
Abstract
Background
Bone metastasis is known to occur in some patients with cancer, usually in the spine, pelvis or ribs, and less than 0.01% of patients have metastases in the foot bone, so metatarsal metastasis is quite rare. The initial symptoms of osseous metastases are swelling, pain, or both.
Case presentation
We report a 68-year-old man with solitary metatarsal metastasis 26 months after a diagnosis of renal clear cell carcinoma. The patient suffered intermittent swelling of his right foot and pain for one year due to trauma and was not treated. The doctor attributed the symptoms to trauma, administering massage therapy and a plaster cast to the patient at the local clinic. After reviewing the medical records, we found that this patient had a history of clear cell renal cell carcinoma. The patient underwent radiological examination and open biopsy of the first metatarsal bone of the right foot. These findings confirmed that the patient had a metatarsal metastasis from clear cell renal cell carcinoma. The patient subsequently underwent right foot amputation. No local recurrence or distant metastasis was found after a 6-month follow-up.
Conclusion
Clinicians should be aware of a history of renal cell carcinoma (RCC) and fully understand the patient’s past medical history. When treating patients with clear cell renal cell carcinoma who have unresolving bony pain or swelling, clinicians should always keep in mind the possibility of bone metastasis of RCC.
Similar content being viewed by others


Background
Metastatic disease of the skeleton often occurs in patients with malignancy, with bone damage and pain as the main manifestations. Malignant tumours prone to bone metastasis are breast cancer, lung cancer, kidney cancer, and other common primary cancers, including prostate cancer [1]. The sites of bone metastases are frequently localized in the axial skeleton, such as the spine and pelvis. Metastatic diseases of the distal knee and elbow joints are unusual. Bone metastasis of the foot is rare, occurring in approximately 0.01% of all metastatic bone diseases and is usually a late manifestation of disseminated disease [2, 3]. We report metatarsal metastasis from clear cell renal cell carcinoma in a 68-year-old man and review the related literature.
Case presentation
A 68-year-old male with intermittent swelling of his right foot and pain for one year was admitted in July 2019. The patient had a history of a mild right foot sprain that caused pain a year prior. Initially, the pain was relieved after rest but progressed with worsening pain and swelling after daily activities. At the local clinic, the doctor attributed the symptoms to trauma, administering massage therapy and a plaster cast to the patient, and the symptoms were alleviated. Two months before hospitalization, the patient’s right foot was continuously swollen with worsening, severe pain that limited ambulation. For further treatment, the patient came to our outpatient clinic and underwent X-ray examination of the right foot. The physical examination demonstrated that the soft tissue was mildly swollen. There was pain on palpation in the first metatarsus of the right foot. There was no paresthesia of the surrounding skin. The results of radiographs confirmed bone destruction of the first metatarsus of the right foot, which suggested underlying malignancy (Fig. 1a and b).

X-ray scan of the patient. a Posteroanterior radiograph. b Lateral radiograph
After reviewing the medical history, we discovered that the patient had a history of a large left renal mass discovered in April 2017 (Fig. 2). Computed tomography (CT) showed a round low-density shadow in the left inferior kidney, approximately 13*10 cm in size, with uneven density. There were flaky low-density shadows and point-like high-density shadows. Subsequently, the work-up was negative for metastatic disease, and radical nephrectomy was performed. Postoperative pathological results demonstrated stage II (T2N0M0) clear cell renal cell carcinoma (Fuhrman nuclear grade 2). After discharge, the patient was reviewed regularly in a polyclinic and received Chinese herbal treatment. Therefore, in the context of a known primary RCC, a metatarsal metastasis was suspected. The patient was admitted to the orthopaedic department for further treatment.

Abdominal CT showing a tumour in the left kidney
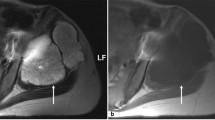
After admission, the patient underwent magnetic resonance imaging (MRI), revealing a mass on the right first metatarsal bone with a less clear margin, approximately 5.19 cm in diameter, which had an isointense signal on T1-weighted images (Fig. 3a) and a mixed slightly high signal on T2-weighted images (Fig. 3b), with bone destruction, which was considered to be a malignant tumour. The results of the CT scan were consistent with those of MRI. After thorough examination and evaluation, no other distant metastatic lesions were found in the patient. Next, the patient underwent open biopsy of the first metatarsal bone of the right foot. Histological examination revealed clear cell carcinoma with nephrogenic implications (Fig. 4). Therefore, metatarsal metastasis from clear cell renal cell carcinoma was confirmed. The patient subsequently underwent right foot amputation (Fig. 5a and b). Six months after surgery, the patient walked with crutches and was re-examined at the orthopaedic clinic of our hospital. No local recurrence or distant metastasis was found.

