
Abstract
Background
Infection of the lower airways by rhinovirus, a member of the picornavirus family, is an important cause of wheezing illnesses in infants, and plays an important role in the pathogenesis of rhinovirus-induced asthma exacerbations. Given the absence of natural rhinovirus infections in rodents, we investigated whether an attenuated form of mengovirus, a picornavirus whose wild-type form causes systemic rather than respiratory infections in its natural rodent hosts, could induce airway infections in rats with inflammatory responses similar to those in human rhinovirus infections.
Results
After inoculation with 107 plaque-forming units of attenuated mengovirus through an inhalation route, infectious mengovirus was consistently recovered on days 1 and 3 postinoculation from left lung homogenates (median Log10 plaque-forming units = 6.0 and 4.8, respectively) and right lung bronchoalveolar lavage fluid (median Log10 plaque-forming units = 5.8 and 4.0, respectively). Insufflation of attenuated mengovirus, but not vehicle or UV-inactivated virus, into the lungs of BN rats caused significant increases (P < 0.05) in lower airway neutrophils and lymphocytes in the bronchoalveolar lavage fluid and patchy peribronchiolar, perivascular, and alveolar cellular infiltrates in lung tissue sections. In addition, infection with attenuated mengovirus significantly increased (P < 0.05) lower airway levels of neutrophil chemoattractant CXCR2 ligands [cytokine-induced neutrophil chemoattractant-1 (CINC-1; CXCL1) and macrophage inflammatory protein-2 (MIP-2; CXCL2)] and monocyte chemoattractant protein-1 (MCP-1; CCL2) in comparison to inoculation with vehicle or UV-inactivated virus.
Conclusion
Attenuated mengovirus caused a respiratory infection in rats with several days of viral shedding accompanied by a lower airway inflammatory response consisting of neutrophils and lymphocytes. These features suggest that mengovirus-induced airway infection in rodents could be a useful model to define mechanisms of rhinovirus-induced airway inflammation in humans.
Similar content being viewed by others

Background
Human rhinovirus (HRV) infections are the most frequent cause of common colds and virus-induced asthma exacerbations, and wheezing HRV infections in infancy are associated with an increased risk for the development of childhood asthma [1–3]. A central conundrum with regard to HRV, a member of the picornavirus family, is explaining how a virus that usually causes a self-limiting upper airway infection, a common cold, can induce asthma exacerbations and provoke persistent lower airway sequelae in susceptible children [4, 5]. An important clue in addressing this issue is the substantial evidence that HRV can infect the lower airways [6–11]. HRV infection of lower airway epithelial cells induces the secretion of a variety of proinflammatory cytokines, chemokines, and mediators [4].
Neutrophils are the predominant inflammatory cell initially recruited to the airways during HRV infections [12, 13], and clinical studies have demonstrated that there is a positive correlation between this inflammatory response and respiratory symptoms and airway dysfunction [14–17]. Although these relationships have been observed in a variety of clinical and experimental infection studies, the nature of this relationship is still enigmatic. It is possible that 1) neutrophilic inflammation causes respiratory symptoms, 2) neutrophils recruited to the airways in response to HRV infection have antiviral effects and contribute to resolution of the infection, or 3) neutrophilic inflammation is an epiphenomenon that does not significantly affect the course of the disease. Finally, perhaps the difference between a relatively uneventful cold and more severe HRV-induced airway sequelae resides in the balance between beneficial and detrimental effects of the neutrophilic inflammatory response.
Progress in understanding the relationship between HRV infection, inflammation, and respiratory symptoms has been significantly hampered by the absence of rodent-specific rhinoviruses. Recently, murine experimental models have been established using either minor group HRV in wild-type mice or major group HRV in mice that are transgenic for human intercellular adhesion molecule-1 (ICAM-1; CD54), the receptor for major group HRV [18, 19]. While these models will be useful, a significant drawback to these models is that HRV replication is short-lived (≤ 24 h) in the mouse. In studying the relationship between viral replication, inflammation, and respiratory dysfunction, it would be advantageous to develop a model with viral replication lasting several days, as occurs during clinical or experimental infections with HRV.
