
Abstract
Background
There are two widely used transient middle cerebral artery occlusion (MCAO) methods, which differ in the use of unilateral or bilateral carotid artery reperfusion (UNICAR and BICAR). Of the two methods, UNICAR is easier to perform. This study was designed to comprehensively compare the two reperfusion methods to determine if there are any differences in outcomes.
Results
The UNICAR and BICAR groups each included 9 rats. At baseline, the average pO2 was 20.54 ± 9.35 and 26.43 ± 7.39, for the UNICAR and BICAR groups, respectively (P = 0.519). Changes in pO2, as well as other physiological parameters measured within the ischemic lesion, were similar between the UNICAR and BICAR groups during 90 min of MCAO and the first 30 min of reperfusion (all P > 0.05). Furthermore, both the Bederson score and Garcia score, which are used for neurological assessment, were also similar (both P > 0.05). There were also no significant differences in T2WI lesion volume, DWI lesion volume, PWI lesion volume, or TTC staining infarct volume between the two groups (all P > 0.05).
Conclusion
UNICAR and BICAR have similar capability for inducing acute brain ischemic injury and can be considered interchangeable up to 24 hours after reperfusion.
Similar content being viewed by others


Background
The transient middle cerebral artery occlusion (MCAO) stroke model has been widely used to study the effects of cerebral ischemia (for review see [1]). Furthermore, there have been many studies on transient MCAO, demonstrating that rat strain [2], animal age [3], ischemia duration [4], and suture type [5] contribute to variability of outcomes. However, we are unaware of any research comparing differences in reperfusion techniques.
There are two basic reperfusion methods (return of blood flow) in models of transient MCAO. In the bilateral carotid artery reperfusion (BICAR) method, the common carotid artery (CCA) is temporarily occluded; a filament is put through an opening cut in the external carotid artery (ECA) and then pushed through the internal carotid artery (ICA) to occlude the middle cerebral artery (MCA). Prior to reperfusion, the filament is pulled out from the ECA, which remains occluded while the CCA and ICA are reopened. This method results in the brain being reperfused by both carotid arteries. In the unilateral carotid artery reperfusion (UNICAR) method, the CCA and ECA are permanently ligated and the filament is pushed through the opening of the CCA distal to the ligation point and then threaded up into the ICA to occlude the MCA. Before reperfusion, the filament is withdrawn while the CCA and ECA are still occluded; as a result, only the carotid artery contralateral to the ischemic hemisphere reperfuses the brain.
The primary difference between the UNICAR and BICAR methods is the complexity of the procedure. In our experience, UNICAR is easier to perform since it does not require separating the ECA prior to MCAO, reopening the CCA, and ligating the nub of the ECA before inducing reperfusion. This increases the possibility of damaging the soft tissues and cranial nerves leading to difficulty in food and water intake, which can confound the results of the study. Furthermore, as the CCA is thicker and straighter than the ECA, it is easier to cut as well as insert the suture.
We hypothesize that BICAR results in more abundant blood supply to the ischemic brain tissue, thereby leading to better locomotor and histological outcomes than UNICAR. To test this hypothesis we compared both reperfusion methods in regards to cerebral blood flow (CBF) and partial oxygen pressure (pO2) within the ischemic brain tissue during MCAO/reperfusion. We also studied infarct volume at 24 h after reperfusion by using comprehensive modalities including histological assessment and magnetic resonance imaging (MRI) including T2-weighted MRI (T2WI), diffusion-weighted MRI (DWI) and perfusion-weighted MRI (PWI). In addition neurological deficits were analyzed using two well-established neurological grading systems.
