
Abstract
Background
Congenital fibiosis of the extraocular muscles (CFEOM1) refers to a group of congenital eye movement disorders that are characterized by non-progressive restrictive ophthalmoplegia. We present clinical and surgical data on affected members of a classic CFEOM1 family.
Methods
Ten members of a fifteen-member, three-generation Italian family affected by classic CFEOM participated in this study. Each affected family member underwent ophthalmologic (corrected visual acuity, pupillary function, anterior segment and fundus examination), orthoptic (cover test, cover-uncover test, prism alternate cover test), and preoperative examinations. Eight of the ten affected members had surgery and underwent postoperative examinations. Surgical procedures are listed.
Results
All affected members were born with varying degrees of bilateral ptosis and ophthalmoplegia with both eyes fixed in a hypotropic position (classic CFEOM). The affected members clinical data prior to surgery, surgery procedures and postoperative outcomes are presented. On 14 operated eyes to correct ptosis there was an improvement in 12 eyes. In addition, the head position improved in all patients.
Conclusions
Surgery is effective at improving ptosis in the majority of patients with classic CFEOM. However, the surgical approach should be individualized to each patient, as inherited CFEOM exhibits variable expressivity and the clinical features may differ markedly between affected individuals, even within the same family.
Similar content being viewed by others


Background
Congenital fibrosis of the extraocular muscles (CFEOM) refers to a group of congenital eye movement disorders that are characterized by non-progressive restrictive ophthalmoplegia. An early description of CFEOM was given by Baumgarten in 1840[1] and Heuck is credited with the first report of a familial occurrence in 1879[2]. Affected individuals are born with their eyes fixed in an abnormal position, are unable to move them normally, and often develop a compensatory chin-up position to see. CFEOM is often associated with ptosis and depending on the subtype, can affect one or both eyes. Table 1 lists the general clinical features of CFEOM as classified by the Authors. Individuals with classic CFEOM are born with ptosis and their eyes in a hypotropic position which they are unable to elevate above the midline. In familial cases, affected family members may present with similar clinical phenotypes, or exhibit a range of clinical severity [3–6]. If left untreated, CFEOM can result in amblyopia, if binocular vision is lost, and the patient may become a strict monofixator.
The CFEOM conditions were traditionally classified based on clinical differences and are referred to in the literature by many names including: congenital fibrosis of the extraocular muscles [7–11]; general fibrosis syndrome[5] ; congenital static familial ophthalmoplegia [12]; familial musculofascial anomaly [13] ; familial opthalmoplegia with co-contraction [14]; congenital external ophthalmoplegia[3, 15, 16] ; and hereditary congenital external ophthalmoplegia [17]. As the genetic basis of these disorders became known, however, their classification changed to one combining both genetic etiology and clinical presentation. Therefore, clinical entities that have the same underlying genetic cause, regardless of clinical variations, are being grouped first by genetic aetiology and then by clinical differences [18–20].
Three genetic loci for CFEOM have been identified (CFEOM1–3) [9, 10, 21–28]
While the aetiology of CFEOM is not fully understood, there is evidence of a neurological rather than myopathic basis. A neuropathologic examination of an individual exhibiting a classic CFEOM phenotype whose disease gene maps to the CFEOM1 locus revealed an absence of the superior division of the third cranial nerve and corresponding oculomotor subnuclei [11], suggesting a primary neuropathic aetiology with secondary myopathic changes, rather than a primary myopathic aetiology.
This finding was similar to postmortem findings showing an absence of the abducens nucleus and abducens nerve in individuals with isolated Duane syndrome, another congenital non-progressive ophthalmoplegia [29, 30]. Furthermore, Gottlob described a patient with CFEOM and elevation of one eye during tooth brushing. This is the first of aberrant regeneration between the nerve to the superior rectus and the trigeminal nerve in a patient with CFEOM, and further supports a primary developmental abnormality of the cranial nerves in CFEOM [31].
