provide objective treatment and assessment of gait in children and adolescents with Acquired Hemiplegia. 2015 37th Annual international conference of the IEEE Engineering in Medicine And Biology Society (EMBC); 2015: IEEE.
Beretta E, Romei M, Molteni E, Avantaggiato P, Strazzer S. Combined robotic-aided gait training and physical therapy improve functional abilities and hip kinematics during gait in children and adolescents with acquired brain injury. Brain Inj. 2015;29(7–8):955–62.
Jansen M, van Alfen N, Geurts AC, de Groot IJ. Assisted bicycle training delays functional deterioration in boys with Duchenne muscular dystrophy: the randomized controlled trial “no use is disuse.” Neurorehabil Neural Repair. 2013;27(9):816–27.
Sanz-Merodio D, Puyuelo G, Ganguly A, Garces E, Goñi A, Garcia E. EXOtrainer project clinical evaluation of gait training with exoskeleton in children with spinal muscular atrophy. Advances in robotics research: from lab to market: Springer; 2020. p. 211–27.
Ganguly A, Sanz-Merodio D, Puyuelo G, Goñi A, Garces E, Garcia E, editors. Wearable pediatric gait exoskeleton-a feasibility study. 2018 IEEE/RSJ international conference on intelligent robots and systems (IROS); 2018: IEEE.
Garcia E, Sancho J, Sanz-Merodio D, Prieto M, editors. Atlas 2020: the pediatric gait exoskeleton project. human-centric robotics-proceedings of the 20th international conference clawar 2017; 2017: World Scientific.
Koo B, Montes J, Gamarnik V, Yeager K, Marra J, Dunaway S, et al., editors. Design and evaluation of a hybrid passive and active gravity neutral orthosis (GNO). 2009 Annual international conference of the IEEE engineering in medicine and biology society; 2009: IEEE.
Samhan AF, Abdelhalim NM, Elnaggar RK. Effects of interactive robot-enhanced hand rehabilitation in treatment of paediatric hand-burns: a randomized, controlled trial with 3-months follow-up. Burns. 2020;46(6):1347–55.
Hornby TG, Zemon DH, Campbell D. Robotic-assisted, body-weight–supported treadmill training in individuals following motor incomplete spinal cord injury. Phys Ther. 2005;85(1):52–66.
Chaparro-Rico BD, Cafolla D, Ceccarelli M, Castillo-Castaneda E. NURSE-2 DoF device for arm motion guidance: kinematic, dynamic, and FEM analysis. Appl Sci. 2020;10(6):2139.
Cleary K, Monfaredi R, Salvador T, Talari HF, Coley C, Kovelman S, et al., editors. Pedbothome: robotically-assisted ankle rehabilitation system for children with cerebral palsy. 2019 IEEE 16th international conference on rehabilitation robotics (ICORR); 2019: IEEE.
Bayón C, Ramírez O, Serrano JI, Castillo MDD, Pérez-Somarriba A, Belda-Lois JM, et al. Development and evaluation of a novel robotic platform for gait rehabilitation in patients with cerebral palsy: CPWalker. Robot Auton Syst. 2017;91:101–14.
Kapeller A, Nagenborg MH, Nizamis K. Wearable robotic exoskeletons: a socio-philosophical perspective on Duchenne muscular dystrophy research. Paladyn, J Behav Robot. 2020;11(1):404–13.
Zhu H, Doan J, Stence C, Lv G, Elery T, Gregg R, editors. Design and validation of a torque dense, highly backdrivable powered knee-ankle orthosis. 2017 IEEE international conference on robotics and automation (ICRA); 2017: IEEE.
Krishnan C, Ranganathan R, Dhaher YY, Rymer WZ. A pilot study on the feasibility of robot-aided leg motor training to facilitate active participation. PLoS ONE. 2013;8(10): e77370.
Heung HL, Tang ZQ, Shi XQ, Tong KY, Li Z. Soft rehabilitation actuator with integrated post-stroke finger spasticity evaluation. Front Bioeng Biotechnol. 2020;8:111.