Methods
Transient MCAO models
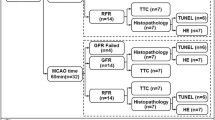
All animal experiments were performed according to the German laws for animal protection and the National Institutes of Health guidelines for the use and care of laboratory animals (all experiments were approved by the Ministerium fuer Landwirtschaft, Umwelt und Ländliche Räume des Landes Schleswig-Holstein, Kiel, Germany). Male Sprague–Dawley rats (Charles River, Germany) weighing 200–250 g and aged 6–8 weeks were provided with food and water ad libitum and housed in a 12:12-h light/dark cycle at 24°C with appropriate humidity. Rats were fasted for one night before the MCAO procedure. Body temperature was maintained at 37.0 ± 0.5°C with a heating pad during all procedures. Chloral hydrate (400 mg/kg body weight) injected intraperitoneally was used as anesthetic for all surgical procedures [6]. The rats were randomized to the UNICAR group (n = 15) and BICAR group (n = 15). For the UNICAR group, an intraluminal MCA occlusion method, combined with unilateral (contralateral) carotid reperfusion was used. Under general anesthesia, the right ECA and CCA were ligated and then the right MCA was occluded for 90 min by means of a silicon-coated 4–0 nylon filament introduced via the ICA through a cut in the right CCA 0.5 cm proximal to the carotid bifurcation. Reperfusion was achieved by pulling out the monofilament from the CCA [7–11] (Figure 1A). For the BICAR group, the right CCA was temporally occluded after anesthesia. The right ECA was separated and occluded permanently at its distal part, the right MCA was occluded for 90 min with a silicon-coated 4–0 nylon filament, introduced through an opening cut in the ECA and then advanced through the ICA. After withdrawing the filament for reperfusion, the ECA was occluded permanently while the CCA was reopened as previously described [12, 13] (Figure 1B).

Magnetic resonance angiography in two different intraluminal middle cerebral artery occlusion (MCAO)/reperfusion rat models. A, UNICAR group, only the right common carotid artery supplied the brain (thick arrows) after reperfusion, the left common carotid artery remained occluded after reperfusion, the left brain is supplied by the contralateral carotid artery via the communication artery; B, BICAR group, bilateral common carotid artery (thick arrows) supplied the brain after reperfusion. The bilateral middle cerebral arteries after reperfusion are shown well in either UNICAR or BICAR model, which indicates that the two models have similar extent of reperfusion. The thin arrows indicate middle cerebral artery in A and B.
Inclusion criteria required each animal to exhibit a decrease in pO2 of > 50% within the infarct area (determined as described below) during MCAO and to survive for at least 24 hours following MCAO.
There were no deaths prior to randomization. In the UNICAR group, one rat died of excessive anesthesia and four rats were excluded from analysis because their pO2 did not meet the criteria. In addition, one rat died of cerebral ischemia after MCAO. The other 9 rats were included in the analysis. In the BICAR group, 2 rats died of subarachnoid hemorrhage and one died of excessive anesthesia. Also, the pO2 changes of 3 rats did not meet the inclusion criteria and they were excluded. The remaining 9 rats were included in the analysis. The analysis therefore included 9 rats in each group.
Measurements
Detection of pO2in ischemic brain tissue
Prior to either MCAO procedure a pO2 detecting probe (Licox® CMP, Kiel, Germany) was implanted according to previously reported stereotactic coordinates [14] to detect pO2 in the core of the ischemic brain tissue during MCAO/reperfusion as shown in Figure 2.

Magnetic resonance imaging showing localization of the pO 2 detecting probe (Licox® CMP) and infarct lesion. A, C, E, DWI, T2WI, and time-of-flight (TOF) image after 90-min ischemia and 1-h reperfusion. B, D, F, DWI, T2WI, and TOF image after 90-min ischemia and 24-h reperfusion. G, H, I, three dimensional localization of the probe. DWI, diffusion-weighted images; T2WI, T2-weighted images.
MRI scan
Three days before the MCAO procedure, a venous catheter was prepared for intravenous contrast injection by inserting a polyethylene catheter (PE-50) into the inferior vena cava. The catheter was filled with heparinized saline, passed through a subcutaneous tunnel, sealed, and then secured at the back of the neck to prevent the animal from removing or damaging it. MRI was performed on anesthetized rats placed in a supine position at 1 hr (DWI and PWI) and 24 hrs (T2WI, DWI, and PWI) following reperfusion with a 3.0 T Philips scanner using a 3 T Solenoid Rat Coil (PFL-Hamburg, Germany). The scanning parameters used are listed in Table 1. Contrast injection was performed as previously described [15]. A neuroradiologist blinded to the type of surgery.