Mengovirus is a picornavirus that naturally infects rodents [20], and the native virus causes systemic infections that resemble poliovirus infections, rather than HRV infections, of humans. The poly(C) tract in the distal region of the 5' untranslated region of the mengovirus genome is a critical virulence determinant that inhibits interferon responses [21–25]. A panel of attenuated mengovirus mutants with varying deletions of the poly(C) tract (wild-type mengovirus has a poly(C) tract length of 44) has been derived, including vMC0, which has no poly(C) tract [21–25]. In contrast to the systemic and often lethal infections caused by wild type mengovirus, intracerebral or intraperitoneal administration of vMC0 induces self-limited infections, and vMC0 also stimulates vigorous type I interferon responses [21–25]. Furthermore, attenuated mengoviruses replicate well in epithelial cells but poorly in macrophage lineage cells [25]. These features are similar to those of HRV infection [4], and led us to hypothesize that inoculation of rats with vMC0 via inhalation could produce infection limited to the respiratory tract, and could serve as a model for HRV infections in humans.
Results
Expression of infectious virus in the lungs after inhalation of attenuated mengovirus
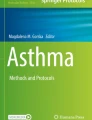
To examine whether attenuated mengovirus could induce lower airway infections in rats, 107 plaque-forming units (PFU) of attenuated mengovirus, vMC0, an equivalent amount of UV-inactivated vMC0, or vehicle were insufflated into the lungs of adult BN rats. On days 1 and 3 postinoculation, significant levels of infectious mengovirus were recovered from left lung homogenates (median Log10 PFU = 6.0 and 4.8, respectively) and right lung bronchoalveolar lavage (BAL) fluid (median Log10 PFU = 5.8 and 4.0, respectively) of BN rats inoculated with the attenuated mengovirus, vMC0 (Figure 1; P < 0.005). By day 5 postinoculation, viral titers in the lung homogenates and BAL fluid of vMC0-inoculated rats were either low or undetectable. Infectious mengovirus was not detected in lung homogenates and BAL fluid from BN rats inoculated with either UV-inactivated vMC0 or vehicle. Examination of brain, heart, and spleen homogenates and plasma revealed no evidence of systemic infection with vMC0.

Lung viral titers after inhalation of attenuated mengovirus. Viral titers in left lung homogenates and BAL fluid (obtained from the right lung) from BN rats inoculated with 107 PFU of attenuated mengovirus, vMC0, an equivalent amount of UV-inactivated vMC0, or vehicle were determined by plaque assays. Data are the total amount of virus present in the lung homogenate or BAL fluid (virus concentrations were multiplied by the volumes of lung homogenate or BAL fluid). Symbols represent data from individual rats. Dotted lines indicate the limits of detection. * P < 0.005 (vMC0 vs. vehicle and UV-inactivated vMC0).
Reduction in body weight gain after inhalation of attenuated mengovirus
A reduction in body weight or in the rate of body weight gain is a sensitive measure of viral respiratory infections in rodents [26]. The percent gain in body weight from the day of the inoculation to day 3 postinoculation was significantly lower in BN rats inoculated with 107 PFU of vMC0 (median = 0.8%; n = 10 rats) than in those receiving the vehicle (median = 2.2%; n = 6 rats; P = 0.04). However, there was no significant difference between the percent gain in body weight in rats inoculated with UV-inactivated vMC0 (median = 1.6%; n = 5 rats) and those inoculated with vehicle, indicating the requirement for replication-competent virus for the observed effects on body weight.
