
Abstract
Background
Non-specific low back pain (NSLBP) is a large and costly problem. It has a lifetime prevalence of 80% and results in high levels of healthcare cost. It is a major cause for long term sickness amongst the workforce and is associated with high levels of fear avoidance and kinesiophobia. Stabilisation (or ‘core stability’) exercises have been suggested to reduce symptoms of pain and disability and form an effective treatment. Despite it being the most commonly used form of physiotherapy treatment within the UK there is a lack of positive evidence to support its use. The aims of this systematic review update is to investigate the effectiveness of stabilisation exercises for the treatment of NSLBP, and compare any effectiveness to other forms of exercise.
Methods
A systematic review published in 2008 was updated with a search of PubMed, CINAHL, AMED, Pedro and The Cochrane Library, October 2006 to October 2013. Two authors independently selected studies, and two authors independently extracted the data. Methodological quality was evaluated using the PEDro scale. Meta-analysis was carried out when appropriate.
Results
29 studies were included: 22 studies (n = 2,258) provided post treatment effect on pain and 24 studies (n = 2,359) provided post treatment effect on disability. Pain and disability scores were transformed to a 0 to 100 scale. Meta-analysis showed significant benefit for stabilisation exercises versus any alternative treatment or control for long term pain and disability with mean difference of -6.39 (95% CI -10.14 to -2.65) and -3.92 (95% CI -7.25 to -0.59) respectively. The difference between groups was clinically insignificant. When compared with alternative forms of exercise, there was no statistical or clinically significant difference. Mean difference for pain was -3.06 (95% CI -6.74 to 0.63) and disability -1.89 (95% CI -5.10 to 1.33).
Conclusion
There is strong evidence stabilisation exercises are not more effective than any other form of active exercise in the long term. The low levels of heterogeneity and large number of high methodological quality of available studies, at long term follow-up, strengthen our current findings, and further research is unlikely to considerably alter this conclusion.
Similar content being viewed by others

Background
Non-specific low back pain (LBP) can be described as low back pain without underlying cause or disease, and has a lifetime prevalence of 80% [1, 2]. Point prevalence ranges from 12% to 33%, with 90% of acute episodes recovering within six weeks [1, 3]. However, 62% of people experiencing their first episode of LBP will develop chronic symptoms lasting longer than one year, with 16% of people still sick listed from work at 6 months [4]. The UK health service spends more than £1 billion on related costs, including hospital and GP appointments and physiotherapy treatments, with similar high costs seen in other developed countries [5, 6]. LBP is a major cause for long term sickness amongst the workforce, and has been estimated to cost UK employers as much as £624 million per year, with 119 million works days lost each year [7, 8].
In the UK patients with LBP are routinely referred to physiotherapy [6]. Treatment can involve a number of different techniques ranging from spinal manipulations, mobilisation, advice, general exercises and specifically tailored exercises [9]. It has been claimed that there is a link between dysfunction within the activation and timing of local spinal stabilisation muscles and back pain [10–12]. Consequently a therapeutic exercise regime aimed at these muscles was developed, designed to ‘retrain’ motor skills and the activation dysfunction [12]. Despite doubts raised about this link between back pain and muscle activation, and the effectiveness of such an exercise regime (known as stabilisation or ‘core stability’ exercises) it has grown in popularity and now ranks the most common form of physiotherapy treatment in the UK for back pain [9, 13–15].
A 2008 systematic review by May and Johnson, which included 18 trials up to 2006, concluded that specific stabilisation exercises may be beneficial over no treatment, but went on to report that it was unlikely to produce an outcome better than any other form of exercise [13]. It has been suggested that median duration of survival time of a systematic review is 5.5 years, with 23% of systematic reviews being out of date within two years of publication [16]. Since 2006 there has been considerable growth in the evidence base, with a large number of new trials being published. In total there have been seven systematic reviews that have looked at stabilisation exercises [13, 17–22], with the previous three performing a meta-analysis [17, 21, 22]. Macedo et al [17] included studies published up to June 2008 and concluded that stabilisation exercises were no better than general exercise. In 2012 Wang et al [21] carried out a systematic review and also concluded there was no significant difference between ‘core stability’ and general exercises [21]. However, Wang et al’s narrow definition of ‘core stability’ exercises was “exercises performed on unstable surfaces”, rather than a broader definition based upon specific muscle activation. Furthermore, they only included randomised controlled trials (RCT) that specifically compared intervention versus general exercise, rather than any other alternative treatment, and only included people suffering back pain for more than three months. Consequently only five articles fulfilled their inclusion criteria [21]. Our systematic review uses a more broader definition and comparison, similar to May and Johnson [13], and found 19 further articles to add to the original 18 [13]. In contract to these results more recently Byström et al [22] reported that stabilisation exercises were more favourable than general exercises. They searched the literature up to October 2011, but did not limit their participants to non specific back pain and had far stricter inclusion criteria. Our review included a further 15 articles to Byström et al thus providing the justification for a more up to date review.
This systemic review and meta-analysis was conducted to update the 2008 data by May and Johnson [13]. The primary aim of this analysis is to systematically review the most current up to date literature to determine whether stabilisation (or ‘core stability’) exercises are an effective therapeutic treatment compared to an alternative treatment for people with non-specific low back pain. The secondary aim is to determine if stabilisation exercises are as effective as other forms of exercise, and to evaluate findings by meta-analysis if appropriate. This systematic review update followed the recommendations of the PRISMA statement [23].
Methods
Search strategy
An electronic database search of title and abstract was conducted October 2006 to October 2013 on the following databases: (1) PubMed, (2) the Cumulative Index to Nursing and Allied Health Literature (CINAHL), (3) The Allied and Complimentary Medicine Database (AMED), (4) Physiotherapy Evidence Database (Pedro), (5) The Cochrane Library. Specific search strategies depended on the particular database being searched. For the keywords and the PubMed search strategy used see Table 1. Hand searches of the reference list of included articles were also performed.
Study selection
For inclusion the studies had to meet the following criteria.
Participants
Adults recruited from the general population with non-specific low back pain of any length of time. Low back pain defined as, but not restrictive to, pain and/or stiffness between the lower rib and buttock crease with or without leg pain. Studies with specific pathology, such as systemic inflammatory diseases, prolapsed disc, spondylolisthesis, pregnancy related, fractures, tumours, infections or osteoporosis were excluded.
Interventions
Primary intervention arm of stabilisation, or ‘core stability’, exercises defined as: facilitation of deep muscles of the spine (primarily transversus abdominis or multifidus) at low level, integrated into exercise, progressing into functional activity, according to Richardson et al [12], Norris et al [24] or O’Sullivan et al [25]. Comparison group of any other intervention, placebo or control were considered appropriate.
