
Abstract
Background
Obesity plays an important role in the pathogenesis of hypertension. Renal dopamine D1-like receptor-mediated diuresis and natriuresis are impaired in the obese Zucker rat, an obesity-related hypertensive rat model. The role of arterial D1 receptors in the hypertension of obese Zucker rats is not clear.
Methods
Plasma glucose and insulin concentrations and blood pressure were measured. The vasodilatory response of isolated mesenteric arteries was evaluated using a small vessel myograph. The expression and phosphorylation of D1 receptors were quantified by co-immunoprecipitation and immunoblotting To determine the effect of hyperinsulinemia and hyperglycemia on the function of the arterial D1 receptor, we studied obese Zucker rats (six to eight-weeks old) fed (6 weeks) vehicle or rosiglitazone, an insulin sensitizer (10 mg/kg per day) and lean Zucker rats (eight to ten-weeks old), fed high-fat diet to induce hyperinsulinemia or injected intraperitoneally with streptomycin (STZ) to induce hyperglycemia.
Results
In obese Zucker rats, the vasorelaxant effect of D1-like receptors was impaired that could be ascribed to decreased arterial D1 receptor expression and increased D1 receptor phosphorylation. In these obese rats, rosiglitazone normalized the arterial D1 receptor expression and phosphorylation and improved the D1-like receptor-mediated vasorelaxation. We also found that D1 receptor-dependent vasorelaxation was decreased in lean Zucker rats with hyperinsulinemia or hyperglycemia but the D1 receptor dysfunction was greater in the former than in the latter group. The ability of insulin and glucose to decrease D1 receptor expression and increase its phosphorylation were confirmed in studies of rat aortic smooth muscle cells.
Conclusions
Both hyperinsulinemia and hyperglycemia caused D1 receptor dysfunction by decreasing arterial D1 receptor expression and increasing D1 receptor phosphorylation. Impaired D1 receptor-mediated vasorelaxation is involved in the pathogenesis of obesity-related hypertension.
Similar content being viewed by others


Background
There is an increasing incidence of metabolic syndrome (MS) which is characterized by abdominal obesity, hypertriglyceridemia, low serum high density lipoprotein cholesterol, elevated blood pressure, and elevated fasting plasma glucose[1]. The metabolic syndrome can cause or intensify cardiovascular, as well as renal disease[1, 2]. One of the possible etiologies of the metabolic syndrome is insulin resistance associated with hyperinsulinemia[1–4]. The stimulatory effect of insulin on sympathetic drive[5], vascular smooth muscle growth[6] and sodium and water retention[7] and its inhibitory effect on prostacyclin synthesis[8] have been suggested to be involved in the pathogenesis of obesity-related hypertension.
Dopamine, a well recognized neurotransmitter in the central nervous system, is also an important modulator of renal and adrenal function, sodium balance, and blood pressure. Dopamine receptors are classified into two subfamilies: the D1-like receptor subfamily includes the D1 and the D5 receptors, while the D2, D3 and D4 receptors belong to the D2-like receptor subfamily. Dysfunction of the renal dopaminergic system is implicated in the pathogenesis and/or maintenance of hypertension[9, 10].
The obese Zucker rat is a model of metabolic syndrome characterized by hyperinsulinemia, hyperglycemia, and hypertension. Dopamine has been implicated in the development of obesity, caused, in part, by increased food intake due to decreased dopaminergic function, specifically the D2 receptor, in the central nervous system[11, 12]. D1 receptor mediated-natriuresis and diuresis are also impaired in obese Zucker rats[13, 14]. Although the kidney is important in the long-term regulation of blood pressure[15], hypertension is also accompanied by increased vascular resistance[16]. Dopamine receptors are expressed in resistance vessels. In the rat mesenteric artery, D1 and D5 receptors are expressed in the tunica media while D2-like receptors are expressed mainly at the adventitia-tunica media transitional zone. The increase in blood pressure with aging has been related to a decrease in the expression of arterial D1, D2, and D5 receptor[17]. However, the role of the arterial D1 receptor in the hypertension of obese Zucker rats is not clear. Our current study tested the hypothesis that the vasorelaxant effect of the D1 receptor is impaired in obese Zucker rats.
Methods
Animal experiments
Male obese Zucker rats and age-matched male lean Zucker rats were housed in plastic cages and fed normal rodent chow and tap water. Twelve obese Zucker rats (six to eight-weeks old) were randomly divided into two groups: 1) one group consisted of obese rats treated (6 weeks) with oral rosiglitazone maleate (10 mg/kg, suspended in 1% carboxy methyl cellulose in distilled water); and 2) the other group consisted of obese control rats treated with the vehicle (1% carboxy methyl cellulose). Eighteen lean Zucker rats (eight to ten-weeks old) were randomly divided into three groups: 1) control rats fed normal diet and treated with vehicle; 2) rats fed control diet and treated with STZ (single intraperitoneal injection, 65 mg/kg); and 3) rats fed high-fat diet (with 50% fat-derived calories) for one month.
All experiments were approved by the Daping Hospital Animal Use and Care Committee and all procedures were approved by the Experimental Animals Committee of Daping Hospital.
Blood pressure and plasma glucose and insulin measurements
After an overnight fast, obese and lean Zucker rats were anesthetized with pentobarbital (Nembutal) with an initial dose of 60 mg/kg, followed by constant infusion at 40 mg/kg/hr[18]. Following a tracheotomy, the left carotid artery was catheterized with polyethylene-50 tubing for blood pressure monitoring. Blood pressure and heart rate were allowed to stabilize for 10 minutes[19] before accepting the blood pressure and heart rate observed as baseline. The abdomen was opened to expose the abdominal aorta and blood samples were collected from the aorta in EDTA-coated tubes for measurement of plasma glucose and insulin, and then the rats were sacrificed by an overdose of pentobarbital (100 mg/kg body wt). Plasma glucose concentrations were determined by using Accu-Chek Advantage glucose monitoring system. Plasma insulin levels were measured by a rat insulin 96-well plate assay (Millipore Co., St Charles, MO).