On DWI, infarcted brain tissue was defined on a Philips ViewForum workstation (Philips, The Netherlands) using an apparent diffusion coefficient (ADC) threshold of 0.53 × 10-3 mm2/s, as described elsewhere [16]. On PWI, perfusion was calculated using the NordicIce package (NordicIce, Norway) to determine the PWI lesion defined as tissue with a TTP > 7 sec [17, 18].
Accurate calculation of infarct volume must compensate for the effect of brain edema. Thus, the corrected infarct area was calculated as that total area of the infarct area - (the ischemic hemisphere area - the contralateral hemisphere area), as previously described [19]. The edema area was calculated as ischemic hemisphere area - contralateral hemisphere area. Corrected infarct volume was then calculated by the sum of the corrected infarct area on each section multiplied by slice thickness.
MRI images of insufficient quality were excluded from analysis. T2WI images of one rat were excluded; DWI and PWI images of 4 and of 3 rats respectively were excluded.
Evaluation of neurological deficits: the Bederson and Garcia score
Two neurological grading systems were used to assess the effects of ischemia. The first grading system was published by Bederson et al. in 1986 [20]. This system consists of a scale from 0 to 3: (0) no observable deficit; (1) decreased forelimb resistance to a lateral push; (2) forelimb flexion; (3) circling behavior in addition to the former symptoms. The second system was introduced by Garcia et al. in 1995 [21]. It consists of 6 different criteria (spontaneous activity, symmetry in the movement of the 4 limbs, forepaw outstretching, climbing, body proprioception, and response to vibrissae touch). The individual performance in each test was rated on a 0 to 3 point subscore. The sum of all 6 individual subscores was then calculated to give a range of 3 – 18. Thus, the score in healthy rats would be 18. Two blinded to the type of surgery. The neurological scores of each rat were assessed the neurological score at 24 h following reperfusion as previously described [6, 22].
Histological assessment of infarct volume by 2, 3, 5-triphenyl tetrazolium chloride (TTC) staining
TTC staining was used for histological infarct detection [23]. At 24 h after reperfusion, animals were deeply anesthetized with chloral hydrate and perfused intracardially as previously described [6, 22]. The 24 h time point was chosen as it has been used previously in studies assessing pathophysiological mechanisms of cerebral ischemia [6, 24, 25]. Brains were removed, and 6 coronal sections (2 mm thick slices from anterior, 3.5 mm to anterior, 13.5 mm from bregma) were taken. Sections were then stained with 2% TTC and fixed by immersion in 10% phosphate-buffered paraformaldehyde. The TTC-stained brain sections were photographed and the infarct volumes calculated by an investigator blinded to the type of surgery. The infarct volume was then quantified with the use of imaging software (Image J, National institute of Health, USA) and with the same method as MRI scan see above).
Physiological evaluation
In addition to the experimental rats receiving the examinations mentioned above, MCAO was also performed on an additional 17 rats (8 in the UNICAR group and 9 in the BICAR group) in order to evaluate the physiological changes including changes in serum hemoglobin, serum pH, partial carbon dioxide pressure (pCO2), pO2, electrolytes, serum glucose, and mean arterial blood pressure. These rats were used only for physiological parameter analysis, since blood sampling and femoral catheterization could affect outcome of MCAO/reperfusion. Chloral hydrate (400 mg/kg body weight) injected intraperitoneally was used as the anesthetic for all surgical procedures. After anesthesia, a polyethylene catheter (PE-50) was inserted into the right femoral artery and connected with the Pressure Monitor BP1 to continuously monitor the mean arterial blood pressure (MABP). The physiological evaluations were performed at three time points: before MCAO, at 30 min after MCAO, and at 30 min after reperfusion.
Statistical analysis
Quantitative data were expressed as mean ± standard deviation. Statistically significant differences in continuous variables (physiological parameters, DWI lesion volume, PWI lesion volume, infarct volume, edema volume, corrected infarct volume and neurological scores) between the UNICAR and BICAR groups were determined by independent t-test. The pO2 changes were compared between 2 groups at each time-point using a linear mixed model. The statistical analyses were performed using SAS software version 9.2 (SAS Institute Inc., Cary, NC, USA) and a two-tailed P < 0.05 indicated statistical significance.