Outcomes
Included studies were required to report an outcome measure of pain and/or functional disability.
Study design
Studies had to be full randomised controlled trials (RCTs), published in English, in a peer reviewed journal. Studies that were not randomised or quasi-random were excluded.
Study selection
One reviewer (BS) conducted the electronic database searches and screened the title and abstracts. Full copies of potential eligible paper were retrieved and independently screened by two reviewers (BS and CL). Initial percentage agreement was 68%, and using Cohen’s statistic method kappa agreement was k = 0.29, which is considered poor to fair agreement [26–28]. Disagreements were resolved by consensus without the need for a third reviewer (SM), who was available. Initial disagreements were due to; intervention criteria [29–33], study population [34, 35], study design [36–39] and duplication of results from another publication being missed [40, 41].
Our review excluded participants with specific pathology, so all three reviewers (BS, CL and SM) verified any exclusion of studies from the 2008 review [13].
Data extraction
We extracted the following data from the included articles: study design, participant information, interventions and setting, follow-up period and outcome data [42]. These data were then compiled into a standard table by one reviewer (BS) and then independently checked and verified by a second reviewer (SM). Disagreements were resolved through consensus. A third reviewer (CL) was available in the event of an agreement not being reached, but was not required. Of the included articles three had inconsistencies within their text, figures or tables with regards to their results [33, 43, 44]. All were contacted by e-mail, and all gave clarification. One study published median outcome scores, and the authors were contacted and provided mean outcome data [45]. Effectiveness was judged for short term (≤3 months from randomisation), medium term (>3 and <12 months) and long term (≥12 months), as recommended by the 2009 Updated Method Guidelines for Systematic Reviews in the Cochrane Back Review Group and in keeping with the original 2008 systematic review [13, 46].
Data from the 2008 review was taken directly from the published review [13].
Quality assessment
Studies meeting the inclusion criteria were assessed for methodological quality and risk of bias using the PEDro scale [47]. The 11 item PEDro scale was developed by Verhagen et al using the Delphi consensus technique to develop a list of criteria thought by experts in the field to measure methodological quality [48]. The PEDro scale consists of the following items: (1) Was eligibility criteria specified? (2) Were all subjects randomly allocated? (3) Were allocations concealed? (4) Were the groups similar at baseline? (5) Was there blinding of all subjects? (6) Was there blinding of all therapists? (7) Was there blinding of all assessors? (8) Was there measures of at least one key outcome for more than 85% of the subjects initially allocated to groups? (9) Did all subjects for whom outcome measures were available receive the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analysed by “intention to treat”? (10) Were the results of between group statistical comparisons reported for at least one key outcome? (11) Did the study have both point measures and measures of variability for at least one key outcome? [47]. Items 2 – 9 refer to the internal validity of a paper, and items 10 and 11 refer to the statistical analysis, ensuring sufficient data to enable appropriate interpretation of the results. Item 1 is related to the external validity and therefore not included in the total PEDro score [49].
All included articles were already scored within the PEDro database, and these data were extracted from the PEDro website [50]. Based upon the original 2008 paper and precedent within the literature, studies scoring ≥6 out of 10 were considered to be high quality [13, 51].
Statistical analysis
Pain and disability mean scores, along with their measure of range (standard deviation/95% confidence interval) were transformed to a score ranging from 0 to 100 [52]. All data analyses were performed using the OpenMetaAnalyst software [53]. Statistical between study heterogeneity was assessed with the I 2 statistic, and this review considered 25% low, 50% moderate and 75% high [54]. If trials were considered sufficiently homogenous then outcome data was pooled according to outcome (pain or disability), methodological quality (PEDro scores <6, or ≥6) and follow-up period. Due to the inherent heterogeneity in low back pain within the literature, the DerSimonian and Laird random effects model was used [55].
Sensitivity analysis
The robustness of our results was tested through a sensitivity analysis. We assessed the impact of using solely high quality studies with using studies of low, medium and high quality combined.
Results
Study identification
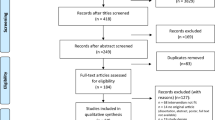
The initial database search produced 2,076 citations, of which 41 were appropriate for full text review, see Figure 1 for study selection process.

Study selection process.
After full text review 23 articles were excluded. Reasons being: participants not meeting criteria [34, 35, 56, 57], intervention not meeting criteria [29, 31, 32, 58–61], study design not meeting criteria [36–39, 62–64], duplications of results from other included studies [40, 41, 65] and no appropriate outcome measures [66]. That left a total 18 studies for inclusion [33, 43–45, 67–80]. Of the 18, two were separate publications of different treatment groups of the same larger study [71, 72]. Of note is that Franca et al [71] did not perform an intention to treat analysis, and so has a lower PEDro score than Franca at al [72]. However, as both had a PEDro score ≥ 6 this does not affect the pooling of both comparisons within the data synthesis. Therefore, a total of 17 separate trials were included.
From the 18 included studies from the 2008 review, seven were rejected for this review, five due to this review only including patients with non specific back pain [25, 81–84], one because it was a pilot study [85] and one due to inappropriate outcomes [86]. That resulted in 12 studies being drawn from the 2008 review (one from two publications) [87–99], with 29 studies in total included for this updated review.
Characteristics of included studies
A summary of the characteristics of the included studies along with the main results is shown in Table 2. There were heterogeneous populations within the studies, with regard to duration of symptoms and presence of leg symptoms. Ten of the studies specified participants having back pain lasting more than three months [43, 67, 69, 71–73, 76–78], with two studies specifying pain lasting three or more months [68, 70], two specifying more than two months [33, 45], one specified any length of time [75], and two studies did not detail their criteria [44, 74]. Four studies included participants with or without leg pain [67–70], eight excluded participants with leg pain [33, 44, 45, 71–73, 77, 78] and six were not clear on their inclusion criteria with regards to leg pain [43, 74–76, 79, 80].
Stabilisation exercises were the sole intervention for the majority of the studies, with five being individually treated [68, 70–72, 75, 79] and nine being in a class setting [33, 44, 45, 64, 73, 76–78, 80]. Three studies combined stabilisation exercises with other forms of treatment, such as general exercises [43, 67], and electrotherapy treatment [74].
