
Abstract
Background
Mutations in PEX1 are the most common primary cause of Zellweger syndrome. In addition to exonic mutations, deletions and splice site mutations two 5' polymorphisms at c.-137 and c.-53 with a potential influence on PEX1 protein levels have been described in the 5' untranslated region (UTR) of the PEX1 gene.
Methods
We used RACE and in silico promoter prediction analysis to study the 5' UTR of PEX1. We determined the distribution of PEX1 5' polymorphisms in a cohort of 30 Zellweger syndrome patients by standard DNA sequencing. 5' polymorphisms were analysed in relation to the two most common mutations in PEX1 and were incorporated into a novel genotype-phenotype analysis by correlation of three classes of PEX1 mutations with patient survival.
Results
We provide evidence that the polymorphism 137 bp upstream of the ATG codon is not part of the UTR, rendering it a promoter polymorphism. We show that the first, but not the second most common PEX1 mutation arose independently of a specific upstream polymorphic constellation. By genotype-phenotype analysis we identified patients with identical exonic mutation and identical 5' polymorphisms, but strongly differing survival.
Conclusions
Our study suggests that two different types of PEX1 5' polymorphisms have to be distinguished: a 5' UTR polymorphism at position c.-53 and a promoter polymorphism 137 bp upstream of the PEX1 start codon. Our results indicate that the exonic PEX1 mutation correlates with patient survival, but the two 5' polymorphisms analysed in this study do not have to be considered for diagnostic and/or prognostic purposes.
Similar content being viewed by others


Background
Peroxisome biogenesis disorders (PBD, MIM #601539) are a group of autosomal recessive diseases characterized by a severe developmental and metabolic phenotype [1]. PBD comprise the Zellweger syndrome (ZS) spectrum and rhizomelic chondrodysplasia punctata. The ZS spectrum consists of three overlapping clinical phenotypes representing a continuum of disorders, ranging form infantile Refsum disease (IRD, MIM #266510) as the mildest variant, to neonatal adrenoleukodystrophy (NALD, #MIM 202370) and to ZS (MIM #214100) as the prototype and most severe form with a life expectancy of less than one year. ZS patients often show characteristic dysmorphic features and severe neurodevelopmental brain abnormalities like polymicrogyria and pachygyria. Clinically patients present with muscular hypotonia and poor feeding, seizures, eye abnormalities, liver dysfunction and skeletal defects.
ZS is caused by mutations in PEX genes, encoding proteins (peroxins) required for the biogenesis of peroxisomes [1, 2]. Peroxisomes are ubiquitous cellular organelles with functions in ether lipid biosynthesis, α-oxidation of phytanic acid, β-oxidation of very long chain fatty acids (VLCFAs) and of bile acid precursors and docosahexaenoic acid (DHA) precursors, and in hydrogen peroxide metabolism [3]. Peroxisomes are versatile organelles which can be induced and regulated according to metabolic needs [4]. In humans, 16 evolutionarily conserved peroxins are known, mutations in 13 of which are associated with disease. The peroxins PEX5 and PEX7 are cytosol-based import receptors for peroxisomal matrix proteins. The import receptor PEX5 loaded with matrix proteins can associate with most peroxisomal proteins in the cytosol and is involved in the translocation of these proteins into the peroxisome. According to one model, a downstream complex of two ATPases, PEX1 and PEX6, and the peroxisomal membrane protein PEX26 are thought to mediate recycling of PEX5 into the cytosol [5, 6]. This process depends on ubiquitination of PEX5 during the translocation process at the peroxisomal membrane. Models of peroxisome protein import have been reviewed recently [7, 8].