Preparation and study of small resistance arteries
Each rat was anesthetized with sodium pentobarbital (60 mg/kg). The entire mesenteric bed was removed carefully and placed in ice-cold physiological salt solution (PSS) containing (mM):NaCl 119, KCl 4.7, CaCl2·H2O 2.5, MgSO4·H2O 1.17, NaH2CO3 25, KH2PO4 1.18, EDTA 0.027, and glucose 5.5, adjusted to pH 7.4. The mesenteric artery was carefully and quickly dissected from the surrounding fat and connective tissues. Third-order branches of the superior mesenteric artery (resting arterial diameter: 200 ± 20 μm) were cut into rings approximately 2 mm in length, and mounted on 40 μm stainless-steel wires in an isometric Mulvany-Halpern small-vessel myograph (model 91 M610, J.P. Trading, Science Park, Aarhus, Denmark)[20]. One wire was attached to a force transducer and the other to a micrometer so that wall tension can be measured at a predetermined internal diameter. The rings were maintained in PSS at 37°C and continuously bubbled with oxygen (95%) and carbon dioxide (5%) (Carbogen)[21]. The dissecting procedures were performed with extreme care to protect the endothelium from inadvertent damage, proved by a normal response to acetylcholine (Ach) (10-5 Ach-induced relaxation >80% of basal values of arteries preconstricted with phenylephrine HCl [PHE, 10-5M]). In some vessels, the endothelium was removed by pulling a hair along the inside of the vessel; successful denudation of the endothelium was confirmed by the absence of relaxation with Ach (10-5M)[22]. Following mounting, the arterial ring was equilibrated in PSS for 1 hr at 37°C at a wall tension of 0.1 mN/mm. Based on preliminary data from >100 vessels, we confirmed that a normalized circumference (L0) = 0.9 L100 resulted in maximal active force development. The vessels were studied at L0 in all subsequent protocols. After determining the response to Ach, as indicated above, the vessels were rinsed three times with fresh PSS and allowed to recover to baseline for 15 minutes. In the first set of experiments, the rings were contracted with phenylephrine HCl (10-5M) and high-potassium PSS (KPSS, 125 mM) to obtain the maximal response. After obtaining the maximal response to PHE (10-5M), the response curves to fenoldopam, a D1 receptor agonist[9, 10], were measured by a cumulative concentration-dependent protocol (10-9 to 10-5M). Response to every single concentration of fenoldopam was observed for 2 minutes. To test the vasorelaxant specific effects of D1 receptors, the arteries were incubated with the D1-like receptor antagonist SCH23390 (10-7M) for 30 minutes before fenoldopam treatment. In order to determine specificity of the vasodilatory effect of D1 receptor stimulation, we studied the vasodilation induced by sodium nitroprusside (SNP, 10-10 to 10-4M) in PHE-preconstricted mesenteric arteries.
Cell and sample preparation
Embryonic thoracic aortic smooth muscle cells from normotensive Berlin–Druckrey IX rats (A10, ATCC, Hercules, CA) were cultured at 37°C in 95% air/5% CO2 atmosphere in Dulbecco’s Modified Eagle’s Medium. A10 cells (80% confluence) and mesenteric arteries from Zucker rats were flash frozen by liquid nitrogen and homogenized in ice-cold lysis buffer (5 ml/gm tissue) (20 mM Tris-HCl, pH 7.4; 2 mM EDTA, pH 8.0; 2 mM EGTA; 100 mM NaCl; 10 μg/ml leupeptin; 10 μg/ml aprotinin; 2 mM phenylmethylsulfonyl fluoride; 1% NP-40), sonicated, kept on ice for 1 hr, and centrifuged at 16,000 g for 30 minutes. All samples were stored at -70°C until use.
Immunoblotting
After boiling the homogenates in sample buffer (35 mmol/L Tris-HCl, pH 6.8, 4% SDS, 9.3% dithiothreitol, 0.01% bromophenol blue, 30% glycerol) at 95°C for 5 min, 100 μg of protein were separated by SDS-PAGE (10% polyacrylamide), and then electroblotted onto nitrocellulose membranes (Bio-Rad). The blots were blocked overnight with 5% nonfat dry milk in phosphate buffered saline with Tween 20 (PBST) (0.05% Tween 20 in 10 mmol/l phosphate buffered (isotonic) saline) at 4°C with constant shaking, then incubated with polyclonal rabbit anti-rat D1 receptor antibodies (1:400 dilution; Millipore) overnight in the cold-room at 4°C. The membranes were then further incubated with infrared- labeled secondary antibodies (donkey anti-rabbit IRDye 800, Li-Cor Biosciences, Lincoln, NE) added to bind to the primary antibody at room temperature for 1 hr. The membranes were washed three times with PBST. The bound complex was detected using the Odyssey Infrared Imaging System (Li-Cor Biosciences). The images were analyzed using the Odyssey Application Software to obtain the integrated intensities.
Determination of basal D1 receptor phosphorylation by co-immunoprecipitation
Equal amounts of lysates (1.0 mg protein/ml supernatant from A10 cells or mesenteric artery) were incubated with polyclonal antiphosphoserine antibody (HKSP, New Territories, HK) (2.5 μg/ml) for 1 hr and protein-G agarose at 4°C for 12 hr. The immunoprecipitates were pelleted and washed four times with lysis buffer. The pellets were suspended in sample buffer, boiled for 10 min, and subjected to immunoblotting with polyclonal affinity-purified rabbit anti-rat D1 receptor antibody. In order to determine the specificity of the bands, normal rabbit IgG (negative control) and D1 receptor antibody (positive control) were used as the immunoprecipitants[23]. The bound complexes were detected using the Odyssey Infrared Imaging System (Li-Cor Biosciences). The images were analyzed using the Odyssey Application Software to obtain the integrated intensities.