Thirteen studies used a visual analogue scale to measure pain [43–45, 67, 70–75, 77, 78, 80], whilst four used an ordinal numerical rating scale [62, 63, 70, 73]. Four studies used the Roland-Morris disability Questionnaire (RMDQ) to measure disability [62, 63, 70, 73], whilst 12 measured disability using the Oswestry Disability Index (ODI) [33, 43–45, 64, 71–74, 77–80]. Two studies also included the Fear-Avoidance Beliefs Questionnaire (FABQ) as an outcome measure [77, 79].
Sixteen studies recorded short term follow-up, with 14 measuring pain and disability [43–45, 68, 70–74, 76–80], one just pain [67] and one just disability [33]. Seven studies recorded medium term follow-up, with six recording outcomes for pain and disability [45, 68–70, 76, 77], and one just pain [75]. Six studies recorded long term follow-up, with five recording pain and disability [45, 68–70, 76], and one just pain [79]. Two further studies went on to record follow-up of disability and pain extra long term [45, 69].
For the characteristics of the 12 included studies from the 2008 review, please refer to the original review [13].
Study quality and bias
The PEDro scores ranged from 4 to 9 [47], with mean score of 6.6 (please refer to the PEDro website for score breakdowns). All participants were randomly allocated and all studies provided adequate results and analysis (items 10 and 11). Only five studies failed to conceal allocation [43, 67, 73, 74, 78] and one study assess baseline comparability [75]. No study blinded therapists, and only three blinded their participants [68, 75, 80]. The lower scoring studies were mainly marked down on blinding of assessors, adequate follow-up, intention to treat analysis and concealed allocation. With all studies, the greatest possible source of bias was related to blinding. Eleven publications scored ≥6 [33, 45, 68–72, 76–80], along with seven from the 2008 review, totalling 18 studies of high quality [88–91, 93, 95, 98].
Data synthesis
Four studies from the 2008 review had insufficient data to enable their inclusion into a meta-analysis [89, 92, 94, 96], one of which was a high quality paper [89]. Twenty-two studies remained, 17 of high quality, which were considered suitably similar to warrant quantitative analysis and synthesis. Too few studies (only two of high quality) provided data ≥18 months to warrant pooling of data results for extra long term.
Pain
Twenty-two studies, with 2,258 participants, provided post treatment effect on pain. Combining the results of high quality studies demonstrated significant benefit (mean difference) of stabilisation exercises for low back pain short, medium and long term of -7.93 (95% CI -11.74 to -4.12), -6.10 (95% CI -10.54 to -1.65) and -6.39 (95% CI -10.14 to -2.65) (Figure 2) respectively, when compared with any alternative treatment or control. However, the difference between groups was clinically insignificant with Minimal Clinical Important Difference (MCID) for pain being suggested as 24 to 40 [100], with between study heterogeneity high to moderate (I 2 = 67%, 50% and 45% respectively).

Forest plot of stabilisation versus alternative intervention: pain - long term. *Negative values favour stabilisation intervention, positive favour control.
Subgroup analysis of stabilisation exercises versus other forms of exercise demonstrated statistical significant short and medium term benefit, with a mean difference of -7.75 (95% CI -12.23 to -3.27) and -4.24 (95% CI -8.27 to -0.21). Differences between groups was clinically insignificant [100]. At long term there was no statistical or clinically significant difference; -3.06 (95% CI -6.74 to 0.63) (Figure 3). Between study heterogeneity was high to negligible (I 2 = 66%, 0% and 0% respectively).

Forest plot of stabilisation versus other exercises: pain - long term. *Negative values favour stabilisation intervention, positive favour control.
Combining the results of all studies for the sensitivity analysis provided very similar results (Additional file 1).
Disability
Twenty-four studies, with 2,359 participants, provided post treatment effect on disability. Combining the results of high quality studies demonstrated statistical significant benefit (mean difference) of stabilisation exercises for low back pain short and long term of -3.61 (95% CI -6.53 to -0.70), -3.92 (95% CI -7.25 to -0.59) (Figure 4), when compared with any alternative treatment or control. However, the difference between groups was clinically insignificant, with MCID for RMDQ 17 to 21 and 8 to 17 for ODI (converting all to 0 – 100 scale) [100]. There was no difference statistically or clinically medium term; -2.31 (95% CI -5.85 to 1.23). Between study heterogeneity was high to moderate (I 2 = 83%, 65% and 56% respectively).

Forest plot of stabilisation versus alternative intervention: disability - long term. *Negative values favour stabilisation intervention, positive favour control.
Subgroup analysis of stabilisation exercises versus other forms of exercises demonstrated significant short and medium term statistical benefit, but no significant clinical difference, (mean difference) of -3.63 (95% CI -6.69 to -0.58) and -3.56 (95% CI -6.47 to -0.66). There was no significant statistical or clinical long term benefit; -1.89 (95% CI -5.10 to 1.33) Figure 5. Between study heterogeneity was high to negligible (I 2 = 82%, 0% and 0% respectively).

Forest plot of stabilisation versus other exercises: disability - long term. *Negative values favour stabilisation intervention, positive favour control.
Combining the results of all studies for the sensitivity analysis provided results that were less favourable for stabilisation exercises for short to medium term, with similar long term results (Additional file 1).
Two high quality studies featured FABQ as an outcome measure. FABQ (physical activity) (0-24) and FABQ (work) (0-42) for Marshall and Kennedy [77] at short term follow-up had a non significant mean difference of 2.2 (95% CI −1.3 to 5.6) and 2.3 (95% CI −1.8 to 6.5) respectively in favour of stabilisation exercises, when compared to stationary bike exercises. There was a non significant medium term mean difference of −2.0 (95% CI −5.1 to 1.0) and −2.7 (95% CI −7.6 to 2.1) respectively in favour of the stationary bike. Short term mean difference for FABQ (physical activity) for Unsgaard-Tøndel et al [79] was non significant at -1.58 (-4.00 to 0.84) and -0.18 (-2.42 to 2.07) in favour of sling and general exercises, respectively. Mean difference for FABQ (work) was non significant at -0.40 (95% CI -3.81 to 3.01) in favour of slings and 0.25 (95% CI -2.74 to 3.24) in favour of stabilisation exercises, when compared to general exercises.
Discussion
Summary of main findings
The objective of this systematic review was to evaluate the current evidence for the benefit of stabilisation (or ‘core stability’) exercises for low back pain. The overall results of the meta-analysis indicates a trend favouring core stability exercises which is not regarded as clinically significant, when compared with any alternative treatment or control. Minimal clinical important difference (MCID) for pain has been suggested as 24 to 40, with 17 to 21 for RMDQ and 8 to 17 for ODI (converting all to 0 – 100 scale) [100]. Any reduction in favour of stabilisation exercises was potentially meaningless, with mean change scores for pain (7.93, 6.10 and 6.39) and disability (3.61, 2.31 and 3.92) falling well below these MCID levels.