Yang HD, Cooper M, Akbas T, Schumm L, Orzel D, Walsh CJ, editors. A soft inflatable wearable robot for hip abductor assistance: design and preliminary assessment. 2020 8th IEEE RAS/EMBS international conference for biomedical robotics and biomechatronics (BioRob): IEEE.
Copaci D, Martín F, Moreno L, Blanco D. SMA based elbow exoskeleton for rehabilitation therapy and patient evaluation. IEEE Access. 2019;7:31473–84.
Behboodi A, DeSantis C, Lubsen J, Lee S, editors. A mechanized pediatric elbow joint powered by a de-based artificial skeletal muscle. 2020 42nd annual international conference of the IEEE Engineering in Medicine & Biology Society (EMBC); 2020: IEEE.
Saharan L, de Andrade MJ, Saleem W, Baughman RH, Tadesse Y. iGrab: hand orthosis powered by twisted and coiled polymer muscles. Smart Mater Struct. 2017;26(10): 105048.
Chu W-S, Lee K-T, Song S-H, Han M-W, Lee J-Y, Kim H-S, et al. Review of biomimetic underwater robots using smart actuators. Int J Precis Eng Manuf. 2012;13(7):1281–92.
Aurich-Schuler T, Grob F, van Hedel HJA, Labruyere R. Can Lokomat therapy with children and adolescents be improved? An adaptive clinical pilot trial comparing guidance force, path control, and FreeD. J Neuroeng Rehabil. 2017;14(1):76.
Aurich-Schuler T, Labruyère R. An increase in kinematic freedom in the lokomat is related to the ability to elicit a physiological muscle activity pattern: a secondary data analysis investigating differences between guidance force, path control, and FreeD. Front Robot AI. 2019;6:109.
Gallagher J, Preston N, Holt R, Mon-Williams M, Levesley M, Weightman A, editors. Assessment of upper limb movement with an autonomous robotic device in a school environment for children with Cerebral Palsy. 2015 IEEE international conference on rehabilitation robotics (ICORR); 2015: IEEE.
Sanz-Merodio D, Sancho J, Pérez M, García E. Control architecture of the ATLAS 2020 lower-limb active orthosis. In: Advances in cooperative robotics. World Scientific; 2017. p. 860–8.
Wu M, Kim J, Gaebler-Spira DJ, Schmit BD, Arora P. Robotic resistance treadmill training improves locomotor function in children with cerebral palsy: a randomized controlled pilot study. Arch Phys Med Rehabil. 2017;98(11):2126–33.
Elias A, Frizera A, Bastos TF, Valadão C, editors. Robotic walkers from a clinical point of view: feature-based classification and proposal of the UFES Walker. 2012 ISSNIP biosignals and biorobotics conference: biosignals and robotics for better and safer living (BRC); 2012: IEEE.
Aurich-Schuler T, Warken B, Graser JV, Ulrich T, Borggraefe I, Heinen F, et al. Practical recommendations for robot-assisted treadmill therapy (lokomat) in children with cerebral palsy: indications, goal setting, and clinical implementation within the WHO-ICF framework. Neuropediatrics. 2015;46(4):248–60.
Rinaldi M, Petrarca M, Romano A, Vasco G, D’Anna C, Schmid M, et al., editors. EMG-based indicators of muscular co-activation during gait in children with duchenne muscular dystrophy. 2019 41st Annual international conference of the IEEE Engineering in Medicine and Biology Society (EMBC); 2019: IEEE.
Larina N, Nacharova M, Korsunskaya L, Vlasenko S, Pavlenko V. Changes in EEG patterns in the α-frequency band following BCI-based therapy in children with cerebral palsy. Bull Russ State Med Univ. 2020;(4):41–6.
Struijk LNA, Bentsen B, Gaihede M, Lontis ER. Error-free text typing performance of an inductive intra-oral tongue computer interface for severely disabled individuals. IEEE Trans Neural Syst Rehabil Eng. 2017;25(11):2094–104.
Johansen D, Popovic DB, Dosen S, Struijk LNA. Hybrid tongue-myoelectric control improves functional use of a robotic hand prosthesis. IEEE Trans Biomed Eng. 2021;68(6):2011–20.