Development of neutrophilic lower airway inflammation after inhalation of attenuated mengovirus
Insufflation of vMC0 (107 PFU) into the lungs of adult BN rats induced the recruitment of neutrophils and lymphocytes into the lower airways. The total number of BAL cells and the numbers of BAL neutrophils and lymphocytes were significantly elevated on days 3 and 5 postinoculation in BN rats inoculated with attenuated mengovirus compared with those inoculated with an equivalent amount of UV-inactivated vMC0 or vehicle (Figure 2; P < 0.05). Levels of BAL lymphocytes were also significantly elevated on day 1 postinoculation in vMC0-inoculated BN rats as compared with vehicle-inoculated rats (Figure 2; P < 0.05). No significant differences were observed among the vMC0-, UV-inactivated vMC0-, and vehicle-inoculated groups with regard to the numbers of BAL macrophages or eosinophils. Examination of Giemsa-stained lung sections revealed patchy peribronchial, perivascular, and alveolar cellular infiltrates in the lungs of BN rats inoculated with 107 PFU of vMC0 but not in those inoculated with vehicle or UV-inactivated vMC0 (Figure 3). These data demonstrate the development of a neutrophilic and lymphocytic lower airway inflammatory response in rats after inhalation of attenuated mengovirus, which required replication-competent virus.

Recruitment of neutrophils and lymphocytes to the lungs after inhalation of attenuated mengovirus. Numbers of (A) total cells, (B) neutrophils, (C) lymphocytes, (D) eosinophils, and (E) macrophages in the BAL fluid harvested on days 1, 3, and 5 postinoculation from the right lungs of BN rats inoculated with 107 PFU of vMC0 (n = 4, 10, and 4 rats, respectively) and on day 3 postinoculation from those inoculated with an equivalent amount of UV-inactivated vMC0 (n = 5 rats) or vehicle (n = 7 rats). Data are presented as box plots. * P < 0.05 (mengovirus vs. vehicle); † P < 0.05 (vMC0 vs. UV-inactivated vMC0).

Recruitment of inflammatory cell infiltrates to the lungs after inhalation of attenuated mengovirus. Giemsa-stained sections of the left lungs from BN rats inoculated with (A) vehicle, (B) vMC0 (107 PFU) or (C) an equivalent amount of UV-inactivated vMC0. Lungs were harvested on day 3 postinoculation. Magnification, 20×.
Expression of CXCR2 ligands in the lower airways after inhalation of attenuated mengovirus
Given the significant neutrophilia in the lower airways that was induced in BN rats by inhalation of vMC0, we examined the BAL fluid for the expression of the rat CXCR2 ligands, CINC-1 and MIP-2, which are neutrophil chemoattractants [27]. The BAL fluid levels of CINC-1 and MIP-2 were significantly elevated on days 1, 3, and 5 postinoculation in rats inoculated with 107 PFU of vMC0 as compared with those inoculated with vehicle or an equivalent amount of UV-inactivated vMC0 (Figure 4A and 4B; P ≤ 0.05).

Inhalation of attenuated mengovirus enhanced pulmonary expression of the chemokines, CINC-1, MIP-2, and MCP-1. BAL fluid was harvested on days 1, 3, and 5 postinoculation from the right lungs of BN rats inoculated with 107 PFU of vMC0 (n = 4, 10, and 4 rats, respectively) and on day 3 postinoculation from those inoculated with an equivalent amount of UV-inactivated vMC0 (n = 5 rats) or vehicle (n = 5–6 rats), and (A) CINC-1, (B) MIP-2, and (C) MCP-1 levels were determined by ELISA. Data are the total amount of chemokine recovered from the right lung BAL (ELISA values, corrected for the 15× concentration, were multiplied by the BAL fluid volume). (A, B) Data are presented as box plots. (C) Symbols represent data from individual rats; bars indicate medians. * P < 0.05, ‡ P = 0.05 (vMC0 vs. vehicle); † P < 0.05 (vMC0 vs. UV-inactivated vMC0).