Materials
Fenoldopam, rosiglitazone maleate, STZ, mitogen-activated protein kinase (MAPK) inhibitor PD98059, Ach, SNP, PHE, and D1 receptor antagonist SCH23390 were obtained from Sigma-Aldrich (St. Louis, MO). Rabbit anti-rat D1 receptor polyclonal antibodies and rat insulin 96 well plate assay kit were obtained from Millipore Corporation (St Charles, MO); and anti-phosphoserine antibodies were obtained from Abcam Ltd (New Territories, Hong Kong, China).
Statistical analysis
The data are expressed as mean ± SEM. Comparison within groups was made by repeated measures ANOVA (or paired t- test when only 2 groups were compared), and comparison among groups (or t-test when only 2 groups were compared) was made by factorial ANOVA with Holm-Sidak test. A value of P < 0.05 was considered significant.
Results
D1 receptor-mediated vasorelaxant effect is impaired in mesenteric arteries from obese Zucker rats
Consistent with previous reports[24], several variables, including body weight, and fasting plasma glucose and insulin concentrations and blood pressure, were higher in obese than lean Zucker rats (Table 1). Fenoldopam, the D1 receptor agonist, (10-7M to 10-5M) induced a concentration-dependent vasorelaxation in the third-order mesenteric arteries from lean Zucker rats (Figure 1A). The absence of endothelium did not affect the fenoldopam-induced vasorelaxation, indicating that the fenoldopam-induced vasorelaxation was endothelium-independent (Figure 1B). The vasorelaxant effect of fenoldopam was via a D1-like receptor because a D1-like receptor antagonist, SCH23390 (10-7M), blocked the fenoldopam-induced vasorelaxation (Figure 1C), although SCH23390, by itself, was without any effect. The impaired vasorelaxant effect of fenoldopam was not a generalized phenomenon, because sodium nitroprusside (10-10 to 10-4M)-mediated vasodilation was not impaired in obese Zucker rats, consistent with previous reports[25, 26] (Figure 1D).

Relaxation of phenylephrine (PHE)-preconstricted rat mesenteric arterial rings in response to fenoldopam and sodium nitroprusside (SNP). Rat mesenteric arterial rings from obese and lean Zucker rats with (E+) (A) or without (E-) endothelium (B) were preconstricted with PHE (10-5M) and then treated with varying concentrations of fenoldopam (Fen, 10-9-10-5M) (*P < 0.01 vs. obese rats, n = 8). (C): D1-like receptor specificity of fenoldopam-induced vasorelaxation in rat mesenteric arterial rings. Rat mesenteric arterial rings from lean Zucker rats were preconstricted with PHE, and then incubated with fenoldopam (Fen, 10-6M) and/or SCH23390 (SCH, 10-7M) (*P < 0.01 vs. Fen, n = 6). (D): Rat mesenteric arterial rings from obese and lean Zucker rats with endothelium (E+) were preconstricted with PHE (10-5M) and then treated with varying concentrations of SNP (10-10-10-4M) (P = NS lean vs obese, n = 5).
To determine whether or not the arterial D1 receptor is involved in the pathogenesis of obesity-related hypertension, we studied the D1 receptor function in third-order mesenteric arteries from obese Zucker rats. We found that the fenoldopam-induced vasorelaxation was lost in obese Zucker rats in the presence (Figure 1A) or absence (Figure 1B) of the endothelium. The dysfunction of renal D1 receptor in hypertension[27] and obese Zucker rats[28, 29] has been reported to be caused by basal hyperphosphorylation of the renal D1 receptor. To determine whether or not this phenomenon also exists in third order mesenteric arteries of obese Zucker rats, D1 receptor expression and phosphorylation was studied by immunoblotting and immunoprecipitation. We found that D1 receptor expression was lower (Figure 2A), while basal D1 receptor phosphorylation (Figure 2B) in third order mesenteric arteries was higher in obese than lean Zucker rats.

D 1 receptor expression and phosphorylation in mesenteric arteries from lean and obese Zucker rats. (A): D1 receptor expression was determined by immunoblotting. (B): Serine-phosphorylated D1 receptor in rat mesenteric arteries was determined by co-immunoprecipitation and immunoblotting. Normal rabbit IgG (negative control) or D1 receptor antibody (positive control) was used as the immunoprecipitant. D1 receptor serine phosphorylation was normalized by D1 receptor protein. (*P < 0.05 vs. lean rats, n = 6).
Roles of hyperinsulinemia and hyperglycemia in the D1 receptor vascular dysfunction in obese Zucker rats
The pathogenesis of obesity is complex. To determine whether or not high plasma levels of glucose and insulin are involved in the obesity-related hypertension, the obese Zucker rats were treated with the insulin sensitizer[30], rosiglitazone (10 mg/kg oral, daily). We found that rosiglitazone restored the impaired fenoldopam-mediated vasorelaxation in obese Zucker rats (Figure 3A), increased the decreased D1 receptor expression (Figure 3B), and decreased the increased phosphorylation (Figure 3C) of D1 receptor in mesenteric arteries from obese Zucker rats consistent with those reported in the kidney[28].

Effect of rosiglitazone on D 1 receptor expression and function in mesenteric arteries from obese Zucker rats. The mesenteric arteries from obese Zucker rats, treated with rosiglitazone (ROG) or vehicle, were incubated with varying concentrations of fenoldopam (10-9-10-5M). The vasorelaxation with fenoldopam is shown in 3A (*P < 0.05, vs. obese rats, n = 8 repeated measures ANOVA, Holm-Sidak test) while D1 receptor expression or phosphorylation in mesenteric arteries, determined by immunoblotting or co-immunoprecipitation, is shown in 3B and 3C, respectively. D1 receptor serine phosphorylation was normalized by D1 receptor protein. (*P < 0.05, vs. obese rats, n = 6),
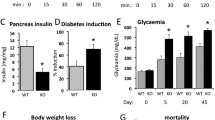
Consistent with other reports[28, 30], our current study found that rosiglitazone reduced plasma insulin and glucose levels and blood pressure (Table 1). Therefore, it was difficult to determine whether hyperinsulinemia, hyperglycemia, or both led to the dysfunction of the arterial D1 receptor. To overcome this dilemma, we used the hyperinsulinemic and hyperglycemic lean Zucker rat models. Lean Zucker rats fattened by a high-fat diet for one month developed hyperinsulinemia but had normal blood pressure, similar to other reports[31, 32]. To establish a hyperglycemia model, lean Zucker rats were intraperitoneally injected with a single dose of STZ (65 mg/kg)[33]; the STZ-treated lean Zucker rats would be expected to develop slightly high blood pressure and hyperglycemia but with low plasma insulin levels (Table 1), as described by others[34]. We found that both hyperinsulinemic (Figure 4A) and hyperglycemic (Figure 4B) lean Zucker rats had impaired D1 receptor-mediated vasorelaxation, accompanied by decreased D1 receptor expression (Figure 4C) and increased D1 receptor phosphorylation (Figure 4D), but the dysfunction of the D1 receptor was greater in the hyperinsulinemia than hyperglycemia model, indicating that insulin plays a more important role than hyperglycemia in the impairment of arterial D1 receptor-mediated relaxation (Figures 4A-D).