The overall results of the subgroup meta-analysis suggest that stabilisation (or ‘core stability’) exercises for low back pain offer very minimal benefit in the short and medium term when compared with other forms of exercise, with mean change scores for pain (7.75 and 4.24) and disability (3.63 and 3.56) also falling well below the clinically significant level. There was no significant benefit in the long term, for pain or disability, when compared with any other form of exercise. Results were trending towards stabilisations, but results were not significant, and any benefit would be clinically insignificant, being largely below the MCID level.
In the subgroup analysis of long term follow-up for stabilisations exercises versus other forms of exercises heterogeneity was negligible (I 2 = 0%). Therefore, our results, that stabilisation exercises offer no benefit over alternative forms of exercises in the long term, can be considered robust.
Whilst not statistically significant, both studies that used FABQ as an outcome found that there was a trend of worse scores with stabilisation exercises, compared with stationary bikes, sling exercises and general exercises [77, 79]. The rehabilitation strategy surrounding stabilisation exercises has been challenged and has been suggested could encourage unhealthy thoughts and beliefs on pain and movement [101].
Limitations of included studies
For the meta-analysis of pain and disability for stabilisation versus any alternative treatment or placebo, high to moderate heterogeneity existed. I 2 scores of pain for short, medium and long term were 67%, 50% and 45%, and disability, 83%, 65% and 56% respectively. The high heterogeneity is possibly due to the different comparisons being made between trials, and this reduces the robustness of our short to medium term results. Overall, the interventions were applied to a wide variety of patients, including patients from low, medium or high socio-economic groups, unemployed or employed, having had investigations or no investigations, patients with or without leg pain, patients with acute or chronic symptoms and patients classed as ‘distressed’ or ‘distressed’ patients excluded. Patients that have high levels of fear avoidance scores are likely to have poor outcomes and compliance with biomedical models of pain and treatments, such as stabilisation exercises, and would likely do better with a biopsychosocial approach [101]. Cairns et al. [88], for example, excluded patients that were ‘distressed’, which perhaps biases results in favour of stabilisation exercises. This compares with Ferreira et al [70], whose participants were from low socio-economic groups, who are more likely to develop chronic pain states with worse outcomes, and would perhaps bias results in favour of alternative treatment protocols [102]. Furthermore, differences existed with how the treatments were delivered, class settings only, one to one treatment only, class/one to one treatment with home exercises or just home exercises, plus different amount of therapist contact times.
The studies included within the main meta-analysis had PEDro scores of ≥6, and as such were considered to have low bias. However, the main source of bias within the studies was blinding. No study blinded the therapist and few studies blinded the participants. Given that the pain and disability rating scales were patient self recorded it is possible that this could over estimate the treatment effect sizes. However blinding in active physiotherapy studies is difficult to achieve.
One of the limitations with long term follow-up of RCTs, particularly with exercise intervention, is the attrition rate. An uneven dropout has the risk of over estimating the effect size of treatment groups. For example Ferreira et al. [70] had an uneven dropout rate, with 9% for the general exercise group and 19% for the stabilisation group. This could easily bias the results in favour of the stabilisation group.
Limitations of this review
An extensive literature search was carried out, with two reviewers screening full texts independently for inclusion and the data extracting independently checked. This minimised bias within this review process, however, no attempt was made to source unpublished studies, nor studies published in any other language than English. It is thought that identifying unpublished trials minimises publication bias [103]. However, this approach has been questioned by others, who suggest that truly unpublished trials frequently have poor methodology, and ones with better methodology often eventually become published [104]. It is not possible to know if the inclusion, if available, of any unpublished trials would considerably alter our conclusions, or if this truly is a weakness of this review.
Comparison with other reviews
Our main findings differ very little from the 2008 review [13], however firmer conclusions about stabilisation exercises can be drawn from our review. In the 2008 review the majority of the studies favouring stabilisation exercises combined the exercises with some other form of treatment, implying that it was the package of care that was effective rather than stabilisation exercises alone. In our updated review the majority of the studies used stabilisation exercises as sole treatment, and as such the data synthesis looks more closely at stabilisation exercises as sole treatment.
Our findings were similar to the Wang et al. [80] review, which also concluded some short term benefit to pain and disability for stabilisation exercises over general exercise, with no long term benefit to pain. No comparison for long term follow-up for disability was made, and no attempt at analysing results against MCID was made. Of their five included articles we included three in our review. One was excluded for duplicating results from another included study, which was included in both of our and Wang et al’s reviews. It is therefore possible that their meta-analysis double counts these results [40, 79]. The other study we excluded during initial screening [105] looked at a relaxation yoga programme with meditation, chanting and counselling, and clearly doesn’t match our intervention definition. It is perhaps questionable that this study was included within Wang et al’s study [80].
Our findings differ from the Byström et al [22] review which concluded long term benefit to disability in favour of stabilisation exercises over general exercises and with regards to pain at intermediate term. The differences may be due to our inclusion of a further 15 publications; their inclusion of studies within the analysis with high risk of bias defined by means of a PEDro score of less than 6; or their use of a fixed effects meta-analysis model for pooled analysis where heterogeneity, as measured by I 2, was less than 50%. Choosing fixed versus random effect models solely based upon the test for heterogeneity is considered incorrect, and should be made upon which model best fits the distribution of effects sizes [106]. We used a random effects model on all analyses, since there is inherent heterogeneity in low back pain within the literature. Using a fixed effects model incorrectly could over estimate the pooled effect sizes and underestimate the confidence interval width, thus reducing reliability of results [106].
Conclusion
The results of this current systematic review suggest that stabilisation exercises improves low back pain symptoms, but no better than any other form of active exercise in the long term. The low levels of heterogeneity and large number of high methodological quality of available studies, at long term follow-up, strengthen our current findings. There is a trend of worse fear avoidance scores.
This review cannot recommend stabilisation exercises for low back pain in preference to other forms of general exercise, and further research is unlikely to considerably alter this conclusion.
References
Nachemson A, Jonsson E: Neck and Back Pain: The Scientific Evidence of Causes, Diagnosis, and Treatment. 2000, Philadelphia: Lippincott Williams and Wilkins
Palmer KT, Walker-Bone K, Griffin MJ, Syddall H, Pannett B, Coggon D, Cooper C: Prevalence and occupational associations of neck pain in the British population. Scand J Work Environ Heal. 2001, 27: 49-56. 10.5271/sjweh.586.