Results
Of the 18 rats (9 in each group), 17 (9 in the UNICAR group and 8 in the BICAR group) underwent T2WI at 24 hours, 14 rats (6 in UNICAR group and 8 in BICAR group) had DWI scan at 60 min and 24 hours after reperfusion, and 15 rats (7 in UNICAR group and 8 in BICAR group) had PWI scan at 60 min and 24 hours after reperfusion.
In the additional 17 rats used to investigate physiological parameters at 3 different time points (before MCAO, at 30 min after MCAO, and at 30 min after reperfusion). at all 3 time points, we found no significant differences between the UNICAR and BICAR groups for any measure (Table 2).
Comparison of pO2change during MCAO/reperfusion
At baseline, the average pO2 was 20.54 ± 9.35 and 26.43 ± 7.39, for UNICAR and BICAR groups, respectively (P = 0.519). The pO2 change percentages (compared to baseline) during MCAO (90 min) and reperfusion (30 min) are shown in Figure 3. For both groups, pO2 change percentages showed a decreasing trend over time during MCAO and an increasing trend over time during reperfusion. However, the pO2 change percentages between the UNICAR and BICAR groups did not differ significantly at any time point during MCAO or reperfusion (all P > 0.05).

Comparison of pO 2 change between the unilateral (n = 9) and bilateral carotid artery reperfusion (n = 9) groups during middle cerebral artery occlusion/reperfusion. pO2 change (%) =100 × (pO2 at each time point - baseline pO2)/ baseline pO2. MCAO, middle cerebral artery occlusion; UNICAR, unilateral carotid artery reperfusion; BICAR, bilateral carotid artery reperfusion.
Comparison of infarct volume, edema volume and corrected infarct volume on T2WI
The comparisons of infarct volume, edema volume, and corrected infarct volume on T2WI are shown in Figure 4. Both infarct volume and edema volume on T2WI were larger in the UNICAR group than in the BICAR group, but these differences were not statistically significant (infarct volume: 253.87 ± 91.32 mm3 vs. 174.88 ± 69.47 mm3; P = 0.066, edema volume: 92.83 ± 35.67 mm3 vs. 70.16 ± 36.20 mm3; P = 0.214, corrected infarct volume: 161.04 ± 71.00 mm3 vs. 104.72 ± 34.03 mm3; P = 0.059).

Comparison of infarct volume (A), edema volume (B), and corrected infarct volume (C) on T2WI between rats receiving unilateral (n = 9) and bilateral carotid artery reperfusion (n = 8). UNICAR, unilateral carotid artery reperfusion; BICAR, bilateral carotid artery reperfusion.
Comparison of DWI lesion volume
The comparisons of DWI lesion volume between two groups are shown in Table 3. There was no statistically significant difference in DWI lesion volume between the UNICAR and BICAR groups after either 60 min (83.75 ± 31.6 mm3 vs. 67.52 ± 58.36 mm3; P > 0.05) or 24 hrs following reperfusion (274.28 ± 80.19 mm3 vs. 203.55 ± 65.6 mm3; P > 0.05).
Comparison of PWI lesion volume
The comparisons of PWI lesion volume between two groups are shown in Table 4. There was no statistically significant difference in PWI lesion volume between the UNICAR and BICAR groups after either 60 min (459.99 ± 213.58 mm3 vs. 361.15 ± 366.63 mm3; P > 0.05) or 24 hrs of reperfusion (466.07 ± 241.14 mm3 vs. 428.74 ± 287.8 mm3; P > 0.05).
Comparison of neurological scores at 24 hours after reperfusion
When examined using the Bederson scale (Figure 5A), the UNICAR group had higher average scores than the BICAR group, but this difference did not reach statistical significance (2.61 ± 0.49 vs. 2.33 ± 0.50; P = 0.249). There were also no significant differences between the UNICAR and BICAR groups in the total Garcia score (8.50 ± 1.20 vs. 8.83 ± 2.9; P = 0.757) or in any of the six subscales (Figure 5B).