D 1 receptor expression and function in lean Zucker rats with hyperinsulinemia or hyperglycemia. Lean Zucker rats were fed high-fat diet (HFD) to induce hyperinsulinemia or intraperitoneally injected with streptomycin (STZ) to induce hyperglycemia. The mesenteric arteries preconstricted with PHE from those rats were treated with varying concentrations of fenoldopam (Fen, 10-9-10-5M) (A and B) (*P < 0.05, vs. lean Zucker rats, n = 8). D1 receptor expression was determined by immunoblotting (C) and D1 receptor phosphorylation (D) was determined by co-immunoprecipitation and immunobloting. D1 receptor serine phosphorylation was normalized by D1 receptor protein (*P < 0.05, vs. obese rats, n = 6).
Effect of insulin and glucose on D1 receptor expression and phosphorylation in A10 cells
To further confirm the in vivo results, the effects of high insulin and high glucose concentrations on D1 receptor expression and phosphorylation were studied in A10 cells, a rat thoracic aorta-derived smooth muscle cell line. Treatment with insulin (Figures 5A and5B) or high glucose (Figures 5C and5D) decreased D1 receptor expression and increased D1 receptor phosphorylation. In the presence of a MAP kinase inhibitor, PD98059 (10-6 M), the effects of insulin on D1 receptor expression and phosphorylation were blocked, indicating that MAP kinase is involved in the signaling pathway (Figures 6A and6B).

Effect of insulin and glucose on D 1 receptor expression and phosphorylation in A10 cells. A10 cells were treated with varying concentrations of insulin (A and B) or glucose (C and D) for 24 hrs. D1 receptor expression was determined by immunoblotting. A10 cells were treated with insulin (10-7M) and glucose (35 mM) for 24 hrs. D1 receptor expression and phosphorylation were determined by co-immunoprecipitation or immunoblotting. D1 receptor serine phosphorylation was normalized by D1 receptor protein (*P < 0.05, vs. control, n = 5).

Role of MAP kinase in the regulation by insulin of D 1 receptor expression and phosphorylation in A10 cells. A10 cells were treated with insulin (10-7M) in the presence or absence of the MAP kinase inhibitor PD98059 (10-6M) for 24 hrs. D1 receptor expression (A) or phosphorylation (B) was determined by immunoblotting or co-immunoprecipitation. D1 receptor serine phosphorylation was normalized by D1 receptor protein. (*P < 0.01, vs. control; #P < 0.05, vs. insulin, n = 5).
Discussion
Role of hyperinsulinemia in obesity-related hypertension
Obesity is a well-known risk factor for hypertension[15, 35]. Indeed, risk estimates according to the Framingham study show that roughly 80% of essential hypertension in men and 65% in women can be directly attributed to obesity[36]. It is accepted that insulin resistance is epidemiologically linked with hypertension[37, 38]. The compensatory hyperinsulinemia that occurs with insulin resistance increases renal sodium reabsorption and sympathetic activity and leads to elevated arterial pressure[39]. Insulin resistance and compensatory hyperinsulinemia impair the production of nitric oxide and favor the production of vasoconstrictors[40–42]. Our current study found hyperinsulinemia, hyperglycemia, and elevated blood pressure in obese Zucker rats that were reduced by rosiglitazone treatment similar to previous reports[43, 44]. We also found that lean Zucker rats fed a high fat diet had hyperinsulinemia and STZ-treated lean Zucker rats were hyperglycemic and hypoinsulinemic, similar to other reports[31, 45].
Impairment of D1 receptor-mediated vasodilation is involved in obesity-related hypertension
Dopamine has been reported as an important modulator of sodium balance, renal and adrenal function, and blood pressure and is relevant to the pathogenesis and/or maintenance of hypertension. In humans with essential hypertension and rodents with genetic hypertension (SHRs and Dahl salt-sensitive rats), D1-like receptor agonist-mediated natriuretic and diuretic responses are impaired[46, 47]. The ability of D1-like receptors to stimulate adenylyl cyclase activity in renal arteries is also impaired in SHRs[48] and we have also reported an impaired ability of D1 receptors to dilate the mesenteric arteries of SHRs[49]. Other studies have shown that the D1 receptor is hyperphosphorylated and uncoupled from G protein subunits, leading to the D1 receptor dysfunction in SHRs, which precedes the onset of hypertension and co-segregates with the hypertensive phenotype[10, 50]. Thus, D1 receptor dysfunction is a primary defect in the hypertension of SHRs. Lokhandwala et al have found that obese Zucker rats have defective renal D1 receptor function associated with a decrease in D1 receptor expression and ability to inhibit Na, K-ATPase and Na,H-exchanger activities in renal proximal tubules[13, 28, 30]. These authors suggested that the renal dopaminergic dysfunction in obese Zucker rats is acquired and not inherited[14] and could be ameliorated by inhibition of reactive oxygen species production by tempol and insulin sensitization by rosiglitazone[28, 29]. Because increased peripheral vascular resistance and altered vascular reactivity are distinctive features of essential hypertension[16], we tested the hypothesis that the hypertension of obese Zucker rats may be caused by an impairment of D1 receptor-mediated vasodilation. This was indeed the case as the D1 receptor-mediated vasorelaxation was impaired in obese Zucker rats. This dysfunction of the D1 receptor could be ascribed to the decreased D1 receptor expression and increased D1 receptor phosphorylation because the rosiglitazone-mediated amelioration of the impaired D1 receptor relaxant effect was associated with an increase in D1 receptor expression and a decrease in D1 receptor phosphorylation. Rosiglitazone, a PPARγ agonist, has many effects on the cardiovascular system independent of its insulin sensitizing effects, including anti-inflammation and direct stimulation of NO production[51]. Whether or not such mechanisms were involved in the rosiglitazone-mediated improvement of the vasodilatory effect of the D1 receptor in the current report needs to be determined in a future study.