Walker BF: The prevalence of low back pain: a systematic review of the literature from 1966 to 1998. J Spinal Disord. 2000, 13: 205-217. 10.1097/00002517-200006000-00003.
Hestbaek L, Leboeuf-Yde C, Manniche C: Low back pain: what is the long-term course? A review of studies of general patient populations. Eur Spine J. 2003, 12: 149-165.
Maniadakis N, Gray A: The economic burden of back pain in the UK. Pain. 2000, 84: 95-103. 10.1016/S0304-3959(99)00187-6.
National Institute for Health and Care Excellence: Low Back Pain. Early Management of Persistent Non-Specific Low Back Pain [CG88]. 2009
Pain in Europe; A 2003 Report. 2003,http://www.paineurope.com,
Department of Health (DoH): The NHS Plan: A Plan for Investment a Plan for Reform. 2000, 82-
Liddle SD, David Baxter G, Gracey JH: Physiotherapists’ use of advice and exercise for the management of chronic low back pain: a national survey. Man Ther. 2009, 14: 189-196. 10.1016/j.math.2008.01.012.
Hodges PW, Richardson CA: Inefficient muscular stabilization of the lumbar spine associated with low back pain. A motor control evaluation of transversus abdominis. Spine (Phila Pa 1976). 1996, 21: 2640-2650. 10.1097/00007632-199611150-00014.
Hodges PW, Richardson CA: Altered trunk muscle recruitment in people with low back pain with upper limb movement at different speeds. Arch Phys Med Rehabil. 1999, 80: 1005-1012. 10.1016/S0003-9993(99)90052-7.
Richardson C, Jull G, Hodges P, Hides J: Therapeutic Exercise for Spinal Segmental Stabilization: In Lower Back Pain. 1999, Edinburgh: Churchill Livingstone
May S, Johnson R: Stabilisation exercises for low back pain: a systematic review. Physiotherapy. 2008, 94 (3): 179-189. 10.1016/j.physio.2007.08.010.
Mannion AF, Pulkovski N, Schenk P, Hodges PW, Gerber H, Loupas T, Gorelick M, Sprott H: A new method for the noninvasive determination of abdominal muscle feedforward activity based on tissue velocity information from tissue Doppler imaging. J Appl Physiol. 2008, 104: 1192-1201. 10.1152/japplphysiol.00794.2007.
Vasseljen O, Fladmark AM, Westad C, Torp HG: Onset in abdominal muscles recorded simultaneously by ultrasound imaging and intramuscular electromyography. J Electromyogr Kinesiol. 2009, 19 (2): e23-e31. 10.1016/j.jelekin.2007.07.013.
Shojania KG, Sampson M, Ansari MT, Ji J, Doucette S, Moher D: How quickly do systematic reviews go out of date? A survival analysis. Ann Intern Med. 2007, 147: 224-233. 10.7326/0003-4819-147-4-200708210-00179.
Macedo LG, Maher CG, Latimer J, McAuley JH: Motor control exercise for persistent, nonspecific low back pain: a systematic review. Phys Ther. 2009, 89: 9-25. 10.2522/ptj.20080103.
Hauggaard A, Persson AL: Specific spinal stabilisation exercises in patients with low back pain – a systematic review. Phys Ther Rev. 2007, 12 (3): 233-248. 10.1179/108331907X222949.
Ferreira PH, Ferreira ML, Maher CG, Herbert RD, Refshauge K: Specific stabilisation exercise for spinal and pelvic pain: a systematic review. Aust J Physiother. 2006, 52: 79-88. 10.1016/S0004-9514(06)70043-5.
Rackwitz B, de Bie R, Limm H, von Garnier K, Ewert T, Stucki G: Segmental stabilizing exercises and low back pain. What is the evidence? A systematic review of randomized controlled trials. Clin Rehabil. 2006, 20: 553-567. 10.1191/0269215506cr977oa.
Wang XQ, Zheng JJ, Yu ZW, Bi X, Lou SJ, Liu J, Cai B, Hua YH, Wu M, Wei ML, Shen HM, Chen Y, Pan YJ, Xu GH, Chen PJ, Eldabe S: A meta-analysis of core stability exercise versus general exercise for chronic low back pain. PLoS One. 2012, 7: e52082-10.1371/journal.pone.0052082.
Byström MG, Rasmussen-Barr E, Grooten WJA: Motor control exercises reduces pain and disability in chronic and recurrent low back pain: a meta-analysis. Spine (Phila Pa 1976). 2013, 38: E350-8. 10.1097/BRS.0b013e31828435fb.
Moher D, Liberati A, Tetzlaff J, Altman DG: Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009, 6 (7): e1000097-10.1371/journal.pmed.1000097.
Norris C: Back Stability. 2000, Leeds: Human Kinetics Europe Ltd
O’Sullivan PB, Phyty GD, Twomey LT, Allison GT: Evaluation of specific stabilizing exercise in the treatment of chronic low back pain with radiologic diagnosis of spondylolysis or spondylolisthesis. Spine (Phila Pa 1976). 1997, 22: 2959-2967. 10.1097/00007632-199712150-00020.
Cohen J: A coefficient of agreement of nominal scales. Educ Psychol Meas. 1960, 20: 37-46. 10.1177/001316446002000104.
Landis JR, Koch GG: The measurement of observer agreement for categorical data. Biometrics. 1977, 33: 159-174. 10.2307/2529310.
Fleiss JL: Statistical Methods for Rates and Proportions. 1981, New York: John Wiley, 2
Miyamoto GC, Costa LOP, Galvanin T, Cabral CMN: Efficacy of the addition of modified pilates exercises to a minimal intervention in patients with chronic low back pain: a randomized controlled trial. Phys Ther. 2012, 93 (3): 310-320.
Mohseni-Bandpei MA, Rahmani N, Behtash H, Karimloo M: The effect of pelvic floor muscle exercise on women with chronic non-specific low back pain. J Bodyw Mov Ther. 2011, 15: 75-81. 10.1016/j.jbmt.2009.12.001.
Smith D, Bissell G, Bruce-Low S, Wakefield C: The effect of lumbar extension training with and without pelvic stabilization on lumbar strength and low back pain. J Back Musculoskelet Rehabil. 2011, 24: 241-249.
Wajswelner H, Metcalf B, Bennell K: Clinical pilates versus general exercise for chronic low back pain: randomized trial. Med Sci Sports Exerc. 2012, 44: 1197-205. 10.1249/MSS.0b013e318248f665.
Sung PS: Disability and back muscle fatigability changes following two therapeutic exercise interventions in participants with recurrent low back pain. Med Sci Monit. 2013, 19: 40-8.