Foot magnetic resonance imaging scans of the patient. a T1-weighted images. b T2-weighted images

Postoperative pathology of the metatarsal bone

Postoperative X-ray scan of the patient. a Positive radiograph. b Lateral radiograph
Discussion and conclusion
RCC is commonly known to metastasize to the lungs, bone, and brain, but RCC can metastasize to some atypical sites as well, such as skeletal muscle [4], scalp [5] and uvula [6], as described in the literature. This report describes the metastasis of clear cell renal cell carcinoma to the metatarsus. Previously reported malignant tumours that metastasized to the foot skeleton are listed in Tables 1 and 2. The most common primary cancer of foot bone metastasis is lung cancer, followed by renal and intestinal tumours [7, 50, 51]. In metastatic RCC, bone metastases occur in almost 30% of patients [52]. Bone metastases are a common site of relapse in many types of solid cancers. Most bone metastases occur in the spine, followed by the pelvis and long bones. Acrometastasis (defined as metastasis to the hand or foot) is quite rare [2]. The metastatic sites of foot bones are summarized in Table 3 according to previous case reports. The calcaneus is the foot bone most commonly involved [18, 35].
In this case report, the clinician did not inquire about the patient’s previous medical history, nor did he perform any image examination for the foot for the patient upon first presentation. During the 1-year period, the patient developed intermittent swelling of the right foot with mild pain and an inability to walk without receiving definite diagnosis and timely treatment. Diagnostic delay may lead to pathological fractures; therefore, metastatic bone disease of the foot may affect the quality of life of patients, particularly as they are ambulating. However, the combination of medical history and imaging examination usually reveals the underlying diagnosis and provides a reference for treatment. For that reason, we report metatarsal metastasis from clear cell renal cell carcinoma in a 68-year-old man and review cases of foot bone metastasis of renal cancer reported in previous literature (Table 4). In these cases, the most common pathological type of foot bone metastasis was clear cell renal cell carcinoma, which represents the most common histology of renal carcinoma and has a worse prognosis than other RCCs [54,55,56]. All patients in Table 4 were male. Studies have reported a 4:1 male predominance in clear cell renal cell carcinoma with bone metastasis [57]. Almost all the patients received surgical treatment.
As no therapeutic standard or guideline currently exists for RCC with bone metastasis. The median survival time of RCC with bone metastasis is usually below 24 months [57]. Acrometastases are often associated with extensive metastasis in other sites, so the prognosis is poor. The treatment is usually palliative and needs to be adapted to each patient’s individual condition. Relief of pain is often the therapeutic goal. Palliative treatment of bone metastases has always been conservative: radiotherapy, chemotherapy, immunotherapy, targeted therapy, bisphosphonates and analgesics [58]. More recently, minimally invasive techniques, including ethanol ablation, laser ablation, microwave ablation, cryoablation and radiofrequency ablation, have been used for painful bone lesions [59,60,61,62,63]. Surgical resection of bone metastasis from RCC has been reported to improve the prognosis of patients, and the effect is further improved for solitary metastasis if feasible [64]. These conditions were all met in our case. We believe that the best treatment for a single metastasis is always surgical excision if there is a long time from nephrectomy to the detection of isolated metastasis.
In conclusion, clinicians should fully understand the patient’s past medical history. Even though acrometastasis is rare, this diagnosis should be considered in any patient with a history of RCC, particularly male patients, with local pain and swelling. Appropriate clinical and radiographic evaluation of these patients is essential to offer timely local therapy that may improve prognosis and enhance patient quality of life.
Availability of data and materials
All data supporting the study are presented in the manuscript or available upon request.
Abbreviations
- CT:
-
Computed Tomography
- MRI:
-
Magnetic Resonance Imaging
- RCC:
-
Renal Cell Carcinoma
References
Salapura V, Zupan I, Seruga B, Gasljevic G, Kavcic P. Osteoblastic bone metastases from renal cell carcinoma. Radiol Oncol. 2014;48(3):243–6.
Rice B, Ross J, Todd N, Caputo L, Rush S, Shrestha B. Pulmonary pleomorphic carcinoma metastasis to the midfoot. J Foot Ankle Surg. 2015;54(3):483–6.