Role of hyperinsulinemia or hyperglycemia in the dysfunction of arterial D1 receptor in obese Zucker rats
Obese Zucker rats have increased plasma insulin and fasting glucose levels[24, 52, 53]. As stated above, treatment of obese Zucker rats with rosiglitazone reduced plasma insulin and glucose levels and improved the vasorelaxant effect of fenoldopam that was associated with an increase in the vascular expression of D1 receptor and a decrease in vascular serine-phosphorylated D1 receptor. Thus, hyperinsulinemia and hyperglycemia may be involved in the defective fenoldopam-mediated relaxation in small mesenteric arteries isolated from obese Zucker rats. In order to identify the mechanisms that caused the impaired D1 receptor vasodilatory function in obese Zucker rats, we used two rat models: high fat diet-induced hyperinsulinemia and STZ-induced type 1 diabetes in lean Zucker rats. The former rat model is characterized by insulin resistance and hyperinsulinemia[31, 32] while the latter rat model is characterized by hyperglycemia and low plasma insulin levels[33, 34]. After the establishment of hyperinsulinemia or hyperglycemia, mesenteric arteries had an impaired fenoldopam-mediated vasorelaxation that was more evident in the high fat diet-fed hyperinsulinemic rats than STZ-induced type I diabetic rats. Therefore, both hyperinsulinemia and hyperglycemia are involved in the dysfunction of the arterial D1 receptor, but hyperinsulinemia plays a more important role than hyperglycemia in this phenomenon.
The ability of increased insulin and glucose concentrations to decrease D1 receptor expression and increase D1 receptor phosphorylation in vivo was confirmed in vitro in A10 cells. Treatment of A10 cells with insulin decreased D1 receptor expression and increased D1 receptor phosphorylation, consistent with the findings in renal proximal tubule cells[54, 55]. Mitogen-activated protein kinase (MAPK) is activated in cardiovascular diseases such as diabetes and hypertension[56, 57]. The up-regulation of MAPK reduces renal D1 receptor affinity and G-protein coupling in obese rats[58]. The current studies also showed that blockade of MAPK reversed both the decreased D1 receptor expression and increased D1 receptor phosphorylation caused by high insulin in A10 cells.
Limitations
Besides of the role of hyperinsulinemia and hyperglycemia in the D1-receptor mediated arterial dysfunction, adiponectin, as an important adipose tissue-derived factor, might have some effect on dopamine function. For example, monosodium glutamate induces obesity in rodents markedly decreases adiponectin levels[59] and compromises dopaminergic systems[60]. Moreover, dopamine stimulates adiponectin release[61], and antidiabetic treatment in Zucker diabetic fatty rats inhibits the development of hypo-adiponectinemia in mesenteric resistance arteries, but is not able to improve adiponectin induced vasodilation[62]. Whether or not the plasma adiponectin would affect arterial dopamine receptor function needs to be determined in the future study.
Conclusions
In summary, this study shows that both hyperinsulinemia and hyperglycemia impair vascular D1 receptor function that is associated with decreased D1 receptor expression and increased D1 receptor phosphorylation. Besides, hyperinsulinemia plays a more important role than hyperglycemia in the dysfunction of the arterial D1 receptor in obese Zucker rats. Impaired D1 receptor-mediated vasorelaxation is involved in the pathogenesis of obesity-related hypertension.
Abbreviations
- STZ:
-
Streptomycin
- HFD:
-
High-fat diet
- MS:
-
Metabolic syndrome
- PSS:
-
Physiological salt solution
- Ach:
-
Acetylcholine
- PHE:
-
Phenylephrine HCl
- KPSS:
-
High-potassium PSS
- SNP:
-
Sodium nitroprusside
- MAPK:
-
Mitogen-activated protein kinase
- ROG:
-
Rosiglitazone
- Fen:
-
Fenoldopam
- SCH:
-
SCH23390
- E:
-
Endothelium
- M:
-
mol/L
References
Grundy SM, Brewer HB, Cleeman JI, Smith SC, Lenfant C: American Heart Association; National Heart, Lung, and Blood Institute. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation. 2004, 109 (3): 433-438. 10.1161/01.CIR.0000111245.75752.C6.
Singh AK, Kari JA: Metabolic syndrome and chronic kidney disease. Curr Opin Nephrol Hypertens. 2013, 22 (2): 198-203. 10.1097/MNH.0b013e32835dda78.
Vonbank A, Saely CH, Rein P, Drexel H: Insulin resistance is significantly associated with the metabolic syndrome, but not with sonographically proven peripheral arterial disease. Cardiovasc Diabetol. 2013, 12: 106-10.1186/1475-2840-12-106.
Saely CH, Aczel S, Marte T, Langer P, Hoefle G, Drexel H: The metabolic syndrome, insulin resistance, and cardiovascular risk in diabetic and nondiabetic patients. J Clin Endocrinol Metab. 2005, 90 (10): 5698-5703. 10.1210/jc.2005-0799.
Alvarez GE, Beske SD, Ballard TP, Davy KP: Sympathetic neural activation in visceral obesity. Circulation. 2002, 106 (20): 2533-2536. 10.1161/01.CIR.0000041244.79165.25.