Expression of MCP-1 in the lower airways after inhalation of attenuated mengovirus
Because HRV infection induces high levels of MCP-1 expression [28], and MCP-1 indirectly contributes to neutrophil recruitment to the lungs [29–32], we examined the BAL fluid from BN rats that had been inoculated with 107 PFU of vMC0 for MCP-1 expression. The levels of MCP-1 in BAL fluid were significantly increased on days 1 and 3 or day 3 postinoculation in vMC0-inoculated rats compared with vehicle- or UV-inactivated vMC0-inoculated rats, respectively (Figure 4C; P < 0.05). As shown with regard to CXCR2 ligand expression, UV-inactivation of vMC0 abrogated its ability to induce a significant elevation in BAL fluid MCP-1 levels, demonstrating the need for replication-competent virus.
Effect of inoculation dose on inflammatory response to inhalation of attenuated mengovirus
Inoculation with a ten-fold lower dose of vMC0 yielded a similar inflammatory response in the lower airways. Insufflation of 106 PFU of vMC0 into the lungs of BN rats (n = 4) induced a significant increase (P < 0.05) in the numbers [106 cells: median (interquartile range)] of neutrophils [0.19 (0.16, 0.21)] and lymphocytes [0.23 (0.20, 0.30)], but not total cells, eosinophils, or macrophages in the BAL fluid on day 3 postinoculation as compared with the values from vehicle-inoculated rats. In addition, the levels [pg: median (interquartile range)] of CINC-1 [715 (611, 835)], MIP-2 [188 (168, 208)], and MCP-1 [385 (266, 452)] in the BAL fluid were significantly elevated (P < 0.05) in these rats as compared with vehicle-inoculated controls. An inoculation dose of 105 PFU of vMC0 was substantially less effective at generating an inflammatory response in the lower airways of the rats, leading to the recruitment of about 75% fewer BAL neutrophils and 60% fewer BAL lymphocytes on day 3 postinoculation compared with that observed using inoculation doses of 107 or 106 PFU.
Effect of inhalation of attenuated mengovirus on pulmonary physiology and airway hyperresponsiveness (AHR)
To examine whether infection of the lower airways with attenuated mengovirus induced changes in pulmonary physiology, either vehicle or 107 PFU of vMC0 were insufflated into the lungs of adult BN rats, and pulmonary function was measured on day 3 postinoculation. No significant differences were observed between vehicle- and vMC0-inoculated groups of rats with regard to respiratory system resistance (Rrs) or the input impedance variables, Newtonian resistance (Rn), tissue viscance (G), and elastance (H), either at baseline or in response to methacholine challenge (Figure 5 and data not shown), indicating a lack of viral effects on pulmonary physiology and AHR.

Effect of inhalation of attenuated mengovirus on pulmonary physiology. BN rats were inoculated with either vehicle or 107 PFU of vMC0 (n = 5 rats per group), and on day 3 postinoculation, pulmonary physiology measurements were obtained after exposure to aerosols of normal saline followed by escalating concentrations of methacholine. Values for respiratory system resistance (Rrs) are presented as the group means ± the standard error. There were no significant differences between the vehicle- and vMC0-inoculated groups.
Discussion
The establishment of useful small animal models to study HRV pathogenesis has been an important goal to enable mechanistic studies and facilitate the development of new therapies. The earliest reported effort to develop a HRV infection model in mice required very large input doses of virus and pretreatment of the mice with actinomycin D [33]. Recently, more robust murine experimental models of HRV infection have been established. These models employ either a murine cell culture-adapted minor group HRV in wild-type mice or a major group HRV in mice that are transgenic for human ICAM-1 [18, 19]. Although the development of these novel tools represents a significant advance in the study of HRV-induced airway inflammation, an important limitation is that HRV shedding is limited to ≤ 24 h postinoculation [18].