PEX1 and the paralogous PEX6 gene encode members of the AAA (ATPases associated with diverse cellular activities) family of proteins. PEX1 and PEX6 comprise two AAA domains. The PEX1 gene spans about 41.5 Mbp and is composed of 24 exons, encoding an mRNA of 4.4 kbp. Mutations in PEX1 are the most common primary cause of Zellweger syndrome and account for roughly two thirds of all PBD patients [9–14]. The most commonly found mutation in PEX1 is c.2528G > A leading to an exchange of Gly to Asp in the PEX1 protein [15–17]. The second most frequent mutation is the insertion 2097_2098insT leading to a frameshift and nonsense mutation after I700 [9, 18]. These common PEX1 mutations have been included in genotype phenotype analyses showing that the missense mutation is associated with the mild end of the clinical spectrum and the insertion with more severly affected patients [1]. This correlation proves true in the majority of cases, but exceptions can be observed in which same genetic constellation leads to largely divergent phenotypes. Such cases make it necessary to look for potential effects that modulate patient outcome on the basis of a given primary defect. More recently, two polymorphisms have been described upstream the PEX1 coding region. One is a C-to-G transversion located 53 nucleotides upstream the PEX1 ATG (c.-53C > G). The other is a T-to-C transition, c.-137T > C. The c.-137 T > C polymorphism resides in a potential in-frame ATG codon that could expand the PEX1 ORF by 138 bp. This ATG, however, could be shown not to represent a translational start codon [19]. Reporter studies by Maxwell et al. suggest that the -137C polymorphism results in reduced expression of PEX1 whereas the -53G polymorphism increases expression of PEX1 [19]. A combination of both polymorphisms results in near-normal expression of PEX1 in a reporter experiment [19]. Polymorphisms modulating the PEX1 protein level could possibly modulate the disease phenotype of PEX1 patients. An analysis of polymorphisms and PEX1 mutations in 25 PEX1-deficient patients suggested that the c.-137T > C transition cosegregates with the c.-53C > G transversion. In addition, both polymorphisms were found to cosegregate with the 2097_2098insT mutation [19].
To evaluate the potential influence of known 5' polymorphisms in PEX1 on the disease phenotype we analysed the 5' UTR in more detail. We provide evidence that the -137C polymorphism is not a 5' UTR but rather a promoter polymorphism. We included both polymorphisms in a genotype-phenotype analysis of 30 PBD patients with PEX1 mutations representing the whole spectrum of clinical phenotypes.
Methods
Collection of patients
5'UTR polymorphisms of 30 patients with mutations in the PEX1 gene were analyzed. The patients had been referred to the Department of Pediatrics and Pediatric Neurology at the University of Göttingen for diagnostic evaluation of peroxisome biogenesis disorder and through the German LEUKONET. Informed consent has been obtained from guardians of all patients. The work presented in this study was conducted under the approval of the local ethics committee. The clinical phenotype and plasma biochemical abnormalities pointed towards a peroxisome biogenesis disorder and PEX1 gene mutations were identified by direct sequencing. PEX1 mutations of this patient cohort are previously published in part [12]. In some instances PEX1 deficiency was further confirmed by complementation analysis [14].
Extraction of genomic DNA from fibroblasts and blood
Genomic DNA was extracted from 107 cells. After trypsinization, cells were washed in PBS, resuspended in 800 μl lysis buffer (50 mM Tris-HCl, pH 8.0, 100 mM EDTA, 0.5% SDS) and treated with 50 μg proteinase K for 16 hrs at 55°C. DNA was extracted by a standard protocol using phenol-chloroform. Genomic DNA from blood was extracted using the DNeasy Blood&Tissue Kit (Qiagen, Hilden, Germany) following the instructions of the manufacturer.
RNA extraction and cDNA-Synthesis (Reverse Transcription)
RNA was extracted from fibroblasts using peqGOLD TriFast (Peqlab, Erlangen, Germany). For first strand synthesis we used the SuperScriptIII First-Strand Synthesis System (Invitrogen, Darmstadt, Germany) with 1 μg total RNA together with Oligo(dT20) primers according to the specification of the manufacturer.
Determination of polymorphisms and haplotype analysis
Single nucleotide polymorphisms at c.-53 C > G und c.-137 T > C in the PEX1 gene, and exonic mutations were analysed by sequencing after PCR amplification using the primers listed in the table in additional file 1. PCR reactions were performed in a Thermocycler T3000 (Biometra, Göttingen, Germany) and analysed on 1% agarose gels. All PCR products were purified using the High Pure PCR Purification Kit (Roche, Grenzach-Wyhlen, Germany) following the instructions of the manufacturer. For DNA sequencing the BigDyeTerminator v3.1 Cycle Sequencing kit (Applied Biosystems, Darmstadt, Germany) was used. Sequencing reactions were purified by DNA precipitation, dissolved in 10 μl Hi-Di formamid (Applied Biosystems) and analysed on a 3100-Avant Genetic Analyzer (Applied Biosystems). Abi Prism 3100 Genetic Analyzer Data Collection Software 2.0 (Applied Biosystems) and Laser Gene Sequencing Analysis Software 5.1. (Dnastar, Madison, WI, USA) were used for sequence analysis.