Treatment for CFEOM is primarily surgical and aimed at the elimination or improvement of an unacceptable head position, the reduction of ptosis, and/or the elimination or reduction of significant misalignment of the eyes [32]. Unfortunately, nothing can be done to correct the absence of eye movements. Apt and Axelrod [33] demonstrated that satisfactory cosmesis can be obtained with appropriate extraocular muscle surgery, that amblyopia can be successfully treated when recognized early, and that uncomfortable head position can be relieved with proper alignement of the eyes.
They used a strict sequence of surgical steps when the eyes are fixed in the down and out position, beginning with vertical, then horizontal muscle surgery, and finally, eyelid surgery. In case of recurrence of any appreciable degree of deviation, they performed reexploration, lysis of adhesions, and additional appropriate eye muscle surgery. Because the rectus muscle procedures often cause a change in relative eyelid position, blepharoptosis surgery is done last. Houtman [17] treated thirteen individuals affected by CFEOM by a recession or a disinsertion of the inferior rectus muscle and a frontalis suspension procedure in one stage. Boergen [34] reported a large series of CFEOM patients in whom an aggressive surgical approach led to good clinical results. Ferrer [35, 36] proposed "maximal surgery" at the first procedure: unsutured tenomyectomy (9–10 mm) of the inferior rectus, exeresis of the lower-half fascias, recession of the conjunctiva; tenectomy of the superior oblique; and, when not absent, resection of the superior rectus. Despite this aggressive surgery, he has not experienced overcorrections to date. Three to four months later, he corrected ptosis, and, if it existed, the horizontal deviation; this simplified rational approach has been predictably efficient in his experience. Although treatment of these patients is difficult, visual rehabilitation can be achieved [37]. This is accomplished with occlusion for amblyopia and spectacle correction of refractive errors and anisometropia. The goal of strabismus surgery is to release muscle restriction and to align the eye as closely as possible to straight in primary position. Binocular vision is rarely attained post surgery, even with a good surgical result, and repeat surgery is often necessary if a significant amount of residual deviation gradually develops after surgical intervention [32, 33]. We present clinical and, if surgery was done, surgical data on ten affected members of a classic CFEOM1 family.
Methods
Pedigree
The family (3 generations) was identified in the ophthalmological clinic of the University of Naples "Federico II". The ten affected family members each underwent ophthalmologic (corrected visual acuity, examination of pupillary function, anterior segment and fundus), orthoptic (cover test, cover-uncover test, prism alternate cover test), and preoperative examinations.
To classify the degree of ptosis in our patients the amount of cornea left "covered" by the palpebrae was measured [38]. A baseline measurement of 2 mm for the non-ptosis state was calculated. Using this baseline measurements, the degree of ptosis was quantified as follows: Absence of ptosis:2 mm of cornea "covered"; Ist degree ptosis:4 mm of cornea "covered"; II degree ptosis: 5–6 mm of cornea "covered"; III degree ptosis: >6 mm of cornea "covered".
The amount of ptosis was measured without frontalis innervation, and during this process the frontalis muscle was immobilized using the hands, and the eyebrow was kept in the normal position. The type of surgery performed to correct ptosis depended on the level of the patient's eyelid levator function. Levator function was assessed by measuring the palpebral excursion [39]. This was done by doing a measurement from the point in the extreme down gaze to the point in the extreme upgaze. The levator muscle function (mm) was quantified as follows: 10–15 mm: excellent; 8 mm: good; 5–7 mm: sufficient; <4 mm: poor.
All affected members who had surgery (eight of the ten) also underwent postoperative examinations.
Prior to surgery we found that an evaluation of the function of the frontalis muscle is recommended because some varieties of complete congenital ophthalmoplegia involve the mimetic frontal muscles. In addition, the function of the lacrimal tears and sensitivity of the cornea should be tested. To avoid post surgical negative reactions (corneal exposure)treatment with artificial tears in the form of hydroxymethylcellulose, or polyvinylpyrrolidine alkaline eye drops and with simple ointement at night, is recommended after surgery.
Surgical Treatment
Eight of the ten affected members had surgery. Surgical procedures are listed in Additional File 1.