Babur MN, Ahmed D, Rashid F: Comparing the effectiveness of lumbar stabilization exercises with general spinal exercises in patients with postero-lateral disc herniation. Rawal Med J. 2011, 36: 259-261.
Kumar S, Sharma VP, Negi MPS: Efficacy of dynamic muscular stabilization techniques (DMST) over conventional techniques in rehabilitation of chronic low back pain. J Strength Cond Res. 2009, 23: 2651-2659. 10.1519/JSC.0b013e3181b3dde0.
Ferreira PH, Ferreira ML, Maher CG, Refshauge K, Herbert RD, Hodges PW: Changes in recruitment of transversus abdominis correlate with disability in people with chronic low back pain. Br J Sports Med. 2010, 44: 1166-1172. 10.1136/bjsm.2009.061515.
Kumar SP: Efficacy of segmental stabilization exercise for lumbar segmental instability in patients with mechanical low back pain: a randomized placebo controlled crossover study. N Am J Med Sci. 2011, 3: 456-461.
Norris C, Matthews M: The role of an integrated back stability program in patients with chronic low back pain. Complement Ther Clin Pract. 2008, 14: 255-63. 10.1016/j.ctcp.2008.06.001.
Stankovic A, Lazovic M, Kocic M, Dimitrijevic L, Stankovic I, Zlatanovic D, Dimitrijevic I: Lumbar stabilization exercises in addition to strengthening and stretching exercises reduce pain and increase function in patients with chronic low back pain: randomized clinical open-label study. Turkish J Phys Med Rehabil. 2012, 58: 177-183. 10.4274/tftr.22438.
Vasseljen O, Fladmark AM: Abdominal muscle contraction thickness and function after specific and general exercises: a randomized controlled trial in chronic low back pain patients. Man Ther. 2010, 15: 482-489. 10.1016/j.math.2010.04.004.
Vasseljen O, Unsgaard-Tondel M, Westad C, Mork PJ: Effect of core stability exercises on feed-forward activation of deep abdominal muscles in chronic low back pain: a randomized controlled trial [with consumer summary]. Spine (Phila Pa 1976). 2012, 37: 1101-1108. 10.1097/BRS.0b013e318241377c.
Higgins J, Deeks J: Cochrane Handbook: General Methods For Cochrane Reviews: Ch 7: Selecting Studies and Collecting Data. Cochrane Handb Syst Rev Interv. Volume 6. Edited by: Higgins PTJ, Green S. 2011, Wiley-Blackwell, 151-186. [Cochrane Book Series]
Javadian Y, Behtash H, Akbari M, Taghipour-Darzi M, Zekavat H: The effects of stabilizing exercises on pain and disability of patients with lumbar segmental instability. J Back Musculoskelet Rehabil. 2012, 25: 149-155.
Rhee HS, Kim YH, Sung PS: A randomized controlled trial to determine the effect of spinal stabilization exercise intervention based on pain level and standing balance differences in patients with low back pain. Med Sci Monit. 2012, 18: CR174-81.
Rasmussen-Barr E, Ang B, Arvidsson I, Nilsson-Wikmar L: Graded exercise for recurrent low-back pain: a randomized, controlled trial with 6-, 12-, and 36-month follow-ups. Spine (Phila Pa 1976). 2009, 34: 221-228. 10.1097/BRS.0b013e318191e7cb.
Furlan JC, Kalsi-Ryan S, Kailaya-Vasan A, Massicotte EM, Fehlings MG: Functional and clinical outcomes following surgical treatment in patients with cervical spondylotic myelopathy: a prospective study of 81 cases. J Neurosurg Spine. 2011, 14: 348-355. 10.3171/2010.10.SPINE091029.
Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M: Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003, 83: 713-721.
Verhagen AP, De Vet HCW, De Bie RA, Kessels AGH, Boers M, Bouter LM, Knipschild PG: The Delphi list: a criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. J Clin Epidemiol. 1998, 51: 1235-1241. 10.1016/S0895-4356(98)00131-0.
Sherrington C, Herbert RD, Maher CG, Moseley AM: PEDro. A database of randomized trials and systematic reviews in physiotherapy. Man Ther. 2000, 5: 223-226. 10.1054/math.2000.0372.
PEDro. Physiotherapy Evidence Database. [http://www.pedro.org.au/]
Moseley AM, Herbert RD, Sherrington C, Maher CG: Evidence for physiotherapy practice: a survey of the Physiotherapy Evidence Database (PEDro). Aust J Physiother. 2002, 48: 43-49. 10.1016/S0004-9514(14)60281-6.
Herbert RD: How to estimate treatment effects from reports of clinical trials. I: continuous outcomes. Aust J Physiother. 2000, 46: 229-235. 10.1016/S0004-9514(14)60334-2.
Wallace BC, Dahabreh IJ, Trikalinos TA, Lau J, Trow P, Schmid CH: Closing the gap between methodologists and end-users: R as a computational back-end. Wiley Interdiscip Rev Comput. 2012, 49: 1-15.
Higgins J, Thompson S, Deeks J, Altman D: Measuring inconsistency in meta-analyses. BMJ. 2003, 327: 557-60. 10.1136/bmj.327.7414.557.
DerSimonian R, Laird N: Meta-analysis in clinical trials. Control Clin Trials. 1986, 7: 177-188. 10.1016/0197-2456(86)90046-2.
Kluge J, Hall D, Louw Q, Theron G, Grové D: Specific exercises to treat pregnancy-related low back pain in a South African population. Int J Gynaecol Obstet. 2011, 113: 187-191. 10.1016/j.ijgo.2010.10.030.
Mannion AF, Denzler R, Dvorak J, Müntener M, Grob D: A randomised controlled trial of post-operative rehabilitation after surgical decompression of the lumbar spine. Eur Spine J. 2007, 16: 1101-1117. 10.1007/s00586-007-0399-6.
Ammar TA, Mitchell K, Saleh A: Stabilization exercises in postnatal low back pain. Indian J Physiother Occup Ther. 2011, 5 (1): 122-124.
Bi X, Zhao J, Zhao L, Liu Z, Zhang J, Sun D, Song L, Xia Y: Pelvic floor muscle exercise for chronic low back pain. J Int Med Res. 2013, 41: 146-152. 10.1177/0300060513475383.
Gatti R, Faccendini S, Tettamanti A, Barbero M, Balestri A, Calori G: Efficacy of trunk balance exercises for individuals with chronic low back pain: a randomized clinical trial. J Orthop Sport Phys Ther. 2011, 41 (8): 542-552. 10.2519/jospt.2011.3413.