Comparison of Bederson scale (A) and Garcia scale (B) between unilateral (n = 9) and bilateral carotid artery reperfusion (n = 9) groups. SA: spontaneous activity; SM: symmetry of movements; FO: forepaw outstretching; CL: climbing; BP: body proprioception; VT: vibrissae touch; SUM: sum of Garcia. UNICAR, unilateral carotid artery reperfusion; BICAR, bilateral carotid artery reperfusion.
Comparison of mortality rates at 24 hours after reperfusion
A total of 5 rats died. Two rats died of anesthetic overdose and two of subarachnoid hemorrhage; since the causes of deaths were not related to ischemia or the reperfusion methods, these rats were not included in the statistical analysis. Generally, death from these two causes in animal studies of MCAO should according to convention be excluded from the analysis. One rat in the UNICAR group which was still alive 5 hours after reperfusion, had an initial DWI scan and a very large infarction lesion was found. This rat was found dead 24 hours after reperfusion. After its death, we did not find any subarachnoid bleeding and a very large cerebral infarction area could be seen with the naked eye. Therefore, we believe that this rat died of severe cerebral ischemia, which is actually related to the degree of cerebral ischemia or reperfusion method. Therefore, this death should be included in the mortality statistics. Thus, mortality in the UNICAR group was reported as 1/9, and the mortality in the BICAR group was 0. There was no significant difference in mortality between the two groups.
Comparison of infarct volume, edema volume and corrected infarct volume by TTC staining
The comparisons of infarct volume, edema volume, and corrected infarct volume by TTC staining are shown in Figure 6. Both infarct volume and edema volume by TTC staining in the UNICAR group did not differ significantly from the BICAR group (infarct volume: 370.78 ± 97.73 mm3 vs. 291.69 ± 147.36 mm3; P = 0.198, edema volume: 141.60 ± 68.37 mm3 vs. 89.23 ± 52.32 mm3; P = 0.087, corrected infarct volume: 229.18 ± 69.52 mm3 vs. 202.46 ± 99.12 mm3; P = 0.517).

Comparison of infarct volume (A), edema volume (B), and corrected infarct volume (C) by TTC staining between rats receiving unilateral (n = 9) and bilateral cerebral artery reperfusion (n = 9). UNICAR, unilateral carotid artery reperfusion; BICAR, bilateral carotid artery reperfusion.
Discussion
In this study we found that counter to our original hypothesis, there were no statistically significant differences between the UNICAR and BICAR groups in all parameters observed. We initially hypothesized that there would be higher blood flow obtained by using bilateral reperfusion, which would result in better physiological and behavioral outcomes. However, no such differences were found. These similarities were unexpected as changes in variables such as age [3] and strain [2] of the animal, filament type [5], and ischemia duration [4, 26] result in different outcomes in the effects of MCAO, so it was thought that major differences in reperfusion technique would also result in differences in both histological and functional neurological outcomes.
Infarct size is positively correlated with the duration of transient ischemia [4, 26]. As we expected BICAR to result in faster and more widespread increases in blood flow, this should have resulted in smaller infarct size, which did not occur. A possible explanation for this would be that the cerebral vascular system of rats is able to compensate for the loss in blood supply from the ipsilateral carotid artery during the reperfusion period. Anatomically, this could be the result of the vertebral arteries (via posterior communicating arteries and pial collateral vessels) and contralateral carotid artery (via anterior carotid artery and pial collateral vessels) supplying the ischemic cerebral hemisphere during reperfusion [7, 27]. Interestingly, while duration of ischemia correlates with infarct size, reperfusion has also been found to produce brain damage. Deleterious biochemical processes, particularly the formation of ubiquitin aggregates, during reperfusion after ischemia have been shown to antagonize the beneficial effects of oxygen and glucose supply reinstatement [28]. In the Aronowski et al. study, rats that underwent unilateral MCA/CCA occlusion lasting 120–300 min exhibited significantly greater infarct volume than rats receiving permanent occlusion [29]. Accumulation of ubiquinated protein aggregates after cerebral ischemia has been thought to cause neuronal degeneration [30]. In addition, results from a recent study suggest that reperfusion rather than ischemia is the triggering factor for ubiquination [29]. The results from the current study may in line with the theory that both protective and deleterious events are associated with reperfusion after ischemia.