Rapid amplification of cDNA ends (RACE)
The 5'/3' RACE Kit (Roche) was used to characterize the transcriptional start of the PEX1 mRNA following the manufacturer's protocol. Briefly, PEX1 specific reverse primers (SP1, SP2, SP3, respectively) and Reverse Transcriptase were used to synthesize cDNA extending to the 5' end of the PEX1 mRNA. The 3' end of the resulting cDNA was polyadenylated using Terminal Transferase. The resulting cDNA was PCR amplified using internal PEX1 specific primers (SP2, Pex1ex2, SP1, respectively), and an oligo-dT anchor primer. This step was followed by a nested PCR (primers Pec10 or SP2, respectively, and the anchor primer). PCR products were directly cloned into pGEM-T-Easy Vectors I (Promega, Mannheim, Germany) and sequenced using the T7 and SP6 sites of the vector. For primer sequences see table in additional file 1.
Results and Discussion
Definition of the PEX15'UTR
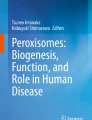
Both 5' polymorphisms, c.-137 T > C and c.-53 C > G, have been described as 5 'UTR polymorphisms implying they become part of the mRNA. The PEX1 5'UTR was reported to extend up to c.-245 according to PCR amplification studies [19]. In PCRs with cDNA prepared from cultivated primary human fibroblasts, however, we could not amplify cDNA with primers upstream of or including c.-137 (primers 455H, 455K, 455I, and OST542 in Figure 1). Our analysis also included the primer used in a previous study [19], here designated OST542 (Figure 1). In contrast, all primers downstream of c.-137 (primers 455C, 455, 455G, 455E, 455F) could amplify the PEX1 cDNA. The most upstream functional primer extended up to c.-123 suggesting that the polymorphism at c.-137 is not necessarily part of the mRNA. Identification of the PEX1 transcriptional start is of importance because a transcriptional start at around c.-123 would render the upstream polymorphism at c.-137 a promotor polymorphism. For comparison, a database entry marked c.-96 as the PEX1 mRNA start (NCBI Reference Sequence NM_000466.2). To experimentally confirm the transcriptional start point of PEX1, we conducted a 5'RACE (rapid amplification of cDNA ends) experiment. The 5' region of PEX1 mRNA was reverse transcribed using a gene-specific internal primer, PCR amplified in two successive rounds and cloned into a pGEM-T vector for sequencing. The longest 5' extension of the cDNA that could be identified by this approach extended to c.-120, giving no further indication that the 5' UTR of PEX1 stretches as far as c.-245. To gain further insight into the PEX1 5'UTR/promotor region, we searched the 500 bp upstream of the ATG for putative transcription factor binding sites using the weight matrix-based Match tool within the TRANSFAC database [20, 21]. Results are summarized in the table in additional file 2. This analysis shows that the region upstream c.-100 is covered by GC box elements that are bound by one of the classical upstream transcription factors, Sp1 [22], also arguing against a transcriptional start at c.-245.

Analysis of the 5' region of PEX1. Schematic representation of the PEX1 5' region. Positions c.-137, c.-53 and the start codon are marked. Primers that in combination with the reverse primer Pec10 or PEX1- Ex 2 (Exon 2) give PCR products are marked in light gray (cDNA template). Primers that do not yield PCR products are marked in dark gray. In our analysis only primers downstream of c.-137 could be used to amplify sequences from PEX1 cDNA. These results were confirmed by RACE.
In summary, PCR and RACE experiments, PEX1 cDNA database entries and a promoter analysis indicate that the PEX1 polymorphism at c.-137 is not necessarily a polymorphic site in the 5' UTR but could also be a polymorphism within the promoter. It is of interest that 242 bp upstream of the PEX1 start codon, the poorly characterized ORF C7orf64 starts, extending on the other DNA strand. Thus the PEX1 5' region, previously defined as UTR [19] coincides with the intergenic regions between PEX1 and C7orf64 and would comprise UTRs of both genes.