Shnayderman I, Katz-Leurer M: An aerobic walking programme versus muscle strengthening programme for chronic low back pain: a randomized controlled trial. Clin Rehabil. 2013, 27: 207-214. 10.1177/0269215512453353.
Unsgaard-Tøndel M, Lund Nilsen TI, Magnussen J, Vasseljen O: Is activation of transversus abdominis and obliquus internus abdominis associated with long-term changes in chronic low back pain? A prospective study with 1-year follow-up. Br J Sports Med. 2012, 46: 729-34. 10.1136/bjsm.2011.085506.
Yoo Y-D, Lee Y-S: The effect of core stabilization exercises using a sling on pain and muscle strength of patients with chronic low back pain. J Phys Ther Sci. 2012, 24: 671-10.1589/jpts.24.671.
Goel P, Veqar Z, Quddus N: Effects of local versus global stabilizer strengthening in chronic low back pain. Indian J Physiother Occup Ther. 2010, 4: 68-74.
Brooks C, Marshall PW, Kennedy S: Specific trunk and general exercise elicit similar changes in anticipatory postural adjustments in patients with chronic low back pain. Spine (Phila Pa 1976). 2012, 37 (25): E1543-E1550. 10.1097/BRS.0b013e31826feac0.
Muthukrishnan R, Shenoy SD, Jaspal SS, Nellikunja S, Fernandes S: The differential effects of core stabilization exercise regime and conventional physiotherapy regime on postural control parameters during perturbation in patients with movement and control impairment chronic low back pain. Sports Med Arthrosc Rehabil Ther Technol. 2010, 2: 13-10.1186/1758-2555-2-13.
Akbaria A, Khorashadizadeh S, Abdi G: The effect of motor control exercise versus general exercise on lumbar local stabilizing muscles thickness: randomized controlled trial of patients with chronic low back pain. J Back Musculoskelet Rehabil. 2008, 21 (2): 105-112.
Costa LOP, Maher CG, Latimer J, Hodges PW, Herbert RD, Refshauge KM, McAuley JH, Jennings MD: Motor control exercise for chronic low back pain: a randomized placebo-controlled trial. Phys Ther. 2009, 89: 1275-1286. 10.2522/ptj.20090218.
Critchley DJ, Ratcliffe J, Noonan S, Jones RH, Hurley MV: Effectiveness and cost-effectiveness of three types of physiotherapy used to reduce chronic low back pain disability: a pragmatic randomized trial with economic evaluation. Spine (Phila Pa 1976). 2007, 32: 1474-1481. 10.1097/BRS.0b013e318067dc26.
Ferreira ML, Ferreira PH, Latimer J, Herbert RD, Hodges PW, Jennings MD, Maher CG, Refshauge KM: Comparison of general exercise, motor control exercise and spinal manipulative therapy for chronic low back pain: a randomized trial. Pain. 2007, 131: 31-37. 10.1016/j.pain.2006.12.008.
França FR, Burke TN, Hanada ES, Marques AP: Segmental stabilization and muscular strengthening in chronic low back pain: a comparative study. Clinics (Sao Paulo). 2010, 65: 1013-1017. 10.1590/S1807-59322010001000015.
França FR, Burke TN, Caffaro RR, Ramos LA, Marques AP: Effects of muscular stretching and segmental stabilization on functional disability and pain in patients with chronic low back pain: a randomized, controlled trial. J Manipulative Physiol Ther. 2012, 35: 279-285. 10.1016/j.jmpt.2012.04.012.
Gladwell V, Head S, Haggar M, Beneke R: Does a program of pilates improve chronic non-specific low back pain?. J Sport Rehabil. 2006, 15: 338-350.
Inani SB, Selkar SP: Effect of core stabilization exercises versus conventional exercises on pain and functional status in patients with non-specific low back pain: a randomized clinical trial. J Back Musculoskelet Rehabil. 2013, 26: 37-43.
Kumar S, Sharma VP, Shukla R, Dev R: Comparative efficacy of two multimodal treatments on male and female sub-groups with low back pain (part II). J Back Musculoskelet Rehabil. 2010, 23: 1-9.
Macedo LG, Latimer J, Maher CG, Hodges PW, McAuley JH, Nicholas MK, Tonkin L, Stanton CJ, Stanton TR, Stafford R: Effect of motor control exercises versus graded activity in patients with chronic nonspecific low back pain: a randomized controlled trial. Phys Ther. 2012, 92: 363-77. 10.2522/ptj.20110290.
Marshall PWM, Kennedy S, Brooks C, Lonsdale C: Pilates exercise or stationary cycling for chronic nonspecific low back pain: does it matter? a randomized controlled trial with 6-month follow-up. Spine (Phila Pa 1976). 2013, 38: E952-9. 10.1097/BRS.0b013e318297c1e5.
Moon HJ, Choi KH, Kim DH, Kim HJ, Cho YK, Lee KH, Kim JH, Choi YJ: Effect of lumbar stabilization and dynamic lumbar strengthening exercises in patients with chronic low back pain. Ann Rehabil Med. 2013, 37: 110-7. 10.5535/arm.2013.37.1.110.
Unsgaard-Tøndel M, Fladmark AM, Salvesen Ø, Vasseljen O: Motor control exercises, sling exercises, and general exercises for patients with chronic low back pain: a randomized controlled trial with 1-year follow-up. Phys Ther. 2010, 90: 1426-1440. 10.2522/ptj.20090421.
Xueqiang W, Jiejiao Z, Xia B, Jing L: Effect of core stability training on patients with chronic low back pain. HealthMED. 2012, 6: 754-759.
Stuge B, Laerum E, Kirkesola G, Vøllestad N: The efficacy of a treatment program focusing on specific stabilizing exercises for pelvic girdle pain after pregnancy: a randomized controlled trial. Spine (Phila Pa 1976). 2004, 29: 351-359. 10.1097/01.BRS.0000090827.16926.1D.
Bakhtiary AH, Safavi-Farokhi Z, Rezasoltani A: Lumbar stabilizing exercises improve activities of daily living in patients with lumbar disc herniation. J Back Musculoskelet Rehabil. 2005, 18: 55-60.
Filiz M, Cakmak A, Ozcan E: The effectiveness of exercise programmes after lumbar disc surgery: a randomized controlled study. Clin Rehabil. 2005, 19: 4-11. 10.1191/0269215505cr836oa.
Elden H, Ladfors L, Olsen MF, Ostgaard H-C, Hagberg H: Effects of acupuncture and stabilising exercises as adjunct to standard treatment in pregnant women with pelvic girdle pain: randomised single blind controlled trial. BMJ. 2005, 330: 761-10.1136/bmj.38397.507014.E0.