In the rat model described here, infectious mengovirus was consistently detected in the lungs at high levels, and persisted for at least 3 days after inoculation. The inoculation dose of 106–107 PFU of attenuated mengovirus in the rats was similar to the dose of 5 × 106 TCID50 (50% tissue-culture infective dose) administered in the HRV models in mice [18, 19], especially considering that the body weight of the rats is about an order of magnitude greater compared to that of mice. Furthermore, inhalation of attenuated mengovirus, but not vehicle or UV-inactivated virus, into the lungs of BN rats resulted in increases in chemokines (CINC-1, MIP-2, and MCP-1) and cellular inflammation (neutrophils, lymphocytes, and total BAL cells). Compared to the HRV mouse models, infection with vMC0 represents a rodent model of picornavirus-induced airway inflammation in which the roles of viral replication and persistence are more prominent.
Mengovirus-induced expression of CXCR2 ligands is consistent with the increased expression of CXCR2 ligands that is observed in response to rhinovirus infection [34–36]. A similar induction of CXCR2 ligands was also observed in the murine HRV infection models [18, 19]. We also observed the induction of MCP-1 expression in response to inhalation of attenuated mengovirus, which represents another similarity between this rat model of attenuated mengovirus-induced airway inflammation and human host responses to HRV infection [28]. Therefore, the induction of rat CXC2 ligand and MCP-1 expression in airway fluids in response to inhalation of attenuated mengovirus closely resembles the HRV-induced enhancement of these chemokines.
Another similarity between this rat model and HRV infection in humans is the relative kinetics of the viral infection vs. the lower airway neutrophilic inflammatory response. Mengovirus titers in the lung peak earlier than the neutrophilic inflammatory response in the lower airways. This parallels data from experimental HRV inoculations in human volunteers [11, 13]. In addition, the patchiness of the mengovirus-induced airway inflammation in this rat model is consistent with the patchy infection of airway epithelial cells observed in HRV infections in human subjects [11, 37–39].
Infection of the lower airways with mengovirus did not result in significant changes in baseline pulmonary physiology measurements or in AHR to methacholine challenge in this rat model. It is important to note that experimentally naïve adult rats without existing airway disease were used in these studies. Similar to this rat model, several studies involving experimental HRV inoculations of healthy, nonasthmatic, nonallergic human subjects have demonstrated no changes in baseline pulmonary function or AHR after HRV infection [10, 40–44]. In one study showing a small change in AHR after experimental HRV infection of nonasthmatic, nonallergic subjects, the small difference was only detected by employing a methacholine concentration that was a half-log higher than the highest concentration typically used [45]. In contrast, experimental inoculation with HRV has been shown to increase AHR in individuals with asthma and/or allergic rhinitis in several studies [10, 17, 44, 46, 47], although not in others [40, 41, 43, 45, 48]. Therefore, the absence of changes in AHR in these healthy adult rats without existing airway disease is consistent with the outcomes of experimental HRV infections in healthy humans who had no underlying airway disease, such as asthma or allergic rhinitis. The absence of viral effects on AHR in this mengovirus model and in the experimental HRV inoculations in humans is consistent with the murine experimental model of HRV infection described by Bartlett et al. in which there was no increase in AHR to methacholine challenge after HRV infection unless the BALB/c mice had also been sensitized and challenged with allergen [18]. However, in the murine experimental HRV infection model described by Newcomb et al., an increase in AHR to methacholine challenge was observed after infection of C57BL/6 mice with HRV [19], which may be related to the use of a different mouse strain. Overall, the lack of significant changes in pulmonary physiology during mengovirus-induced respiratory infection in adult rats without existing airway disease is consistent with previous observations in experimental HRV infections in humans. In future studies, it will be of interest to investigate the effects of mengovirus-induced respiratory infection on rats with existing airway injury related to prior exposures to allergens or other respiratory viruses [49] with the objective of modeling aspects of HRV-induced asthma exacerbations.