5' Polymorphisms in a PEX1 patient population
PEX1 upstream polymorphisms bear the potential to modulate the disease phenotype due to their influence on PEX1 expression levels. We assessed the presence or absence of the two known 5' polymorphisms at c.-137 and c.-53 in a well-characterized PBD patient collection with PEX1 mutations [12]. PEX1 mutations in this patient collection are deletions (11 out of 60 alleles), insertions (12/60), and point mutations (34/60). In three patients, only one affected allele has been identified so far (Table 1). The two most common mutations are the missense mutation c.2528 G > A in exon 15 (22 out of 60 alleles) resulting in an amino acid exchange of glycine to aspartate (p.Gly843Asp or G843D), and the insertion c.2097_2098insT in exon 13 (10/60 alleles) leading to a frameshift after isoleucin in position 700 and a premature termination codon (PTC). Altogether, 20 of the 60 alleles include PTCs, leading to potentially more severe phenotypes. Four constellations of the 5' polymorphisms were identified in the patient collective of 30 patients. We found the common constellation (c.-137 TT and c.-53 CC) in 13 (43%) of the patients and, likewise 11 (37%) heterozygous carriers (c.-137 TC and c.-53 GC). The 5' polymorphism at c.-137 alone in combination with a wild-type allele at c.-53 (c.-137 TC and c.-53 CC) appeared in three (10%) of the PEX1 patients. Another three (10%) were homozygous for both polymorphisms (c.-137 CC and c.-53 GG). The three patients with a c.-137T > C transition without the c.-53C > G transversion indicated that the c.-137T > C transition can be present in the absence of the c.-53C > G transversion. This constellation was not present in the patient cohort analysed by Maxwell and colleagues [19]. On the background of this polymorphism constellation PEX1 expression could potentially be reduced to a stronger extent than caused by the patients' PEX1 mutations alone. The polymorphic constellations identified in this study (TT CC, TC GG, CC GG, and TC CC) are four of a total of nine possible constellations. These four constelations can be explained by existence of only three alleles: -137C -53G, -137T -53C, and the rare -137C -53C. This would be the most parsimonious, but still speculative interpretation.
In sum, the allele frequency of the c.-137T > C polymorphism in our patient cohort was 33% (20/60), compared to 14.9% in the European population (NCBI single nucleotide polymorphism (SNP) database). Interestingly, the allele frequency of the c.-53C > G polymorphism was 28% (17/60) in our cohort, whereas in the healthy population it is reported to range between 4.4 and 7.8% (NCBI SNP database).
We next analysed the distribution of PEX1 5' polymorphisms in relation to the two most common PEX1 mutations. Table 2 shows the distribution of 5' polymorphisms in relation to c.2097_2098insT. Of eleven heterozygous patients (c.-137 TC and c.-53 GC), six were heterozygous for the insertion c.2097_2098insT. The remaining five patients did not carry the insertion. The three patients with the heterozygous polymorphism only at position c.-137 (c.-137 TC and c.-53 CC) did not carry the c.2097_2098insT insertion and both homozygous patients (c.-137 CC and c.-53 GG) were homozygous for c.2097_2098insT. None of our patients with a wild-type configuration at both polymorphism sites (c.-137 TT und c.-53 CC) carries the c.2097_2098insT insertions. We could thus confirm that the second most common PEX1 allele, 2097_2098insT, is coupled to the c.-137 T > C c.-53 C > G constellation and probably evolved on the basis of this allele (Table 2). The evolution of the 2097_2098insT allele on the basis of the c.-137 T > C c.-53 C > G constellation also explains the overrepresentation of the c.-53C > G polymorphism in our cohort.
Table 3 shows the distribution of these polymorphisms in relation to the most common PEX1 mutation, p.Gly843Asp. The 13 patients with the common sequence at positions c.-137 and c.-53 and the 11 patients with the two heterozygous 5' polymorphisms distributed equally in relation to the p.Gly843Asp mutation. One heterozygous p.Gly843Asp patient was found to carry the rare homozygous c.-137 CC c.-53 GG constellation. This indicated that the p.Gly843Asp allele can be found in combination with any of the four possible 5' alleles and that the p.Gly843Asp mutation and the 5' polymorphisms evolved independently of each other.