Aubin PM, Sallum H, Walsh C, Stirling L, Correia A, editors. A pediatric robotic thumb exoskeleton for at-home rehabilitation: the Isolated Orthosis for Thumb Actuation (IOTA). 2013 IEEE 13th International conference on rehabilitation robotics (ICORR); 2013: IEEE.
Laubscher CA, Sawicki JT, editors. Gait guidance control for damping of unnatural motion in a powered pediatric lower-limb orthosis. 2019 IEEE 16th international conference on rehabilitation robotics (ICORR); 2019: IEEE.
Sancho-Perez J, Perez M, Garcia E, Sanz-Merodio D, Plaza A, Cestari M. Mechanical description of ATLAS 2020, A 10-DOF paediatric exoskeleton. Advances in cooperative robotics. World Scientific; 2017. p. 814–22.
Ladenheim B, Altenburger P, Cardinal R, Monterroso L, Dierks T, Mast J, et al. The effect of random or sequential presentation of targets during robot-assisted therapy on children. NeuroRehabilitation. 2013;33(1):25–31.
Masia L, Casadio M, Giannoni P, Sandini G, Morasso P. Performance adaptive training control strategy for recovering wrist movements in stroke patients: a preliminary, feasibility study. J Neuroeng Rehabil. 2009;6:44.
Fluet GG, Qiu Q, Saleh S, Ramirez D, Adamovich S, Kelly D, et al., editors. Robot-assisted virtual rehabilitation (NJIT-RAVR) system for children with upper extremity hemiplegia. 2009 virtual rehabilitation international conference; 2009: IEEE.
Sale P, Lombardi V, Franceschini M. Hand robotics rehabilitation: feasibility and preliminary results of a robotic treatment in patients with hemiparesis. Stroke Res Treat. 2012;2012:820931.
Gilliaux M, Lejeune T, Detrembleur C, Sapin J, Dehez B, Stoquart G. A robotic device as a sensitive quantitative tool to assess upper limb impairments in stroke patients: a preliminary prospective cohort study. J Rehabil Med. 2012;44(3):210–7.
Koenig A, Keller U, Pfluger K, Meyer-Heim A, Riener R, editors. PASCAL: Pediatric arm support robot for combined arm and leg training. 2012 4th IEEE RAS & EMBS international conference on biomedical robotics and biomechatronics (BioRob); 2012: IEEE.
Keller U, Rauter G, Riener R, editors. Assist-as-needed path control for the PASCAL rehabilitation robot. 2013 IEEE 13th international conference on rehabilitation robotics (ICORR); 2013: IEEE.
Tong LZ, Ong HT, Tan JX, Lin J, Burdet E, Ge S, et al., editors. Pediatric rehabilitation with the reachMAN's modular handle. 2015 37th Annual international conference of the IEEE engineering in medicine and biology society (EMBC); 2015: IEEE.
Scott SH. Apparatus for measuring and perturbing shoulder and elbow joint positions and torques during reaching. J Neurosci Methods. 1999;89(2):119–27.
Holley D, Johnson M, Harris G, Beardsley S, editors. A modular low-clearance wrist orthosis for improving wrist motion in children with cerebral palsy. 2014 36th Annual international conference of the IEEE engineering in medicine and biology society; 2014: IEEE.
Hesse S, Uhlenbrock D. A mechanized gait trainer for restoration of gait. J Rehabil Res Dev. 2000;37(6):701–8.
Smania N, Bonetti P, Gandolfi M, Cosentino A, Waldner A, Hesse S, et al. Improved gait after repetitive locomotor training in children with cerebral palsy. Am J Phys Med Rehabil. 2011;90(2):137–49.
Muraki S, Ehara Y, Yamasaki M. Cardiovascular responses at the onset of passive leg cycle exercise in paraplegics with spinal cord injury. Eur J Appl Physiol. 2000;81(4):271–4.
Damiano DL, Stanley CJ, Ohlrich L, Alter KE. Task-specific and functional effects of speed-focused elliptical or motor-assisted cycle training in children with bilateral cerebral palsy: randomized clinical trial. Neurorehabil Neural Repair. 2017;31(8):736–45.