A potential limitation of this animal model is the use of mengovirus, which is neurotropic, to serve as a model for HRV, which primarily causes respiratory infections. In this regard, it is important to note that poliovirus, which is closely related to HRV, is also neurotropic. The attenuated mengovirus, vMC0, used in these studies induced a self-limited respiratory infection when administered through an inhalation route. This indicates that there is plasticity in the tissue tropism of vMC0 that makes it suitable for a model of picornavirus-induced airway infection and inflammation. Another consideration is that there are both similarities and differences in CXCR2 and its ligands between rats and humans [50]. Humans express IL-8 and two IL-8 receptors, CXCR1 and CXCR2, whereas rats do not express an IL-8 ortholog and only express CXCR2. However, rats do express relevant CXCR2 ligands, such as CINC-1 and MIP-2, which are functional analogs of IL-8 with regard to neutrophil recruitment and activation. We believe that the rat represents an attractive, relevant, and simplified model for examining the role of CXC chemokines in neutrophil recruitment and activation in response to picornavirus-induced respiratory infection because of the reduced number of chemokines and chemokine receptors to be examined.
Conclusion
Overall, our data support the feasibility of using this novel rat model of picornavirus-induced lower airway infection and inflammation to study, among other questions, the role of neutrophilic inflammation in the host response to picornavirus-induced respiratory infections. Although this model does not fully encompass all aspects of HRV infection in humans, it does demonstrate a remarkable number of parallel developments that will provide novel opportunities to study the interactions between picornaviral replication and the host antiviral immune responses in a relevant small animal model.
Methods
Animals
BN/SsN male rats were purchased from Harlan (Indianapolis, IN) and had a median body weight of 250 g when used for inoculation studies. The rats were housed in HEPA-filtered isolation cubicles (Britz and Co., Wheatland, WY) in an American Association for Accreditation of Laboratory Animal Care-accredited laboratory animal facility at the University of Wisconsin School of Medicine and Public Health. All procedures were approved by the University of Wisconsin Animal Care and Use Committee and conformed to the Guide for the Care and Use of Laboratory Animals (1996).
Virus
Stock preparations of the attenuated mengovirus, vMC0 (which has no poly(C) tract) [21–25], were prepared by transfection of HeLa cells with viral RNA transcribed from a plasmid encoding the vMC0 genome followed by amplification of viral titers via passage in HeLa cell cultures as described [51]. Supernates from uninfected HeLa cell cultures were used as vehicle controls, and UV-inactivated vMC0 stocks were prepared by exposing vMC0 to a germicidal UV lamp at a distance of 10 cm for 1 h. Plaque assays using HeLa cells were employed to determine the titer of the active virus preparations and to verify UV-inactivation. Active virus was undetectable (< 10 PFU/ml) in the UV-inactivated preparations.
Virus inoculation
Rats were lightly anesthetized by inhalation of 5% isoflurane, and vMC0, UV-inactivated vMC0, or vehicle in a total volume of 0.1 ml were insufflated into the lungs via an orotracheal catheter.
Measurements of pulmonary inflammation
At various times after inoculation, rats were anesthetized with urethane and euthanized by exsanguination. The chest was opened, and the left mainstem bronchus was clamped to allow BAL of the right lung. The right lung was filled with phosphate buffered saline (PBS) to total lung capacity by gravity and drained 5 times, the BAL fluid was centrifuged, and the cell pellet was resuspended in 1 ml PBS. The total number of BAL leukocytes was determined with an automated cell counter (model Z1, Beckman Coulter, Hialeah, FL), and cytospin slides were prepared for a differential leukocyte count based on 200 cells. BAL fluid was concentrated 15× using a centrifugal filter device with a molecular weight cutoff of 5,000 (Millipore, Bedford, MA) and stored at -80°C until analyzed for chemokine expression. Samples of unconcentrated BAL fluid were used for viral titer determinations. The left lung was either removed for viral titer determinations or filled to total lung capacity by gravity with 10% buffered formalin for histological analysis.