Frisbee JC, Hollander JM, Brock RW, Yu HG, Boegehold MA: Integration of skeletal muscle resistance arteriolar reactivity for perfusion responses in the metabolic syndrome. Am J Physiol Regul Integr Comp Physiol. 2009, 296 (6): R1771-R1782. 10.1152/ajpregu.00096.2009.
Ter Maaten JC, Voorburg A, Heine RJ, Ter Wee PM, Donker AJ, Gans RO: Renal handling of urate and sodium during acute physiological hyperinsulinaemia in healthy subjects. Clin Sci (Lond). 1997, 92 (1): 51-58.
Richelsen B, Borglum JD, Sorensen SS: Biosynthetic capacity and regulatory aspects of prostaglandin E2 formation in adipocytes. Mol Cell Endocrinol. 1992, 85 (1–2): 73-81.
Zeng C, Jose PA: Dopamine receptors: important antihypertensive counterbalance against hypertensive factors. Hypertension. 2011, 57 (1): 11-17. 10.1161/HYPERTENSIONAHA.110.157727.
Zeng C, Felder RA, Jose PA: A new approach for treatment of hypertension: modifying D1 dopamine receptor function. Cardiovasc Hematol Agents Med Chem. 2006, 4 (4): 369-377. 10.2174/187152506778520727.
Baladi MG, Daws LC, France CP: You are what you eat: influence of type and amount of food consumed on central dopamine systems and the behavioral effects of direct- and indirect-acting dopamine receptor agonists. Neuropharmacology. 2012, 63 (1): 76-86. 10.1016/j.neuropharm.2012.02.005.
Davis LM, Michaelides M, Cheskin LJ, Moran TH, Aja S, Watkins PA, Pei Z, Contoreggi C, McCullough K, Hope B, Wang GJ, Volkow ND, Thanos PK: Bromocriptine administration reduces hyperphagia and adiposity and differentially affects dopamine D2 receptor and transporter binding in leptin-receptor-deficient Zucker rats and rats with diet-induced obesity. Neuroendocrinology. 2009, 89 (2): 152-162. 10.1159/000170586.
Lokhandwala MF, Hussain T: Defective renal dopamine D1-like receptor signal transduction in obese hypertensive rats. Acta Physiol Scand. 2000, 168 (1): 251-255. 10.1046/j.1365-201x.2000.00667.x.
Banday AA, Hussain T, Lokhandwala MF: Renal dopamine D1 receptor dysfunction is acquired and not inherited in obese Zucker rats. Am J Physiol Renal Physiol. 2004, 287 (1): F109-F116. 10.1152/ajprenal.00396.2003.
Hall JE, Granger JP, do Carmo JM, da Silva AA, Dubinion J, George E, Hamza S, Speed J, Hall ME: Hypertension: physiology and pathophysiology. Compr Physiol. 2012, 2 (4): 2393-2442.
Schiffrin EL, Touyz RM: From bedside to bench to bedside: role of renin-angiotensin-aldosterone system in remodeling of resistance arteries in hypertension. Am J Physiol Heart Circ Physiol. 2004, 287 (2): H435-H446. 10.1152/ajpheart.00262.2004.
Ricci A, Amenta F, Bronzetti E, Felici L, Hussain T, Lokhandwala MF: Age-related changes of dopamine receptor protein immunoreactivity in the rat mesenteric vascular tree. Mech Ageing Dev. 2002, 123 (5): 537-546. 10.1016/S0047-6374(01)00361-X.
Charbit AR, Akerman S, Goadsby PJ: Comparison of the effects of central and peripheral dopamine receptor activation on evoked firing in the trigeminocervical complex. J Pharmacol Exp Ther. 2009, 331 (2): 752-763. 10.1124/jpet.109.151951.
McCoy CE, Douglas FL, Goldberg LI: Selective antagonism of the hypotensive effects of dopamine agonists in spontaneously hypertensive rats. Hypertension. 1986, 8 (4): 298-302. 10.1161/01.HYP.8.4.298.
Mulvany MJ, Halpern W: Contractile properties of small arterial resistance vessels in spontaneously hypertensive and normotensive rats. Circ Res. 1977, 41 (1): 19-26. 10.1161/01.RES.41.1.19.
Lobato NS, Filgueira FP, Prakash R, Giachini FR, Ergul A, Carvalho MH, Webb RC, Tostes RC, Fortes ZB: Reduced endothelium-dependent relaxation to anandamide in mesenteric arteries from young obese Zucker rats. PLoSOne. 2013, 8 (5): e63449-10.1371/journal.pone.0063449.
Wang Y, Han Y, Yang J, Wang Z, Liu L, Wang W: Relaxant effect of all-trans-retinoic acid via NO-sGC-cGMP pathway and calcium-activated potassium channels in rat mesenteric artery. Am J Physiol Heart Circ Physiol. 2013, 304 (1): H51-H57. 10.1152/ajpheart.00240.2012.
Chen Y, Asico LD, Zheng S, Villar VA, He D, Zhou L, Zeng C, Jose PA: Gastrin and D1 dopamine receptor interact to induce natriuresis and diuresis. Hypertension. 2013, 62 (5): 927-933. 10.1161/HYPERTENSIONAHA.113.01094.
Muhammad AB, Lokhandwala MF, Banday AA: Exercise reduces oxidative stress but does not alleviate hyperinsulinemia or renal dopamine D1 receptor dysfunction in obese rats. Am J Physiol Renal Physiol. 2011, 300 (1): F98-F104. 10.1152/ajprenal.00386.2010.
Mingorance C, del Pozo Gonzalez M, Dolores Herrera M, de Sotomayor Alvarez M: Oral supplementation of propionyl-l-carnitine reduces body weight and hyperinsulinaemia in obese Zucker rats. Br J Nutr. 2009, 102 (8): 1145-1153. 10.1017/S0007114509389230.
Zhou W, Wang XL, Kaduce TL, Spector AA, Lee HC: Impaired arachidonic acid-mediated dilation of small mesenteric arteries in Zucker diabetic fatty rats. Am J Physiol Heart Circ Physiol. 2005, 288 (5): H2210-H2218. 10.1152/ajpheart.00704.2004.