Results
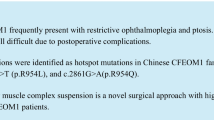
Ten members of a fifteen-member, three-generation Italian family who are affected by classic CFEOM participated in this study (figure 1, figure 2). All affected members were born with bilateral ptosis and varying degrees of ophthalmoplegia with both eyes fixed in a hypotropic position. None were able to elevate either eye above the horizontal midline. All affected members presented with a compensatory chin up position and head turn prior to surgical intervention.

F.Family pedigree

Seven members of the family affected by CFEOM1 Top: From the left : III:1 after the last operation III:2 after the last operation II:2 after the last operation II:4 after the last operation III:7 before surgery Bottom: III:5 before surgery III:4 before surgery
Examination of pupillary function, anterior segment and fundus were normal in all ten affected members. Eight of the ten affected members underwent strabismus and ptosis surgery. Forced duction testing done during surgery of these individuals was positive, showing a restriction of eye movement. The affected family members' clinical presentations prior to surgery, surgical procedures performed and postoperative outcomes are shown in Additional File 1.
Case descriptions(the age of the patient shown for the year 2000)
Case I: 1 is a 66 year old man who was born with asymmetric ptosis (1st degree in the right eye and 3rd degree in the left eye), bilateral ophthalmoplegia with complete restriction of up-gaze and marked restriction of down-gaze. He has not had any surgery. He has esotropia of +30 prism dioptres, corrected visual acuity of 6/8 in right eye and 6/12 in left eye, and simple hypermetropic astigmatism. The levator function is absent in the left eye and sufficient (6 mm) in the right eye.
Case II: 2 is a 41 year old woman who was born with marked symmetric ptosis (3rd degree), bilateral ophthalmoplegia with complete restriction of up-gaze and marked restriction of down-gaze. She had exotropia of -30 prism dioptres, corrected visual acuity of 6/8 (RE) and 6/7 (LE), and simple hypermetropic astigmatism. The levator function was sufficient (5 mm) in both eyes. She had surgery in 1967 at age 8 years (Both eyes: recession Inferior Rectus Muscle(IRM)5 mm, resection Superior Rectus Muscle(SRM) 6 mm, eyelid levator resection 10 mm by skin approach) and in 1968 at age 9 years (RE: superior oblique tenotomy; LE: recession Lateral Rectus Muscle(LRM) 5 mm, resection MRM(Medial Rectus Muscle) 9 mm). Postoperative results showed an improvement in degree of ptosis (now mild) in both eyes, and exotropia changed from -30 prism dioptres prior to surgery to -10 prism dioptres. The patient was operated on all recti muscles, but did not have an anterior segmenti ischemia.
Case II: 4 is a 38 year old man who was born with marked symmetric ptosis (3rd degree), bilateral ophthalmoplegia with complete restriction of up-gaze and very marked restriction of down-gaze. He had esotropia of +20 prism dioptres, corrected visual acuity of 6/60 (RE) and 6/8 (LE), and simple myopic astigmatism. His levator function was poor (4 mm) in both eyes. He had surgery in 1967 at age 5 years (Both eyes: recession IRM 6 mm, resection SRM 6 mm), in 1968 at age 6 years (Both eyes: recession MRM 5 mm, superior oblique tenotomy) and in 1969 at age 7 years (Both eyes: eyelid levator resection 14 mm by skin approach). Postoperative results showed mild ptosis in both eyes, and a consecutive exotropia (-10 prism dioptres) in the right eye.
Case III: 1 is a 21 year old man who was born with marked symmetric ptosis of 2nd degree, bilateral ophthalmoplegia with complete restriction of up-gaze, very marked restriction of down-gaze and exophoria-tropia OD. His corrected visual acuity was 6/20 (RE) and 6/8 (LE), and a simple hypermetropic astigmatism was present. His levator function was absent in both eyes. He had surgery in 1984 at age 5 years (both eyes: recession IRM 6 mm., conjunctival recession of 5 mm. LE: resection SRM 7 mm. RE: resection SRM 6 mm.) and 1986 at age 7 years (both eyes: suspension from frontalis muscle with autologous fascia lata). Postoperative results showed 1st degree ptosis and exophoria-tropia OD.