Tables 2 and 3 also indicate the expected effect of the polymorphisms on PEX1 gene expression levels following the analysis of Maxwell et al. [19]. It was found that c.-137 T > C polymorphism decreased the PEX1 gene expression by 50% (↓), whereas the c.-53 C > G polymorphism increased PEX1 expression by approximately 25% (↑) when analyzed in a luciferase reporter study [19]. A combination of both 5' polymorphisms did not lead to a significant change in PEX1 gene expression. To evaluate a possible effect of PEX1 5' polymorphisms on the severity of the patient phenotype we included the 5' polymorphisms in a genotype-phenotype analysis.
Genotype-Phenotype-Correlation
With respect to the common exonic PEX1 mutations, a genotype-phenotype correlation has been described [9, 12, 23, 24]. Generally, PEX1 alleles that lead to a PTC (P), caused by frameshift or nonsense mutations, lead to more severe phenotypes than alleles with a missense mutation (M). It is thus possible to classify patients in three groups, depending on the combinations of PTC and M: MM (type 1), PM (type 2), PP (type 3). In order to limit the genotypic classes to three, we included the patients with short insertions that do not result in PTC in the type 1 group and the more extensive deletions together with other deletions resulting in PTCs in the PTC group. We undertook this analysis with our patient cohort and plotted the time of survival as a measure of phenotypic severity on the y-axis (Figure 2).

Genotype-Phenotype-Correlation in PEX1 patients with known survival. Patients were grouped according to their genotypes into patients with missense mutations (M) on both alleles (type 1, MM), with premature termination codons (PTCs, P) on both alleles (type 3, PP), or with a combination of a PTC with a missense mutation (type 2, MP). To limit the genotypic classes to three, we grouped short insertions that do not result in PTC together with M, and more extensive deletions together with the P alleles. 5' polymorphisms are marked in color. Numbers in circles refer to ZS patient numbers as in Table 1. Patients with survival of more than 100 months were alive at the time of submission of the manuscript.
This representation confirms that the type 3 genotype results in the most severe phenotype with an average survival of only 4.7 months (six patients). This group also includes patient ZS01 with a homozygous deletion of 115 amino acids. The average survival in the patient group with a combination of a missense mutation and a PTC (type 2) is 50.8 months (eight patients). This group also includes patient ZS19 with a three-base pair insertion in combination with the common p.Ile700TyrfsX42 mutation. Patients with missense mutations on both PEX1 copies (type 1) show the longest survival, 106 months on average (eight patients). The patient group generally associated with the longest survival can be divided into two groups of survival of less than 40 months or 8.2 months on average (four patients) and more than 170 months, or 203 months on average (Figure 2). It has to be noted that patients with a survival of more than 100 months were alive at the time of the submission of this manuscript, so the longer survival rates can be prognostically used as a lower limit only.
We also indicated the 5' polymorphisms within each of these groups and found that all but one patient of known survival in the type 1 group have the common 5' genotype c.-137 TT c.-53 CC. This means that the differentiation in survival in the type 1 group is not due to differences in the known 5' polymorphisms, and, more generally, that differences in 5' polymorphisms are not the cause for the different survival of patients with the same mutations in PEX1. On the other side, conclusions that can be drawn from this analysis are limited by the absence of a pair of patients with functionally different 5' polymorphisms and with the same exonic genotype. Extreme differences in survival of patients with identical exonic mutations and 5' polymorphisms suggest, however, that these differences cannot be attributed to the 5' polymorphisms.
Conclusions
Our study suggests that only the PEX1 5' polymorphic site at c.-53 is part of the 5' UTR while the polymorphism 137 bp upstream of the PEX1 start codon might be part of the PEX1 promoter. The common c.2528G > A (p.Gly843Asp) mutation appears to be independent of a specific upstream polymorphism in contrast to the second most common mutation, c.2097_2098insT (p.Ile700TyrfsX42), that arose on the basis of the -137 T > C c.-53 C > G polymorphic constellation. A novel genotype-phenotype representation with only three genetic categories allows distinguishing groups of largely differing patient survival, but 5' polymorphisms do not seem to further modulate patient survival. We could not yet, however, identify patients with identical PEX1 mutations and functionally different 5' polymorphisms.