The primary limitation of our study was that we did not observe long-term neurobehavioral outcomes of rats with ischemia/reperfusion, only a single 90 min duration of ischemia was performed. Also, as cerebral ischemia can have effects on various physiological functions, it would be impossible to account for all of them in the current study. Future studies using longer ischemia and survival and, as well as examining other physiological parameters will be necessary to determine this. Another limitation is that we used the 3.0T MRI scanner that is used in clinical practice to scan the rats. Although the scanning coils were specialized coils for rats, using an MRI scanner designed for clinical use may produce some errors. In the future, we plan to perform post-ischemic cerebral perfusion studies in rats using an MRI instrument designed for animals with a higher field (>7T), which may reduce the variability.
Conclusions
We conclude that despite our original hypotheses, the UNICAR and BICAR techniques resulted in similar neurophysiological and histological outcomes at 24 hrs after ischemia/reperfusion, the time commonly used for observation of the neuroprotective effects of various compounds in male Sprague Dawley rats. These similarities of effects were found across all parameters, including infarct volume, the effects on the ischemic tissue itself, and locomotor deficits commonly associated with unilateral cerebral ischemia. These results suggest that while other variables involved in induction of ischemia will influence outcomes, the type of reperfusion method may not. This finding is potentially of great benefit to the scientific community as it allows comparison of studies using different reperfusion techniques without worrying about the introduction of confounding variables and it also allows experimenters to choose which reperfusion technique to use based on practical matters instead of difference in effects. However, additional studies using longer periods of assessment than 24 h after reperfusion are needed to evaluate possible differences in neurological outcome between the two methods.
Authors’ information
Shared authorship: Jian-Ren Liu, Ulf R. Jensen-Kondering.
References
Liu F, McCullough LD: Middle cerebral artery occlusion model in rodents: methods and potential pitfalls. J Biomed Biotechnol. 2011, 2011: 464701.
Prieto R, Carceller F, Roda JM, Avendano C: The intraluminal thread model revisited: Rat strain differences in local cerebral blood flow. Neurol Res. 2005, 27: 47-52. 10.1179/016164105X18214.
Wang RY, Wang PS, Yang YR: Effect of age in rats following middle cerebral artery occlusion. Gerontology. 2003, 49: 27-32. 10.1159/000066505.
Lim SH, Le JS, Lee JI, Ko YJ, Kim HW: The quantitative assessment of functional impairment and it’s correlation to infarct volume in rats with transient middle cerebral artery occlusion. Brain Res. 2008, 1230: 303-309.
Shimamura N, Matchett G, Tsubokawa T, Ohkuma H, Zhang J: Comparison of silicon-coated nylon suture to plain nylon suture in the rat middle cerebral artery occlusion model. J Neurosci Methods. 2006, 156: 161-165. 10.1016/j.jneumeth.2006.02.017.
Liu JR, Zhao Y, Patzer A, Staak N, Boehm R, Deuschl G, Culman J, Bonny C, Herdegen T, Eschenfelder C: The c-jun n-terminal kinase (jnk) inhibitor xg-102 enhances the neuroprotection of hyperbaric oxygen after cerebral ischaemia in adult rats. Neuropathol Appl Neurobiol. 2010, 36: 211-224. 10.1111/j.1365-2990.2009.01047.x.
Koizumi JY, Nakazawa TO, Ooneda G: Experimental studies of ischemic brain edema. I: a new experimental model of cerebral embolism in rats in which recirculation can be introduced in the ischemic area. Jpn J Stroke. 1986, 8: 1-8. 10.3995/jstroke.8.1.
Xu J, Culman J, Blume A, Brecht S, Gohlke P: Chronic treatment with a low dose of lithium protects the brain against ischemic injury by reducing apoptotic death. Stroke. 2003, 34: 1287-1292. 10.1161/01.STR.0000066308.25088.64.