Case III: 2 is a 20 year old woman who was born with very marked symmetric ptosis (3rd degree), and bilateral ophthalmoplegia with complete restriction of up- and down-gaze. She had esotropia of + 25 prism dioptres and horizontal manifest-latent nystagmus. Her corrected visual acuity was 6/30 in both eyes and a simple myopic astigmatism was present. Her levator function was absent in both eyes. She had surgery in 1986 at age 6 years (both eyes: suspension from frontalis with autologous fascia lata, recession IRM 6 mm, recession of conjunctive 6 mm), in 1987 at age 7 years (RE : suspension from frontalis with autologous fascia lata, LE: recession MRM 8 mm) and in 1988 at age 8 years (both eyes: entropion correction). Postoperative results showed mild ptosis in both eyes (1st degrees), and the left eye showed consecutive exotropia (-10 prism dioptres).
Case III: 3 is a 15 year old girl who was born with very marked bilateral ptosis (3rd degree), and bilateral ophthalmoplegia with an inability to move her eyes above the midline. She had exotropia of -30 prism dioptres (V alphabetical pattern), corrected visual acuity of 6/8 in both eyes and hypermetropic astigmatism. Her levator function was sufficient (6 mm) in both eyes. She had surgery in 1989 at age 4 years (both eyes: levator resection 8 mm by conjunctival approach) and in 1996 at age 11 years (both eyes: recession IRM 5 mm, conjunctival recession 4 mm; RE: recession LRM 8 mm and up displacement LRM 5 mm; LE: recession LRM 5 mm and up displacement LRM 5 mm). Postoperative results showed 1st degree ptosis and exotropia was reduced from -30 to -5 prism dioptres in the RE.
Case III: 4 is a 13 year old girl who was born with very marked bilateral ptosis (3rd degree) and bilateral ophthalmoplegia with complete restriction of both up- and down-gaze. She had exotropia of -20 prism dioptres (V alphabetical pattern), corrected visual acuity of 6/30 in both eyes and a myopic astigmatism. Her levator function was absent in both eyes. She had surgery in 1995 at age 8 years (both eyes: resection SRM 8 mm) and in1997 at age 10 years (both eyes: suspension from frontalis with autologous fascia lata, recession LRM 4, up displacement LRM 6 mm). Postoperative results showed that ptosis was a slightly improved after surgery (2nd degree) only in the left eye, and strabismus was unchanged.
Case III: 5 is a 10 year old girl who was born with a very marked symmetric ptosis (3rd degree) and bilateral ophthalmoplegia with complete restriction of all eye movement. She had esotropia of +20 prism dioptres, corrected visual acuity of 6/8 in both eyes and a hypermetropic astigmatism. Her levator function was absent in both eyes. She had surgery in 1995 at age 4 years (both eyes: recession IRM and conjunctive), in 1996 at age 5 years (both eyes: resection RSM 6 mm) and in 1997 at age 6 years (both eyes: suspension from frontalis with autologous fascia lata; LE: Up transposition muscular belly MRM 7 mm; Up transposition muscular belly LRM 7 mm). Postoperative results showed 2nd degree ptosis in the right eye, but ptosis in the left eye and vertical and horizontal strabismus were unchanged.
Case III: 7 is an 8 year old boy who was born with a very marked symmetric ptosis (3rd degree), and bilateral ophthalmopegia with complete restriction of up- and down-gaze. He had exotropia of -30 prism dioptres, corrected visual acuity of 6/30 in both eyes and a hypermetropic astigmatism. His levator function was absent in both eyes. He had surgery in 1998 at age 6 years (both eyes: recession IRM 5 mm, recession of conjunctive and recession LRM 7 mm), in 1999 at age 7 years (both eyes: resection SRM 3 mm) and in 2000 at age 8 years (RE: resection MRM 6 mm). Postoperative results showed that a consecutive esotropia (+10 prism dioptres) was present in the left eye. The patient has not yet been operated for ptosis.
Case III: 8 is a two year old girl who was born with symmetric moderate ptosis (2nd degree) and ophthalmoplegia with complete restriction of up-gaze and moderate restriction of down-gaze. Her levator function was sufficient (6 mm). She has not yet had surgery.