References
Weller S, Gould SJ, Valle D: Peroxisome biogenesis disorders. Annu Rev Genomics Hum Genet. 2003, 4: 165-211. 10.1146/annurev.genom.4.070802.110424.
Ebberink MS, Mooijer PA, Gootjes J, Koster J, Wanders RJ, Waterham HR: Genetic classification and mutational spectrum of more than 600 patients with a Zellweger syndrome spectrum disorder. Hum Mutat. 2011, 32: 59-69. 10.1002/humu.21388.
Wanders RJ, Waterham HR: Biochemistry of mammalian peroxisomes revisited. Annu Rev Biochem. 2006, 75: 295-332. 10.1146/annurev.biochem.74.082803.133329.
Thoms S, Erdmann R: Dynamin-related proteins and Pex11 proteins in peroxisome division and proliferation. Febs J. 2005, 272: 5169-5181. 10.1111/j.1742-4658.2005.04939.x.
Weller S, Cajigas I, Morrell J, Obie C, Steel G, Gould SJ, Valle D: Alternative splicing suggests extended function of PEX26 in peroxisome biogenesis. Am J Hum Genet. 2005, 76: 987-1007. 10.1086/430637.
Thoms S, Erdmann R: Peroxisomal matrix protein receptor ubiquitination and recycling. Biochim Biophys Acta. 2006, 1763: 1620-1628. 10.1016/j.bbamcr.2006.08.046.
Grou CP, Carvalho AF, Pinto MP, Alencastre IS, Rodrigues TA, Freitas MO, Francisco T, Sa-Miranda C, Azevedo JE: The peroxisomal protein import machinery--a case report of transient ubiquitination with a new flavor. Cell Mol Life Sci. 2009, 66: 254-262. 10.1007/s00018-008-8415-5.
Baker A, Sparkes IA, Brown LA, O'Leary-Steele C, Warriner SL: Peroxisome biogenesis and positioning. Biochem Soc Trans. 2010, 38: 807-816. 10.1042/BST0380807.
Preuss N, Brosius U, Biermanns M, Muntau AC, Conzelmann E, Gartner J: PEX1 mutations in complementation group 1 of Zellweger spectrum patients correlate with severity of disease. Pediatr Res. 2002, 51: 706-714.
Gartner J, Preuss N, Brosius U, Biermanns M: Mutations in PEX1 in peroxisome biogenesis disorders: G843D and a mild clinical phenotype. J Inherit Metab Dis. 1999, 22: 311-313. 10.1023/A:1005599903632.
Yik WY, Steinberg SJ, Moser AB, Moser HW, Hacia JG: Identification of novel mutations and sequence variation in the Zellweger syndrome spectrum of peroxisome biogenesis disorders. Hum Mutat. 2009, 30: E467-480. 10.1002/humu.20932.
Rosewich H, Ohlenbusch A, Gartner J: Genetic and clinical aspects of Zellweger spectrum patients with PEX1 mutations. J Med Genet. 2005, 42: e58-10.1136/jmg.2005.033324.
Crane DI, Maxwell MA, Paton BC: PEX1 mutations in the Zellweger spectrum of the peroxisome biogenesis disorders. Hum Mutat. 2005, 26: 167-175. 10.1002/humu.20211.
Krause C, Rosewich H, Gartner J: Rational diagnostic strategy for Zellweger syndrome spectrum patients. Eur J Hum Genet. 2009, 17: 741-748. 10.1038/ejhg.2008.252.
Tamura S, Okumoto K, Toyama R, Shimozawa N, Tsukamoto T, Suzuki Y, Osumi T, Kondo N, Fujiki Y: Human PEX1 cloned by functional complementation on a CHO cell mutant is responsible for peroxisome-deficient Zellweger syndrome of complementation group I. Proc Natl Acad Sci USA. 1998, 95: 4350-4355. 10.1073/pnas.95.8.4350.