Measurements of pulmonary physiology
Rats were anesthetized with pentobarbital (Abbott, North Chicago, IL), intubated via tracheostomy, paralyzed with succinylcholine HCl (Sigma, St. Louis, MO), and ventilated mechanically (flexiVent, SCIREQ, Montreal, Canada). Aerosol challenges were delivered by the ventilator via an inline nebulizer (Aeroneb, SCIREQ) as 10 breaths of aerosolized normal saline, followed by methacholine HCl (Sigma) solutions in concentrations of 0.1, 0.3, 1, 3, and 10 mg/ml. Each challenge was preceded by two lung inflations to 30 cmH2O, and the challenges were delivered every 4 min. After each aerosol challenge, measurements of pulmonary physiology were performed by the flexiVent system every 15 s for 2 min, alternating measures of Rrs with measures of input impedance variables (Rn, G, and H). For each variable, the highest value occurring after each aerosol challenge was recorded as the response, referenced to the value obtained after saline challenge.
Measurement of viral titers
Viral titers in left lung homogenates, prepared in PBS (10% w/v) and clarified by centrifugation, and in unconcentrated BAL fluid were determined by plaque assay using HeLa cells as described [24, 51]. Briefly, HeLa cell monolayers were inoculated with dilutions of the samples, incubated for 24–48 h at 37°C (until plaques form), formalin fixed, stained with crystal violet, and scored for plaques. Stock vMC0 preparations served as the positive control.
Histological assessment of pulmonary inflammation
Sections (5 μM) were prepared from formalin-fixed, paraffin-embedded left lungs. Giemsa staining was performed on these sections, which were evaluated for inflammation by light microscopy.
Measurement of chemokine expression
Chemokine levels in BAL fluid were determined using commercially available rat-specific enzyme-linked immunosorbent assay (ELISA) kits for CINC-1 (R&D Systems, Minneapolis, MN), MIP-2, and MCP-1 (Biosource, Camarillo, CA) with sensitivities of 7.8, 7.8, and 8 pg/ml, respectively, according to the manufacturers' instructions.
Statistical analysis
Analysis of variance (general linear model) was performed on the BAL fluid CINC-1 and MIP-2 ELISA data and on pulmonary physiology data after a log transformation, and Fischer's least significant difference test was used for planned pairwise comparisons. A residual analysis was employed to test the adequacy of the models. Nonparametric tests were used to analyze all other data. For comparisons between two groups, the Mann-Whitney test was used. The Kruskal-Wallis test was used for comparisons among three or more groups and was followed by planned pairwise comparisons using the Mann-Whitney test. Because infectious virus was undetectable in the lung homogenate and BAL fluid samples from rats inoculated with vehicle or UV-inactivated virus, these groups were combined for statistical analysis of viral titers. Box plots depict the median and the interquartile range between the 25th and 75th percentile, and whiskers show the 10th and 90th percentiles. Analyses were performed using the statistical software package SYSTAT 11.0 (Systat Software, Chicago, IL).
References
Lemanske RF Jr, Jackson DJ, Gangnon RE, Evans MD, Li Z, Shult PA, Kirk CJ, Reisdorf E, Roberg KA, Anderson EL, Carlson-Dakes KT, Adler KJ, Gilbertson-White S, Pappas TE, DaSilva DF, Tisler CJ, Gern JE: Rhinovirus illnesses during infancy predict subsequent childhood wheezing. J Allergy Clin Immunol 2005, 116: 571-577. 10.1016/j.jaci.2005.06.024
Jackson DJ, Gangnon RE, Evans MD, Roberg KA, Anderson EL, Pappas TE, Printz MC, Lee WM, Shult PA, Reisdorf E, Carlson-Dakes KT, Salazar LP, DaSilva DF, Tisler CJ, Gern JE, Lemanske RF Jr: Wheezing rhinovirus illnesses in early life predict asthma development in high-riskchildren. Am J Respir Crit Care Med 2008, 178: 667-672. 10.1164/rccm.200802-309OC
Kusel MM, de Klerk NH, Kebadze T, Vohma V, Holt PG, Johnston SL, Sly PD: Early-life respiratory viral infections, atopic sensitization, and risk of subsequent development of persistent asthma. J Allergy Clin Immunol 2007, 119: 1105-1110. 10.1016/j.jaci.2006.12.669
Kelly JT, Busse WW: Host immune responses to rhinovirus: mechanisms in asthma. J Allergy Clin Immunol 2008, 122: 671-682. 10.1016/j.jaci.2008.08.013
Singh AM, Moore PE, Gern JE, Lemanske RF Jr, Hartert TV: Bronchiolitis to asthma: a review and call for studies of gene-virus interactions in asthma causation. Am J Respir Crit Care Med 2007, 175: 108-119. 10.1164/rccm.200603-435PP
Gern JE, Galagan DM, Jarjour NN, Dick EC, Busse WW: Detection of rhinovirus RNA in lower airway cells during experimentally induced infection. Am J Respir Crit Care Med 1997, 155: 1159-1161.