Yu P, Asico LD, Luo Y, Andrews P, Eisner GM, Hopfer U: D1 dopamine receptor hyperphosphorylation in renal proximal tubules in hypertension. Kidney Int. 2006, 70 (6): 1072-1079. 10.1038/sj.ki.5001708.
Trivedi M, Lokhandwala MF: Rosiglitazone restores renal D1A receptor-Gs protein coupling by reducing receptor hyperphosphorylation in obese rats. Am J Physiol Renal Physiol. 2005, 289 (2): F298-F304. 10.1152/ajprenal.00362.2004.
Banday AA, Marwaha A, Tallam LS, Lokhandwala MF: Tempol reduces oxidative stress, improves insulin sensitivity, decreases renal dopamine D1 receptor hyperphosphorylation, and restores D1 receptor-G-protein coupling and function in obese Zucker rats. Diabetes. 2005, 54 (7): 2219-2226. 10.2337/diabetes.54.7.2219.
Trivedi M, Marwaha A, Lokhandwala M: Rosiglitazone restores G-protein coupling, recruitment, and function of renal dopamine D1A receptor in obese Zucker rats. Hypertension. 2004, 43 (2): 376-382. 10.1161/01.HYP.0000111587.51185.fe.
Ebenezer PJ, Mariappan N, Elks CM, Haque M, Francis J: Diet-induced renal changes in Zucker rats are ameliorated by the superoxide dismutase mimetic TEMPOL. Obesity (Silver Spring). 2009, 17 (11): 1994-2002. 10.1038/oby.2009.137.
Henriksen EJ, Teachey MK, Lindborg KA, Diehl CJ, Beneze AN: The high-fat-fed lean Zucker rat: a spontaneous isocaloric model of fat-induced insulin resistance associated with muscle GSK-3 overactivity. Am J Physiol Regul Integr Comp Physiol. 2008, 294 (6): R1813-R1821. 10.1152/ajpregu.00178.2008.
Marwaha A, Banday AA, Lokhandwala MF: Reduced renal dopamine D1 receptor function in streptozotocin-induced diabetic rats. Am J Physiol Renal Physiol. 2004, 286 (3): F451-F457. 10.1152/ajprenal.00227.2003.
Varu VN, Ahanchi SS, Hogg ME, Bhikhapurwala HA, Chen A, Popowich DA, Vavra AK, Martinez J, Jiang Q, Saavedra JE, Hrabie JA, Keefer LK, Kibbe MR: Insulin enhances the effect of nitric oxide at inhibiting neointimal hyperplasia in a rat model of type 1 diabetes. Am J Physiol Heart Circ Physiol. 2010, 299 (3): H772-H779. 10.1152/ajpheart.01234.2009.
Landsberg L, Aronne LJ, Beilin LJ, Burke V, Igel LI, Lloyd-Jones D: Obesity-related hypertension: pathogenesis, cardiovascular risk, and treatment: a position paper of The Obesity Society and the American Society of Hypertension. J Clin Hypertens (Greenwich). 2013, 15 (1): 14-33. 10.1111/jch.12049.
Garrison RJ, Kannel WB, Stokes J, Castelli WP: Incidence and precursors of hypertension in young adults: the Framingham Offspring Study. Prev Med. 1987, 16 (2): 235-251. 10.1016/0091-7435(87)90087-9.
Xun P, Wu Y, He Q, He K: Fasting insulin concentrations and incidence of hypertension, stroke, and coronary heart disease: a meta-analysis of prospective cohort studies. Am J Clin Nutr. 2013, 98 (6): 1543-1554. 10.3945/ajcn.113.065565.
Ruderman NB, Carling D, Prentki M, Cacicedo JM: AMPK, insulin resistance, and the metabolic syndrome. J Clin Invest. 2013, 123 (7): 2764-2772. 10.1172/JCI67227.
Tiwari S, Riazi S, Ecelbarger CA: Insulin’s impact on renal sodium transport and blood pressure in health, obesity, and diabetes. Am J Physiol Renal Physiol. 2007, 293 (4): F974-F984. 10.1152/ajprenal.00149.2007.
Wilcox CS: Effects of tempol and redox-cycling nitroxides in models of oxidative stress. Pharmacol Ther. 2010, 126 (2): 119-145. 10.1016/j.pharmthera.2010.01.003.
Kashyap SR, Roman LJ, Lamont J, Masters BS, Bajaj M, Suraamornkul S, Belfort R, Berria R, Kellogg DL, Liu Y, DeFronzo RA: Insulin resistance is associated with impaired nitric oxide synthase activity in skeletal muscle of type 2 diabetic subjects. J Clin Endocrinol Metab. 2005, 90 (2): 1100-1105. 10.1210/jc.2004-0745.
Hsueh WA, Lyon CJ, Quinones MJ: Insulin resistance and the endothelium. Am J Med. 2004, 117 (2): 109-117. 10.1016/j.amjmed.2004.02.042.
de Artiñano Aleixandre A, Miguel Castro M: Experimental rat models to study the metabolic syndrome. Br J Nutr. 2009, 102 (9): 1246-1253. 10.1017/S0007114509990729.
Umrani DN, Banday AA, Hussain T, Lokhandwala MF: Rosiglitazone treatment restores renal dopamine receptor function in obese Zucker rats. Hypertension. 2002, 40 (6): 880-885. 10.1161/01.HYP.0000039963.01288.D3.
Tiwari S, Halagappa VK, Riazi S, Hu X, Ecelbarger CA: Reduced expression of insulin receptors in the kidneys of insulin-resistant rats. J Am Soc Nephrol. 2007, 18 (10): 2661-2671. 10.1681/ASN.2006121410.
Ladines CA, Zeng C, Asico LD, Sun X, Pocchiari F, Semeraro C, Pisegna J, Wank S, Yamaguchi I, Eisner GM, Jose PA: Impaired renal D (1)-like and D (2)-like dopamine receptor interaction in the spontaneously hypertensive rat. Am J Physiol Regul Integr Comp Physiol. 2001, 281 (4): R1071-R1078.