Discussion
The surgical management performed on individuals with CFEOM in this study can be summarized as follows[40]: an Inferior Recti Muscles recession was generally performed (II:2, II:4, III:1, III:2, III:3, III:5, III:7). If this was not possible because of muscle contractures, surgery was performed directly on the Superior Recti Muscles (III:4).
The shallow inferior fornix was then corrected by means of a 4–5 mm conjuctival recession (III:1, III:2, III:3, III:5, III:7). Shortening of the inferior fornix, which is caused by the congenital downward rotation, is corrected by elevation of the eyeballs. This in turn corrected the anomalous head position. The elevation was then reinforced, whenever possible, by means of a SRM resection (II:2, II:4, III:1, III:4, III:5). If the SRM presented as a thin fibrous cord adhering to the sclera, surgery was not possible. If this was the case, to straighten the eye, the SRM was replaced with a portion of the superior oblique muscle which was resected and anchored to the sclera (III:7). If horizontal strabismus was present (esotropia or exotropia), surgery was performed on medial and lateral rectus muscles to reduce horizontal strabismus(II:2, II:4, III:2, III:3, III:4, III:5, III:7).
The type of surgery performed to correct ptosis depended on the level of the patient's eyelid levator function. The level of levator function in our patients was rated as sufficient, poor or absent. When the level of levator function was sufficient or poor (a measurement of approximately 4–5 mm), a resection of levator palpebrae by skin approach was done (II:2, II:4), or, in one case (III:3), with a levator function of approximately 6 mm, a resection of the levator palpebral by conjunctival approach was performed. When the levator function was absent (a measurement of < 4 mm), a suspension to the frontalis muscle was done (III:1, III:2, III:4, III:5).
Conclusions
Surgery on vertical muscles, associated with ptosis surgery, resulted in improvements in head position in all patients, with 3 of them (II 2, III 3 and III 7) achieving a normal head position. We obtained this result with a moderate amount of strabismus surgery for both vertical and horizontal deviation; we did not perform multiple supra-maximal surgeries and believe that different results achieved with different surgical approaches reflects mostly on the fact that CFEOM clinical features are variable.
On 14 operated eyes (7 patients) to correct ptosis, we had an improvement in 12 eyes, while 2 cases (III: 4 RE; III: 5 LE) exhibited no improvement. This is even when a suspension from frontalis by autologous fascia lata was performed. Careful attempts to avoid overcorrection of ptosis have prevented corneal exposure problems in all operated patients. The post-operative status of cornea is good in all operated patients. Even so, treatment with artificial tears in the form of hydroxymethylcellulose or polyvinylpyrrolidine alkaline eye drops and with simple ointement at night was recommended after ptosis surgery for six months in all patients.
In some cases (III:4, III:5), in spite of sugery performed on the vertical muscles and to correct ptosis, satisfactory results were not achieved. Unfortunately, this is a common outcome when these surgeries are performed on individuals with CFEOM and is related to the condition rather than any errors in how the surgeries were done. As the clinical features of the CFEOM are often variable, even in the same family, the surgical approach should be individualized to optimise success.
References
Baumgarten M: Erfahrungen uber den Strabismus und die Muskeldurchschneidung am Auge in physiologisch-pathologischer und therapeutischer Beziehung. Monatsschr Med Augenheilkd Chir. 1840, 3: 474-499.
Heuck G: Uber angeborenen verebten Beweglichkeitsdefekte der Augen. Klin Monatsbl Augeneilk. 1879, 17: 253-278.
Magli A, Greco GM, D'Esposito M: Genetica della oftalmoplegia congenita esterna. Atti LVIII Congresso SOI. Roma. 1977
Mollica F, Li Volti S, Incorpora G, Tita F, Tomarchio S, Moro F: Variabilité intrafamiliale de l'ophtalmoplegie externe congenitale. Etude d'une famille sicilienne. J Génét Hum. 1980, 28: 23-30.
Hiatt RL, Halle AA: General fibrosis syndrome. Ann Ophthalmol. 1983, 15: 1103-1109.
Abeloos MC, Cordonnier M, Van Nechel C, Van Bogaert P, Gérard JM, Van Regemoorter N: Fibrose Congénitale des muscles oculaires: un diagnostic pour plusieurs tableaux cliniques. Bull Soc Belge Ophtalmol. 1990, 239: 61-74.