Zhang LQ, Chung SG, Bai Z, Xu D, van Rey EM, Rogers MW, et al. Intelligent stretching of ankle joints with contracture/spasticity. IEEE Trans Neural Syst Rehabil Eng. 2002;10(3):149–57.
Chen K, Wu YN, Ren Y, Liu L, Gaebler-Spira D, Tankard K, et al. Home-based versus laboratory-based robotic ankle training for children with cerebral palsy: a pilot randomized comparative trial. Arch Phys Med Rehabil. 2016;97(8):1237–43.
Schmidt-Lucke C, Kaferle J, Rydh Berner BM, Ahlborg L, Hansen HM, Skjellvik Tollefsen U, et al. Effect of assisted walking-movement in patients with genetic and acquired neuromuscular disorders with the motorised Innowalk device: an international case study meta-analysis. PeerJ. 2019;7: e7098.
Wang F-C, Yu C-H, Chou T-Y. Design and implementation of robust controllers for a gait trainer. Proc Inst Mech Eng [H]. 2009;223(6):687–96.
Wu M, Hornby TG, Landry JM, Roth H, Schmit BD. A cable-driven locomotor training system for restoration of gait in human SCI. Gait Posture. 2011;33(2):256–60.
Nelson CA, Burnfield JM, Shu Y, Buster TW, Taylor AP, Graham A. Modified elliptical machine motor-drive design for assistive gait rehabilitation. J Med Devices. 2011. https://doi.org/10.1115/1.4003693.
Burnfield JM, Buster TW, Pfeifer CM, Irons SL, Cesar GM, Nelson CA. Adapted motor-assisted elliptical for rehabilitation of children with physical disabilities. J Med Devices. 2019; https://doi.org/10.1115/1.4041588.
Girone M, Burdea G, Bouzit M, editors. The Rutgers ankle orthopedic rehabilitation interface. Proceedings of the ASME haptics symposium; 1999: DSC.
Ren Y, Lee SJ, Park HS, Zhang LQ. A pivoting elliptical training system for improving pivoting neuromuscular control and rehabilitating musculoskeletal injuries. IEEE Trans Neural Syst Rehabil Eng. 2013;21(5):860–8.
Monfaredi R, Evans S, Coley C, Silverman A, Jain A, Wilson E, et al., editors. Robotically assisted ankle rehabilitation for pediatrics. 2016 6th IEEE international conference on biomedical robotics and biomechatronics (BioRob); 2016: IEEE.
Park EJ, Kang J, Su H, Stegall P, Miranda DL, Hsu W-H, et al., editors. Design and preliminary evaluation of a multi-robotic system with pelvic and hip assistance for pediatric gait rehabilitation. 2017 International conference on rehabilitation robotics (ICORR); 2017: IEEE.
B. Maalej, R. Jribi, N. Ayadi, F. Abdelhedi, N. Derbel. On a robotic application for rehabilitation systems dedicated to kids affected by cerebral palsy. 2018 15th International multi-conference on systems, signals & devices (SSD). 2018:414–9.
Meyer-Heim A, Borggraefe I, Ammann-Reiffer C, Berweck S, Sennhauser F, Colombo G, et al. Feasibility of robotic-assisted locomotor training in children with central gait impairment. Dev Med Child Neurol. 2007;49(12):900–6.
Kawasaki S, Ohata K, Yoshida T, Yokoyama A, Yamada S. Gait improvements by assisting hip movements with the robot in children with cerebral palsy: a pilot randomized controlled trial. J Neuroeng Rehabil. 2020;17(1):1–8.
Tanaka N, Matsushita S, Sonoda Y, Maruta Y, Fujitaka Y, Sato M, et al. Effect of stride management assist gait training for poststroke hemiplegia: a single center, open-label, randomized controlled trial. J Stroke Cerebrovasc Dis. 2019;28(2):477–86.
Smania N, Gandolfi M, Marconi V, Calanca A, Geroin C, Piazza S, et al. Applicability of a new robotic walking aid in a patient with cerebral palsy. Eur J Phys Rehabil Med. 2011;147(2):135–40.