Zhao Y, Patzer A, Herdegen T, Gohlke P, Culman J: Activation of cerebral peroxisome proliferator-activated receptors gamma promotes neuroprotection by attenuation of neuronal cyclooxygenase-2 overexpression after focal cerebral ischemia in rats. FASEB J. 2006, 20: 1162-1175. 10.1096/fj.05-5007com.
Neumann-Haefelin T, Kastrup A, de Crespigny A, Yenari MA, Ringer T, Sun GH, Moseley ME: Serial mri after transient focal cerebral ischemia in rats: Dynamics of tissue injury, blood–brain barrier damage, and edema formation. Stroke. 2000, 31: 1965-1972. 10.1161/01.STR.31.8.1965. discussion 1972–1963
Hartings JA, Rolli ML, Lu XC, Tortella FC: Delayed secondary phase of peri-infarct depolarizations after focal cerebral ischemia: relation to infarct growth and neuroprotection. J Neurosci. 2003, 23: 11602-11610.
Longa EZ, Weinstein PR, Carlson S, Cummins R: Reversible middle cerebral artery occlusion without craniectomy in rats. Stroke. 1989, 20: 84-91. 10.1161/01.STR.20.1.84.
Cuomo O, Gala R, Pignataro G, Boscia F, Secondo A, Scorziello A, Pannaccione A, Viggiano D, Adornetto A, Molinaro P, Li XF, Lytton J, Di Renzo G, Annunziato L: A critical role for the potassium-dependent sodium-calcium exchanger nckx2 in protection against focal ischemic brain damage. J Neurosci. 2008, 28: 2053-2063.
Liu S, Liu W, Ding W, Miyake M, Rosenberg GA, Liu KJ: Electron paramagnetic resonance-guided normobaric hyperoxia treatment protects the brain by maintaining penumbral oxygenation in a rat model of transient focal cerebral ischemia. J Cereb Blood Flow Metab. 2006, 26: 1274-1284. 10.1038/sj.jcbfm.9600277.
Jensen UR, Liu JR, Eschenfelder C, Meyne J, Zhao Y, Deuschl G, Jansen O, Ulmer S: The correlation between quantitative t2' and regional cerebral blood flow after acute brain ischemia in early reperfusion as demonstrated in a middle cerebral artery occlusion/reperfusion model of the rat. J Neurosci Methods. 2009, 178: 55-58. 10.1016/j.jneumeth.2008.11.023.
Meng X, Fisher M, Shen Q, Sotak CH, Duong TQ: Characterizing the diffusion/perfusion mismatch in experimental focal cerebral ischemia. Ann Neurol. 2004, 55 (2): 207-212. 10.1002/ana.10803.
Neumann-Haefelin T, Wittsack HJ, Wenserski F, Siebler M, Seitz RJ, Mödder U, Freund HJ: Diffusion- and perfusion-weighted MRI. The DWI/PWI mismatch region in acute stroke. Stroke. 1999, 30 (8): 1591-1597. 10.1161/01.STR.30.8.1591.
Schellinger PD, Latour LL, Wu CS, Chalela JA, Warach S: The association between neurological deficit in acute ischemic stroke and mean transit time: Comparison of four different perfusion mri algorithms. Neuroradiology. 2006, 48: 69-77. 10.1007/s00234-005-0012-9.
Swanson RA, Morton MT, Tsao-Wu G, Savalos RA, Davidson C, Sharp FR: A semiautomated method for measuring brain infarct volume. J Cereb Blood Flow Metab. 1990, 10: 290-293. 10.1038/jcbfm.1990.47.
Bederson JB, Pitts LH, Tsuji M, Nishimura MC, Davis RL, Bartkowski H: Rat middle cerebral artery occlusion: evaluation of the model and development of a neurologic examination. Stroke. 1986, 17: 472-476. 10.1161/01.STR.17.3.472.