Portsteffen H, Beyer A, Becker E, Epplen C, Pawlak A, Kunau WH, Dodt G: Human PEX1 is mutated in complementation group 1 of the peroxisome biogenesis disorders. Nat Genet. 1997, 17: 449-452. 10.1038/ng1297-449.
Reuber BE, Germain-Lee E, Collins CS, Morrell JC, Ameritunga R, Moser HW, Valle D, Gould SJ: Mutations in PEX1 are the most common cause of peroxisome biogenesis disorders. Nat Genet. 1997, 17: 445-448. 10.1038/ng1297-445.
Walter C, Gootjes J, Mooijer PA, Portsteffen H, Klein C, Waterham HR, Barth PG, Epplen JT, Kunau WH, Wanders RJ, Dodt G: Disorders of peroxisome biogenesis due to mutations in PEX1: phenotypes and PEX1 protein levels. Am J Hum Genet. 2001, 69: 35-48. 10.1086/321265.
Maxwell MA, Leane PB, Paton BC, Crane DI: Novel PEX1 coding mutations and 5' UTR regulatory polymorphisms. Hum Mutat. 2005, 26: 279-
Matys V, Fricke E, Geffers R, Gossling E, Haubrock M, Hehl R, Hornischer K, Karas D, Kel AE, Kel-Margoulis OV, Kloos DU, Land S, Lewicki-Potapov B, Michael H, Munch R, Reuter I, Rotert S, Saxel H, Scheer M, Thiele S, Wingender E: TRANSFAC: transcriptional regulation, from patterns to profiles. Nucleic Acids Res. 2003, 31: 374-378. 10.1093/nar/gkg108.
Wingender E, Chen X, Hehl R, Karas H, Liebich I, Matys V, Meinhardt T, Pruss M, Reuter I, Schacherer F: TRANSFAC: an integrated system for gene expression regulation. Nucleic Acids Res. 2000, 28: 316-319. 10.1093/nar/28.1.316.
Briggs MR, Kadonaga JT, Bell SP, Tjian R: Purification and biochemical characterization of the promoter-specific transcription factor, Sp1. Science. 1986, 234: 47-52. 10.1126/science.3529394.
Maxwell MA, Allen T, Solly PB, Svingen T, Paton BC, Crane DI: Novel PEX1 mutations and genotype-phenotype correlations in Australasian peroxisome biogenesis disorder patients. Hum Mutat. 2002, 20: 342-351. 10.1002/humu.10128.
Tamura S, Matsumoto N, Imamura A, Shimozawa N, Suzuki Y, Kondo N, Fujiki Y: Phenotype-genotype relationships in peroxisome biogenesis disorders of PEX1-defective complementation group 1 are defined by Pex1p-Pex6p interaction. Biochem J. 2001, 357: 417-426. 10.1042/0264-6021:3570417.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2350/12/109/prepub
Acknowledgements and Funding
We thank Birgit Zirn for helpful discussion and Jens Kaiser for help with the RACE experiments. This project was supported by grants from the BMBF (German LEUKONET) and the Deutsche Forschungsgemeinschaft (GA354/7-1).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
ST, SG and JG conceived the study. ST and SG analysed the data, and wrote the manuscript. JR and AO carried out the molecular genetic studies and analyzed the data. ST and JR prepared tables and figures. ST, SG and JG supervised JR. HR provided patient genotypes and analysed the clinical data including patient survival information. All authors read and approved the final manuscript.
Sven Thoms, Sabine Grønborg contributed equally to this work.
Electronic supplementary material
12881_2011_841_MOESM1_ESM.PDF
Additional file 1: Primers used in this study. Table with list of oligonucleotide primers used in this study. (PDF 11 KB)
12881_2011_841_MOESM2_ESM.PDF
Additional file 2: Transcription factor binding sites in the PEX1 5' upstream region from c.-500 to c.-1. Table with results of an in silico analysis of transcription factor binding sites in the PEX1 5' region. (PDF 11 KB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Thoms, S., Grønborg, S., Rabenau, J. et al. Characterization of two common 5' polymorphisms in PEX1 and correlation to survival in PEX1 peroxisome biogenesis disorder patients. BMC Med Genet 12, 109 (2011). https://doi.org/10.1186/1471-2350-12-109
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2350-12-109