Maheshwari AV, Chiappetta G, Kugler CD, Pitcher JD Jr, Temple HT. Metastatic skeletal disease of the foot: case reports and literature review. Foot Ankle Int. 2008;29(7):699–710.
Salman R, Sebaaly MG, Asmar K, Nasserdine M, Bannoura S, Khoury NJ. Rare skeletal muscle metastasis from renal cell carcinoma: case report and review of the literature. CEN Case Rep. 2018;7(2):316–9.
Errami M, Margulis V, Huerta S. Renal cell carcinoma metastatic to the scalp. Rare Tumors. 2016;8(4):6400.
Khade P, Devarakonda S. Atypical metastasis of renal cell carcinoma to the uvula: case report and review of literature. Int Med Case Rep J. 2018;11:29–32.
Kemnitz MJ, Erdmann BB, Julsrud ME, Jacobs PM, Ringstrom JB. Adenocarcinoma of the lung with metatarsal metastasis. J Foot Ankle Surg. 1996;35(3):210–2.
Dai H, Qiang M, Chen Y, Zhai W, Zhang K. Lung cancer presenting as heel pain: a case report. Oncol Lett. 2014;8(2):736–8.
Baran R, Tosti A. Metastatic carcinoma to the terminal phalanx of the big toe: report of two cases and review of the literature. J Am Acad Dermatol. 1994;31(2 Pt 1):259–63.
Delgadillo LA, Nichols DE. Oat cell carcinoma metastasis to the foot. J Foot Ankle Surg. 1998;37(1):55–62.
Wu KK. Bronchogenic carcinoma with metastases to the foot: a report of two cases. J Foot Ankle Surg. 1995;34(3):322–6.
Trinidad J, Kaplansky D, Nerone V, Springer K. Metastatic adenosquamous carcinoma of the foot: a case report. J Foot Ankle Surg. 2012;51(3):345–51.
Gan K, Shen Y. Metastatic pulmonary adenocarcinoma of the talus: a case report. J Foot Ankle Surg. 2017;56(4):827–31.
Iselin LD, Symeonidis PD, Stavrou P. Solitary navicular metastasis of a pulmonary adenocarcinoma. Foot Ankle Spec. 2011;4(6):373–5.
Li W, Li W, Zhang R. Metastasis to the medial cuneiform bone from squamous cell carcinoma of the lung revealed by bone Scintigraphy. Clin Nucl Med. 2016;41(12):946–7.
Singh C, Gupta M, Singh J, Ali A. Isolated calcaneal metastasis: an unusual presentation of lung carcinoma as heel pain. Clin Nucl Med. 2016;41(3):214–6.
Ciccone MA, Conturie CL, Lee CM, Matsuo K. Toe metastasis: a rare pattern of cervical cancer spread. Gynecol Oncol Case Rep. 2014;8:7–9.
Cooper JK, Wong FL, Swenerton KD. Endometrial adenocarcinoma presenting as an isolated calcaneal metastasis. A rare entity with good prognosis. Cancer. 1994;73(11):2779–81.
Longo R, Gamelon-Benichou C, Elias-Matta C, Platini C, Eid N, Yacoubi M, Quetin P. An unusual solitary metatarsal metastasis from an Endometrioid endometrial adenocarcinoma. Am J Case Rep. 2015;16:473–7.
Ali ZA, Wimhurst JA, Ali AA, Tempest ME, Edwards DJ. Endometrial cancer metastasis presenting as a grossly swollen toe. Int J Gynecol Cancer. 2003;13(6):909–11.
Amiot RA, Wilson SE, Reznicek MJ, Webb BS. Endometrial carcinoma metastasis to the distal phalanx of the hallux: a case report. J Foot Ankle Surg. 2005;44(6):462–5.
Manolitsas TP, Fowler JM, Gahbauer RA, Gupta N. Pain in the foot: calcaneal metastasis as the presenting feature of endometrial cancer. Obstet Gynecol. 2002;100(5 Pt 2):1067–9.
Reyes DK, Miller JA, Cerrato RA, Pienta KJ. Oligometastatic prostate cancer to the navicular bone: case report. Urol Case Rep. 2015;3(3):59–62.
Agrawal S, Irvine A, Money-Kyrle J, Ellis BW. Isolated calcaneal metastasis from prostate cancer. Ann R Coll Surg Engl. 2008;90(3):W7–9.
Oh WK, Loda M, Kantoff PW, Janicek M. Progressive sclerosis of isolated foot metastasis of prostate cancer. J Urol. 2002;167(3):1392.