Laughlin RC: Congenital fibrosis of the extraocular muscles. A report of six cases. Am J Ophthalmol. 1956, 41: 432-438.
McKusick VA: Mendelian inheritance in man: catalogs of autosomal dominant, autosomal recessive, and X-linked phenotypes. Baltimore: The Johns Hopkins University Press. 1990, 9
Engle EC, Kunkel LM, Specht LA, Beggs AH: Mapping a gene for congenital fibrosis of the extraocular muscles to the centromeric region of chromosome 12. Nat Genet. 1994, 7: 69-73.
Engle EC, Marondel I, Houtman WA, de Vries B, Loewenstein A, Lazar M, Ward DC, Kucherlapati R, Beggs AH: Congenital fibrosis of the extraocular muscles (autosomal dominant congenital external ophthalmoplegia): genetic homogeneity, linkage refinement, and physical mapping on chromosome 12. Am J Hum Genet. 1995, 57 (5): 1086-1094.
Engle EC, Goumnerov BC, McKeown CA, Schatz M, Johns DR, Porter JD, Beggs AH: Oculomotor nerve and muscle abnormalities in congenital fibrosis of the extraocular muscles. Ann Neurol. 1997, 41: 314-325.
Lees F: Congenital static familial ophthalmoplegia. J Neurol Neurosurg Psychiatry. 1960, 23: 46-51.
Catford GV: A familial musculo-fascial anomaly. Trans Ophtalmol Soc UK. 1966, 86: 19-36.
Cibis GW, Kies R, Lawwill T, Varghese G: Electromyography in congenital familial ophthalmoplegia. Strabismus. 1984, 2: 379-389.
Magli A, Santoro L, Perretti A, D'Esposito M, Caruso G: Electromyographic and enzymatic studies on families with external congenital ophthalmoplegia. Reprinted from Paediatric Ophthalmology. Edited by: Francois J, Maione M. 1982, John Wiley & Sons and Cortina Verona, 19: 371-374.
Black G, Perveen R, Hatchwell E, Reck A, Clayton-Smith J: Locus heterogeneity in autosomal dominant congenital external ophthalmoplegia. J Med Genet. 1998, 35 (12): 985-8.
Houtman WA, van Weerden TW, Robinson PH, de Vries B, Hoogenraad TU: Hereditary congenital external ophthalmoplegia. Ophthalmologica. 1986, 193: 207-218.
Engle EC: Applications of molecular genetics to the understanding of congenital ocular motility disorders. Ann N Y Acad Sci. 2002, 956: 55-63.
Engle E: The molecular basis of the congenital fibrosis syndromes. Strabismus. 2002, 10 (2): 125-128. 10.1076/stra.10.2.125.8142.
Lorenz B: Genetics of isolated and syndromic strabismus: facts and perspectives. Strabismus. 2002, 10 (2): 147-156. 10.1076/stra.10.2.147.8133.
Wang S, Zwaan J, Mullaney PB, Jabak MH, Al-Awad A, Beggs AH, Engle EC: Congenital fibrosis of the extraocular muscles type 2 (CFEOM2), an inherited exotropic strabismus fixus, maps to distal 11q13. Am J Hum Genet. 1998, 63: 517-525. 10.1086/301980.
Doherty E, Macy M, Wang S, Dykeman C, Melanson M, Engle E: CFEOM3: a new extraocular congenital fibrosis syndrome that maps to 16q24.2-q24.3. Invest Ophthalmol Vis Sci. 1999, 40 (8): 1687-1694.
Traboulsi E, Lee B, Mousawi A, Khamis A, Engle E: Evidence of genetic heterogeneity in autosomal recessive Congenital Fibrosis of the Extraocular Muscles (CFEOM). Am J Ophthalmol. 2000, 129: 658-662. 10.1016/S0002-9394(99)00467-5.
Nakano M, Yamada K, Fain J, Sener EC, Sellek CJ, Awad AH, Zwaan J, Mullaney PB, Bosley TM, Engle EC: Homozygous mutations in ARIX (PHOX2A) result in congenital fibrosis of the extraocular muscles type 2. Nat Genet. 2001, 29 (3): 315-20. 10.1038/ng744.