Garcia JH, Wagner S, Liu KF, Hu XJ: Neurological deficit and extent of neuronal necrosis attributable to middle cerebral artery occlusion in rats. Statistical validation. Stroke. 1995, 26: 627-634. 10.1161/01.STR.26.4.627. discussion 635
Eschenfelder CC, Krug R, Yusofi AF, Meyne JK, Herdegen T, Koch A, Zhao Y, Carl UM, Deuschl G: Neuroprotection by oxygen in acute transient focal cerebral ischemia is dose dependent and shows superiority of hyperbaric oxygenation. Cerebrovasc Dis. 2008, 25: 193-201.
Hatfield RH, Mendelow AD, Perry RH, Alvarez LM, Modha P: Triphenyltetrazolium chloride (ttc) as a marker for ischaemic changes in rat brain following permanent middle cerebral artery occlusion. Neuropathol Appl Neurobiol. 1991, 17: 61-67. 10.1111/j.1365-2990.1991.tb00694.x.
McCarthy CA, Vinh A, Broughton BR, Sobey CG, Callaway JK, Widdop RE: Angiotensin II type 2 receptor stimulation initiated after stroke causes neuroprotection in conscious rats. Hypertension. 2012, Oct 22 [Epub ahead of print]
Raida Z, Hundahl CA, Kelsen J, Nyengaard JR, Hay-Schmidt A: Reduced infart size in neuroglobin-null mice after experimental stroke in vivo. Exp Transl Stroke Med. 2012, 4 (1): 15-10.1186/2040-7378-4-15.
Calloni RL, Winkler BC, Ricci G, Potetto MG, Homero WM, Serafinni EP, Corleta OC: Transient middle cerebral artery occlusion in rats as an experimental model of brain ischemia. Acta Cirugica Brasilerira. 2010, 25 (5): 428-433. 10.1590/S0102-86502010000500008.
Dai WJ, Funk A, Herdegen T, Unger T, Culman J: Blockade of central angiotensin at(1) receptors improves neurological outcome and reduces expression of ap-1 transcription factors after focal brain ischemia in rats. Stroke. 1999, 30: 2391-2398. 10.1161/01.STR.30.11.2391. discussion 2398–2399
Aronowski J, Strong R, Grotta JC: Reperfusion injury: demonstration of brain damage produced by reperfusion after transient focal ischemia in rats. J Cereb Blood Flow Metab. 1997, 17 (10): 1048-1056.
Hochrainer K, Jackman K, Anrather J, Iadecola C: Reperfusion rather than ischemia drives the formation of ubiquitin aggregates after middle cerebral artery occlusion. Stroke. 2012, 43 (8): 2229-2235. 10.1161/STROKEAHA.112.650416.
Hu BR, Martone ME, Jones YZ, Liu CL: Protein aggregation after transient cerebral ischemia. J Neurosci. 2000, 20 (9): 3191-3199.
Acknowledgements
This work was supported by the China Visiting Scholars Program, Campus Kiel, Germany and grants from the National Natural Science Foundation of China [No. 81070914 and 81271302 to J.R. Liu]; and a grant from the “New One Hundred Talent Project” from Shanghai Jiao Tong University School of Medicine, China [2012, to J.R. Liu].
Author information
Authors and Affiliations
Corresponding authors
Additional information
Competing interests
The authors declare to have no competing interests.
Authors’ contributions
JRL contributed to study concepts, study design, definition of intellectual content, literature research, experimental studies, data acquisition, data analysis, statistical analysis, manuscript preparation and drafting of the manuscript. URJ contributed to definition of intellectual content, literature research, data analysis, statistical analysis, manuscript editing and manuscript review. JJZ, FS, XYF and XLS contributed to experimental studies and data acquisition. GD contributed to manuscript review and supervision. OJ is the guarantor of integrity of the entire study, supervision. TH contributed to manuscript review. JM contributed to experimental studies and data acquisition. YZ contributed to experimental studies and data analysis. CE contributed to study concepts, study design, definition of intellectual content, literature research, manuscript editing, manuscript review and supervision. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Liu, JR., Jensen-Kondering, U.R., Zhou, JJ. et al. Transient filament occlusion of the middle cerebral artery in rats: does the reperfusion method matter 24 hours after perfusion?. BMC Neurosci 13, 154 (2012). https://doi.org/10.1186/1471-2202-13-154
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2202-13-154