McCarthy MT, Ebrahem H, Aibdeen Z, Hodnett PA, Mulcahy E, Osman N. Prostate cancer metastasis to calcaneus: a solitary lesion at an atypical site, dormant for more than 10 years. JRSM Open. 2016;7(10):2054270416660934.
Bibbo C, Hatfield SP, Albright JT. Treatment of metastatic prostate adenocarcinoma to the calcaneus. J Foot Ankle Surg. 2010;49(2):159):e115–20.
Ravind R, Prameela CG, Gurram BC, Dinesh M. Synchronous phalangeal metastases in upper and lower limbs from primary breast malignancy: a rare case scenario with a review of the literature. BMJ Case Rep. 2015;2015.
Groves MJ, Stiles RG. Metastatic breast cancer presenting as heel pain. J Am Podiatr Med Assoc. 1998;88(8):400–5.
Wu KK, Guise ER. Metastatic tumors of the foot. South Med J. 1978;71(7):807–8 812.
Wijayaratna R, Ng JW. Metatarsal metastasis as the presenting feature of occult colorectal carcinoma. BMJ Case Rep. 2013;2013:bcr2013010353.
Ellington JK, Kneisl JS. Acrometastasis to the foot: three case reports with primary colon cancer. Foot Ankle Spec. 2009;2(3):140–5.
Sworn MJ, Buchanan R, Moynihan FJ. Rectal carcinoma presenting as massive metastatic involvement of foot bones. Br Med J. 1978;2(6130):98–9.
Petkovic M, Muhvic D, Zamolo G, Jonjic N, Mustac E, Mrakovcic-Sutic I, Seili-Bekafigo I. Metatarsal metastasis from transitional cell cancer of the urinary bladder. Coll Antropol. 2004;28(1):337–41.
Yadav R, Ansari MS, Dogra PN. Renal cell carcinoma presenting as solitary foot metastasis. Int Urol Nephrol. 2004;36(3):329–30.
Perdona S, Autorino R, Gallo L, Des M, Marra L, Claudio L, Caraco C, Franco R, Fazzioli F, Gallo A. Renal cell carcinoma with solitary toe metastasis. Int J Urol. 2005;12(4):401–4.
Choufani E, Diligent J, Galois L, Mainard D. Metastatic renal cell carcinoma presenting as foot metastasis: case report and review of the literature. J Am Podiatr Med Assoc. 2011;101(3):265–8.
Tonogai I, Nishisho T, Miyagi R, Sairyo K. Total calcanectomy for metastasis of renal cell carcinoma in the calcaneus: a case report. Foot Ankle Surg. 2018;24(1):e7–e12.
Chauveaux D, Liquois F, Le Huec JC, Le Rebeller A. Metatarsal metastasis. A case treated by exeresis an reconstruction. Rev Chir Orthop Reparatrice Appar Mot. 1990;76(7):525–7.
Kumar PP, Kovi J. Metastases to bones of the hands and feet. J Natl Med Assoc. 1978;70(11):837–40.
Anderson EE, Leitner WA, Boyarsky S, Small MP, McCollum DE. Renal-cell carcinoma metastatic to great toe. J Bone Joint Surg Am. 1968;50(5):997–8.
Bergqvist D, Mattsson J. Solitary calcaneal metastasis as the first sign of gastric cancer. A case report. Ups J Med Sci. 1978;83(2):115–8.
Kakarala G, Chatha H, Ferns B, Ebizie A. Metastatic gastric adenocarcinoma mimicking osteomyelitis of second toe. Foot (Edinb). 2008;18(3):171–3.
Ryder JH, McGarry SV, Wang J. Calcaneal acrometastasis from urothelial carcinoma of the ureter: a case report and literature review. Clin Interv Aging. 2013;8:395–9.
Zhang J, Sun Y, Li Z, Feng H. Metastasis of submandibular gland carcinoma to the toe bone: a case report. Br J Oral Maxillofac Surg. 2019;57(4):368–70.
Friend G, Mitchell J. Metastatic melanoma of a MetatarsalA case report. J Am Podiatr Med Assoc. 2017;107(1):90–4.
Allman LM. Metastatic bone involvement of the hallux distal phalanx and cuboid in an elderly patient with non-Hodgkin lymphoma. Foot Ankle Spec. 2008;1(6):355–8.
Lee DK. Distant metastases to the hallux in nasopharyngeal carcinoma. J Am Podiatr Med Assoc. 2008;98(3):239–41.
Mohanty A, Dutta D, Das S, Samanta DR, Senapati S. Carcinoma esophagus with isolated metatarsal metastasis. Indian J Cancer. 2011;48(1):112–3.