Nishi A, Eklöf AC, Bertorello AM, Aperia A: Dopamine regulation of renal Na+, K(+)-ATPase activity is lacking in Dahl salt-sensitive rats. Hypertension. 1993, 21 (6 Pt 1): 767-771.
De Vries PA, de Zeeuw D, de Jong PE, Navis G: The abnormal renal vasodilator response to D1-like receptor stimulation in conscious SHR can be normalized by AT1 blockade. J Cardiovasc Pharmacol. 2004, 44 (5): 571-576. 10.1097/00005344-200411000-00009.
Zeng C, Wang D, Asico LD, Welch WJ, Wilcox CS, Hopfer U, Eisner GM, Felder RA, Jose PA: Aberrant D1 and D3 dopamine receptor transregulation in hypertension. Hypertension. 2004, 43 (3): 654-660. 10.1161/01.HYP.0000114601.30306.bf.
Albrecht FE, Drago J, Felder RA, Printz MP, Eisner GM, Robillard JE, Sibley DR, Westphal HJ, Jose PA: Role of the D1A dopamine receptor in the pathogenesis of genetic hypertension. J Clin Invest. 1996, 97 (10): 2283-2288. 10.1172/JCI118670.
Balakumar P, Kathuria S: Submaximal PPARγ activation and endothelial dysfunction: new perspectives for the management of cardiovascular disorders. Br J Pharmacol. 2012, 166 (7): 1981-1992. 10.1111/j.1476-5381.2012.01938.x.
Wu SQ, Hopfner RL, McNeill JR, Wilson TW, Gopalakrishnan V: Altered paracrine effect of endothelin in blood vessels of the hyperinsulinemic, insulin resistant obese Zucker rat. Cardiovasc Res. 2000, 45 (4): 994-1000. 10.1016/S0008-6363(99)00417-4.
Walker AB, Chattington PD, Buckingham RE, Williams G: The thiazolidinedione rosiglitazone (BRL-49653) lowers blood pressure and protects against impairment of endothelial function in Zucker fatty rats. Diabetes. 1999, 48 (7): 1448-1453. 10.2337/diabetes.48.7.1448.
Banday AA, Fazili FR, Lokhandwala MF: Insulin causes renal dopamine D1 receptor desensitization via GRK2-mediated receptor phosphorylation involving phosphatidylinositol 3-kinase and protein kinase C. Am J Physiol Renal Physiol. 2007, 293 (3): F877-F884. 10.1152/ajprenal.00184.2007.
Banday AA, Asghar M, Hussain T, Lokhandwala MF: Dopamine-mediated inhibition of renal Na, K-ATPase is reduced by insulin. Hypertension. 2003, 41 (6): 1353-1358. 10.1161/01.HYP.0000069260.11830.CD.
Yoshizumi M, Tsuchiya K, Tamaki T: Signal transduction of reactive oxygen species and mitogen-activated protein kinases in cardiovascular disease. J Med Invest. 2001, 48: 11-24.
Nishiyama A, Yoshizumi M, Hitomi H, Kagami S, Kondo S, Miyatake A, Fukunaga M, Tamaki T, Kiyomoto H, Kohno M, Shokoji T, Kimura S, Abe Y: The SOD mimetic tempol ameliorates glomerular injury and reduces mitogen-activated protein kinase activity in Dahl salt-sensitive rats. J Am Soc Nephrol. 2004, 15: 306-315. 10.1097/01.ASN.0000108523.02100.E0.
Banday AA, Fazili FR, Marwaha A, Lokhandwala MF: Mitogen-activated protein kinase upregulation reduces renal D1 receptor affinity and G-protein coupling in obese rats. Kidney Int. 2007, 71 (5): 397-406. 10.1038/sj.ki.5002055.
Savcheniuk OA, Virchenko OV, Falalyeyeva TM, Beregova TV, Babenko LP, Lazarenko LM, Demchenko OM, Bubnov RV, Spivak MY: The efficacy of probiotics for monosodium glutamate-induced obesity: dietology concerns and opportunities for prevention. EPMA J. 2014, 5 (1): 2-10.1186/1878-5085-5-2.
Leguisamo NM, Lehnen AM, Machado UF, Okamoto MM, Markoski MM, Pinto GH, Schaan BD: GLUT4 content decreases along with insulin resistance and high levels of inflammatory markers in rats with metabolic syndrome. Cardiovasc Diabetol. 2012, 11: 100-10.1186/1475-2840-11-100.
Borcherding DC, Hugo ER, Idelman G, De Silva A, Richtand NW, Loftus J, Ben-Jonathan N: Dopamine receptors in human adipocytes: expression and functions. PLoS One. 2011, 6 (9): e25537-10.1371/journal.pone.0025537.
Schmid PM, Resch M, Schach C, Birner C, Riegger GA, Luchner A, Endemann DH: Antidiabetic treatment restores adiponectin serum levels and APPL1 expression, but does not improve adiponectin-induced vasodilation and endothelial dysfunction in Zucker diabetic fatty rats. Cardiovasc Diabetol. 2013, 12: 46-10.1186/1475-2840-12-46.
Acknowledgments
This research was supported by grants from the National Outstanding Youth Science Foundation (30925018) and National Natural Science Foundation of China (81070559, 81270338).
Author information
Authors and Affiliations
Corresponding authors
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
JJF, YH, HYW performed most of the experiments and analyzed data and wrote the manuscript. ZW performed some experiments and write the cover letter. YKL reviewed and edited the manuscript. XJC and YC performed some experiments and contributed to the discussion. Laureano D. Asico and Pedro A. Jose edited the manuscript and contributed to the discussion. CCZ and LZ designed the experiments and wrote and edited the manuscript. All authors read and approved the final manuscript.
Jinjuan Fu, Yu Han, Hongyong Wang contributed equally to this work.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Fu, J., Han, Y., Wang, H. et al. Impaired dopamine D1 receptor-mediated vasorelaxation of mesenteric arteries in obese Zucker rats. Cardiovasc Diabetol 13, 50 (2014). https://doi.org/10.1186/1475-2840-13-50
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1475-2840-13-50