Shaughnessy M, Caulfield B: A pilot study to investigate the effect of lumbar stabilisation exercise training on functional ability and quality of life in patients with chronic low back pain. Int J Rehabil Res. 2004, 27: 297-301. 10.1097/00004356-200412000-00007.
Hides JA, Jull GA, Richardson CA: Long-term effects of specific stabilizing exercises for first-episode low back pain. Spine (Phila Pa 1976). 2001, 26: E243-E248. 10.1097/00007632-200106010-00004.
Goldby LJ, Moore AP, Doust J, Trew ME: A randomized controlled trial investigating the efficiency of musculoskeletal physiotherapy on chronic low back disorder. Spine (Phila Pa 1976). 2006, 31: 1083-1093. 10.1097/01.brs.0000216464.37504.64.
Cairns MC, Foster NE, Wright C: Randomized controlled trial of specific spinal stabilization exercises and conventional physiotherapy for recurrent low back pain. Spine (Phila Pa 1976). 2006, 31: E670-E681. 10.1097/01.brs.0000232787.71938.5d.
Hides JA, Richardson CA, Jull GA: Multifidus muscle recovery is not automatic after resolution of acute, first-episode low back pain. Spine (Phila Pa 1976). 1996, 21: 2763-2769. 10.1097/00007632-199612010-00011.
Moseley L: Combined physiotherapy and education is efficacious for chronic low back pain. Aust J Physiother. 2002, 48: 297-302. 10.1016/S0004-9514(14)60169-0.
Niemistö L, Lahtinen-Suopanki T, Rissanen , Lindgren K, Sarna S, Hurri H: A randomized trial of combined manipulation, stabilizing exercises, and physician consultation compared to physician consultation alone for chronic low back pain. Spine (Phila Pa 1976). 2003, 28: 2185-91. 10.1097/01.BRS.0000085096.62603.61.
Rasmussen-Barr E, Nilsson-Wikmar L, Arvidsson I: Stabilizing training compared with manual treatment in sub-acute and chronic low-back pain. Man Ther. 2003, 8: 233-241. 10.1016/S1356-689X(03)00053-5.
Childs MJD, Fritz JM, Flynn TW, Irrgang JJ, Johnson MKK: Article a clinical prediction rule to identify patients with low back pain most likely to benefit from spinal manipulation : a validation study. Ann Intern Med. 2004, 141: 920-928. 10.7326/0003-4819-141-12-200412210-00008.
Monticone M, Barbarino A, Testi C, Arzano S, Moschi A, Negrini S: Symptomatic efficacy of stabilizing treatment versus laser therapy for sub-acute low back pain with positive tests for sacroiliac dysfunction: a randomised clinical controlled trial with 1 year follow-up. Eura Medicophys. 2004, 40: 263-268.
Koumantakis GA, Watson PJ, Oldham JA: Trunk muscle stabilization training plus general exercise versus general exercise only: randomized controlled trial of patients with recurrent low back pain. Phys Ther. 2005, 85: 209-225.
Celestini M, Marchese A, Serenelli A, Graziani G: A randomized controlled trial on the efficacy of physical exercise in patients braced for instability of the lumbar spine. Eura Medicophys. 2005, 41: 223-231.
Miller ER, Schenk RJ, Karnes JL, Rousselle JG: A comparison of the McKenzie approach to a specific spine stabilization program for chronic low back pain. J Man Manip Ther. 2005, 103-112.
Brennan GP, Fritz JM, Hunter SJ, Thackeray A, Delitto A, Erhard RE: Identifying subgroups of patients with acute/subacute “nonspecific” low back pain: results of a randomized clinical trial. Spine (Phila Pa 1976). 2006, 31: 623-631. 10.1097/01.brs.0000202807.72292.a8.
Niemistö L, Rissanen P, Sarna S, Lahtinen-Suopanki T, Lindgren K-A, Hurri H: Cost-effectiveness of combined manipulation, stabilizing exercises, and physician consultation compared to physician consultation alone for chronic low back pain: a prospective randomized trial with 2-year follow-up. Spine (Phila Pa 1976). 2005, 30: 1109-1115. 10.1097/01.brs.0000162569.00685.7b.
Maughan EF, Lewis JS: Outcome measures in chronic low back pain. Eur Spine J. 2010, 19: 1484-1494. 10.1007/s00586-010-1353-6.
Nijs J, Roussel N, Paul van Wilgen C, Köke A, Smeets R: Thinking beyond muscles and joints: therapists’ and patients’ attitudes and beliefs regarding chronic musculoskeletal pain are key to applying effective treatment. Man Ther. 2013, 18: 96-102. 10.1016/j.math.2012.11.001.
Katz J: Lumbar disc disorders and low-back pain: socioeconomic factors and consequences. J Bone Jt Surg. 2006, 88: 21-24. 10.2106/JBJS.E.01273.
Lefebvre C, Manheimer E, Glanville J: Searching for studies. Cochrane Handb Syst Rev Interv. Edited by: Higgins J, Green S. 2008, Chichester: Wiley-Blackwell, 95-150.
Van Driel ML, De Sutter A, De Maeseneer J, Christiaens T: Searching for unpublished trials in Cochrane reviews may not be worth the effort. J Clin Epidemiol. 2009, 62 (8): 838-844. 10.1016/j.jclinepi.2008.09.010.
Tekur P, Singphow C, Nagendra HR, Raghuram N: Effect of short-term intensive yoga program on pain, functional disability and spinal flexibility in chronic low back pain: a randomized control study. J Altern Complement Med. 2008, 14: 637-644. 10.1089/acm.2007.0815.
Borenstein M, Hedges L, Higgins J, Rothstein H: Introduction to Meta-Analysis. 2009, New York: John Wiley & Sons, Ltd., 1
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2474/15/416/prepub
Source of funding
Funding for open-access publication was gained via the research support fund from the School of Health & Related Research, University of Sheffield. No other funding was obtained.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
BS was responsible for conception and design, publication screening, acquisition of data, analysis and interpretation, drafting and revising the manuscript. CL was responsible for conception and design, publication screening, data interpretation, reviewing and revising the manuscript. SM was responsible for acquisition of data, data interpretation, reviewing and revising the manuscript. All authors have read and approved the final manuscript.
Electronic supplementary material
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Smith, B.E., Littlewood, C. & May, S. An update of stabilisation exercises for low back pain: a systematic review with meta-analysis. BMC Musculoskelet Disord 15, 416 (2014). https://doi.org/10.1186/1471-2474-15-416
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2474-15-416