Karunakaran KK, Ehrenberg N, Cheng J, Nolan KJ, editors. Effects of robotic exoskeleton gait training on an adolescent with brain injury. 2019 41st Annual international conference of the IEEE engineering in medicine and biology society (EMBC); 2019: IEEE.
Lee DR, Shin YK, Park J-H, You JH. Concurrent validity and test-retest reliability of the walkbot-K system for robotic gait training. J Mech Med Biol. 2016;16(08):1640029.
Jin LH, Yang S-S, Choi JY, Sohn MK. The effect of robot-assisted gait training on locomotor function and functional capability for daily activities in children with cerebral palsy: a single-blinded, randomized cross-over trial. Brain Sci. 2020;10(11):801.
Erbil D, Tugba G, Murat TH, Melike A, Merve A, Cagla K, et al. Effects of robot-assisted gait training in chronic stroke patients treated by botulinum toxin-a: a pivotal study. Physiotherapy Res Int. 2018;23(3): e1718.
Sucuoglu H. Effects of robot-assisted gait training alongside conventional therapy on the development of walking in children with cerebral palsy. J Pediatr Rehabil Med. 2020;13(2):127–35.
Mileti I, Taborri J, Rossi S, Petrarca M, Patanè F, Cappa P, editors. Evaluation of the effects on stride-to-stride variability and gait asymmetry in children with cerebral palsy wearing the WAKE-up ankle module. 2016 IEEE International symposium on medical measurements and applications (MeMeA); 2016: IEEE.
Cornejo JL, Santana JF, Salinas SA, editors. Exoskeleton for gait rehabilitation of children: conceptual design. 2017 International conference on rehabilitation robotics (ICORR); 2017: IEEE.
Ren Y, Wu YN, Yang CY, Xu T, Harvey RL, Zhang LQ. Developing a wearable ankle rehabilitation robotic device for in-bed acute stroke rehabilitation. IEEE Trans Neural Syst Rehabil Eng. 2017;25(6):589–96.
Sanz-Merodio D, Perez M, Prieto M, Sancho J, Garcia E, editors. Result of clinical trials with children with spinal muscular atrophy using the atlas 2020 Lower-limb active orthosis2017: World Scientific; 2017.
Medina-De-La-Cruz M, Mujaico-Mariano A, Tirado-Mendoza G, editors. Implementation of a mechanical-electronic system for children from 7 to 11 years old with Duchenne muscular dystrophy. 2018 IEEE XXV international conference on electronics, electrical engineering and computing (INTERCON); 2018: IEEE.
Adib MAHM, Han SY, Ramani PR, You LJ, Yan LM, Sahat IM, et al., editors. Restoration of kids leg function using exoskeleton robotic leg (ExRoLEG) device. Proceedings of the 10th national technical seminar on underwater system technology 2018; 2019: Springer.
Laubscher CA, Farris RJ, Sawicki JT, editors. Design and preliminary evaluation of a powered pediatric lower limb orthosis. ASME 2017 international design engineering technical conferences and computers and information in engineering conference; 2017: American Society of Mechanical Engineers Digital Collection.
Andrade RM, Sapienza S, Bonato P, editors. Development of a “transparent operation mode” for a lower-limb exoskeleton designed for children with cerebral palsy. 2019 IEEE 16th international conference on rehabilitation robotics (ICORR); 2019: IEEE.
Pérez-San Lázaro R, Salgado I, Chairez I. Adaptive sliding-mode controller of a lower limb mobile exoskeleton for active rehabilitation. ISA Trans. 2020. https://doi.org/10.1016/j.isatra.2020.10.008.
Acknowledgements
Not applicable
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
AG reviewed the literature, wrote the manuscript, and prepared the illustrations. LG, JK, PM contributed to the basic concept of the paper and critically revised the draft paper. All authors read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gonzalez, A., Garcia, L., Kilby, J. et al. Robotic devices for paediatric rehabilitation: a review of design features. BioMed Eng OnLine 20, 89 (2021). https://doi.org/10.1186/s12938-021-00920-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12938-021-00920-5