Nakagawa R, Susa M, Nakayama R, Watanabe I, Horiuchi K, Toyama Y, Nakamura M, Matsumoto M, Morioka H. Metastasis of renal cell carcinoma to the trapezium. J Hand Surg Asian Pac Vol. 2017;22(2):262–5.
Malone M, Gannass A, Binahmed A, Bowling FL, Boulton AJ. An extensive primary nodular melanoma of the foot with associated distant metastases: a case report. Foot (Edinb). 2012;22(3):235–9.
Woodward E, Jagdev S, McParland L, Clark K, Gregory W, Newsham A, Rogerson S, Hayward K, Selby P, Brown J. Skeletal complications and survival in renal cancer patients with bone metastases. Bone. 2011;48(1):160–6.
Zhang J, Li Z, Ma X, Feng H: A pathological toe fracture as the first presentation of cervical cancer: A case report. Medicine (Baltimore) 2019, 98(3):e14190.
Keegan KA, Schupp CW, Chamie K, Hellenthal NJ, Evans CP, Koppie TM. Histopathology of surgically treated renal cell carcinoma: survival differences by subtype and stage. J Urol. 2012;188(2):391–7.
Capitanio U, Cloutier V, Zini L, Isbarn H, Jeldres C, Shariat SF, Perrotte P, Antebi E, Patard JJ, Montorsi F, et al. A critical assessment of the prognostic value of clear cell, papillary and chromophobe histological subtypes in renal cell carcinoma: a population-based study. BJU Int. 2009;103(11):1496–500.
Leibovich BC, Lohse CM, Crispen PL, Boorjian SA, Thompson RH, Blute ML, Cheville JC. Histological subtype is an independent predictor of outcome for patients with renal cell carcinoma. J Urol. 2010;183(4):1309–15.
Huang Z, Du Y, Zhang X, Liu H, Liu S, Xu T. Clear cell renal cell carcinoma bone metastasis: what should be considered in prognostic evaluation. Eur J Surg Oncol. 2019;45(7):1246–52.
Fizazi K, Lipton A, Mariette X, Body JJ, Rahim Y, Gralow JR, Gao G, Wu L, Sohn W, Jun S. Randomized phase II trial of denosumab in patients with bone metastases from prostate cancer, breast cancer, or other neoplasms after intravenous bisphosphonates. J Clin Oncol. 2009;27(10):1564–71.
Gangi A, Kastler B, Klinkert A, Dietemann JL. Injection of alcohol into bone metastases under CT guidance. J Comput Assist Tomogr. 1994;18(6):932–5.
Groenemeyer DH, Schirp S, Gevargez A. Image-guided percutaneous thermal ablation of bone tumors. Acad Radiol. 2002;9(4):467–77.
Simon CJ, Dupuy DE, Mayo-Smith WW. Microwave ablation: principles and applications. Radiographics. 2005;25(Suppl 1):S69–83.
Callstrom MR, Atwell TD, Charboneau JW, Farrell MA, Goetz MP, Rubin J, Sloan JA, Novotny PJ, Welch TJ, Maus TP, et al. Painful metastases involving bone: percutaneous image-guided cryoablation--prospective trial interim analysis. Radiology. 2006;241(2):572–80.
Toyota N, Naito A, Kakizawa H, Hieda M, Hirai N, Tachikake T, Kimura T, Fukuda H, Ito K. Radiofrequency ablation therapy combined with cementoplasty for painful bone metastases: initial experience. Cardiovasc Intervent Radiol. 2005;28(5):578–83.
Ljungberg B, Bensalah K, Canfield S, Dabestani S, Hofmann F, Hora M, Kuczyk MA, Lam T, Marconi L, Merseburger AS, et al. EAU guidelines on renal cell carcinoma: 2014 update. Eur Urol. 2015;67(5):913–24.
Acknowledgements
Not applicable.
Funding
None to declare.
Author information
Authors and Affiliations
Contributions
HW, RH, and HF collected the patient’s data. HW, QZ and YZ analysed the data and performed the reference search. HW, RH, QZ and HF drafted and revised the manuscript. All authors contributed to data analysis and drafting and revision of the manuscript, and read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the participants for publication of this article and any accompanying tables/images.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Wu, H., Han, R., Zhang, Q. et al. Metatarsal metastasis from clear cell renal cell carcinoma: a case report and literature review. BMC Urol 20, 19 (2020). https://doi.org/10.1186/s12894-020-00588-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12894-020-00588-4