Sener EC, Lee BA, Turgut B, Akarsu AN, Engle EC: New clinical variation of a fibrosis syndrome in a Turkish family maps to the CFEOM1 locus on chromosome 12. Arch Ophthalmol. 2000, 118 (8): 1090-1097.
D'Esposito F, Magli A, de Berardinis T, Bhattacharya SS: Oftalmoplegia congenita esterna: conferma della presenza di un locus genetico sul cromosoma 12. IX Meeting of the International Society for Genetic Eye Diseases, Siena. 1992
Engle Ec, McIntosh N, Yamada K, Lee BA, Johnson R, O'Keefe M, Letson R, London A, Ballard E, Ruttum M, Matsumoto N, Saito N, Collins M, Morris L, Monte M, Magli A, de Berardinis T: CFEOM 1, the classic familial form of congenital fibrosis of the extraocular muscles, is genetically heterogeneous but does not result from mutations in ARIX. BMC Genet. 2002, 3 (1): 3-10.1186/1471-2156-3-3.
Venkatesh CP, Pillai VS, Raghunath A, Prakash VS, Vathsala R, Pericak-Vance MA, Kumar A: Clinical phenotype and linkage analysis of the congenital fibrosis of the extraocular muscles in an Indian family. Mol Vis. 2002, 8: 294-297.
Hotchkiss MG, Miller NR, Clark AW, Green WG: Bilateral Duane's retraction syndrome: A clinical-pathological case report. Arch Ophthalmol. 1980, 98: 870-874.
Miller NR, Kiel SM, Green WR, Clark AW: Unilateral Duane's retraction syndrome (type 1). Arch Ophthalmol. 1982, 100: 1468-1472.
Gottlob I, Jain S, Engle E: Elevation of one eye during tooth brushing. Am J Ophthalmol. 2002, 134 (3): 459-10.1016/S0002-9394(02)01540-4.
Traboulsi EI, Jaafar MS, Kattan H, Parks MM: Congenital fibrosis of the extraocular muscles: Report of 24 cases illustrating the clinical spectrum and surgical management. Am Orthop J. 1993, 43: 45-53.
Apt L, Axelord RN: Generalized fibrosis of the extraocular muscles. Am J Ophtalmol. 1978, 85: 822-829.
Boergen P: Proceedings of 18th European Strabismological Association, ed. Kaufman. 1989, 55-59.
Ferrer JA: General Fibrosis Syndrome. Second Congress of the International Strabismological Association. Paris: Diffus Générale de Librairie. 1976, 352-361.
Ferrer JA: Letters to Editor:Congenital Fibrosis of the Extraocular Muscles. Ophthalmology. 1996, 63 (10): 1517-1518.
Hertle WH, Katowitz JA, Young TL, Quinn GE, Farber MG: Congenital unilateral fibrosis, blepharoptosis, and enophthalmos syndrome. Ophthalmology. 1992, 99 (3): 347-355.
Kanski JJ: Oftalmologia clinica. USES Edizioni Scientifiche Firenze. 1989, 20-21.
Magli A, de Berardinis T, Gagliardi V, Pignalosa G: Classificazione, valutazione e trattamento delle blefaroptosi in età pediatrica. Boll Ocul. 1998, 77 (suppl 4): 183-193.
D'Esposito M, Bonavolontà G, Magli A, Aurilia P: Ptosis correction in the context of the treatment of external congenital ophthalmoplegia. Ophthalmic Plast Reconstr Surg. 1989, 5 (3): 176-181.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2415/3/6/prepub
Acknowledgements
We thank the family members for their kind cooperation and Dr E.C. Engle for critical advice. Special thanks to Ms. N. McIntosh for critical review and for translation of the manuscript.
Written consent was obtained from the patient or their relative for publication of the patient's details.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Magli, A., de Berardinis, T., D'Esposito, F. et al. Clinical and surgical data of affected members of a classic CFEOM 1 family. BMC Ophthalmol 3, 6 (2003). https://doi.org/10.1186/1471-2415-3-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2415-3-6