Papadopoulos NG, Bates PJ, Bardin PG, Papi A, Leir SH, Fraenkel DJ, Meyer J, Lackie PM, Sanderson G, Holgate ST, Johnston SL: Rhinoviruses infect the lower airways. J Infect Dis 2000, 181: 1875-1884. 10.1086/315513
Mosser AG, Brockman-Schneider R, Amineva S, Burchell L, Sedgwick JB, Busse WW, Gern JE: Similar frequency of rhinovirus-infectible cells in upper and lower airway epithelium. J Infect Dis 2002, 185: 734-743. 10.1086/339339
Schroth MK, Grimm E, Frindt P, Galagan DM, Konno SI, Love R, Gern JE: Rhinovirus replication causes RANTES production in primary bronchial epithelial cells. Am J Respir Cell Mol Biol 1999, 20: 1220-1228.
Message SD, Laza-Stanca V, Mallia P, Parker HL, Zhu J, Kebadze T, Contoli M, Sanderson G, Kon OM, Papi A, Jeffery PK, Stanciu LA, Johnston SL: Rhinovirus-induced lower respiratory illness is increased in asthma and related to virus load and Th1/2 cytokine and IL-10 production. Proc Natl Acad Sci USA 2008, 105: 13562-13567. 10.1073/pnas.0804181105
Mosser AG, Vrtis R, Burchell L, Lee WM, Dick CR, Weisshaar E, Bock D, Swenson CA, Cornwell RD, Meyer KC, Jarjour NN, Busse WW, Gern JE: Quantitative and qualitative analysis of rhinovirus infection in bronchial tissues. Am J Respir Crit Care Med 2005, 171: 645-651. 10.1164/rccm.200407-970OC
Jarjour NN, Gern JE, Kelly EA, Swenson CA, Dick CR, Busse WW: The effect of an experimental rhinovirus 16 infection on bronchial lavageneutrophils. J Allergy Clin Immunol 2000, 105: 1169-1177. 10.1067/mai.2000.106376
Gern JE, Vrtis R, Grindle KA, Swenson C, Busse WW: Relationship of upper and lower airway cytokines to outcome of experimental rhinovirusinfection. Am J Respir Crit Care Med 2000, 162: 2226-2231.
Fahy JV, Kim KW, Liu J, Boushey HA: Prominent neutrophilic inflammation in sputum from subjects with asthma exacerbation. J Allergy Clin Immunol 1995, 95: 843-852. 10.1016/S0091-6749(95)70128-1
Wark PA, Johnston SL, Moric I, Simpson JL, Hensley MJ, Gibson PG: Neutrophil degranulation and cell lysis is associated with clinical severity in virus-induced asthma. Eur Respir J 2002, 19: 68-75. 10.1183/09031936.02.00226302
Gern JE, Martin MS, Anklam KA, Shen K, Roberg KA, Carlson-Dakes KT, Adler K, Gilbertson-White S, Hamilton R, Shult PA, Kirk CJ, Da Silva DF, Sund SA, Kosorok MR, Lemanske RF Jr: Relationships among specific viral pathogens, virus-induced interleukin-8, and respiratory symptoms in infancy. Pediatr Allergy Immunol 2002, 13: 386-393. 10.1034/j.1399-3038.2002.01093.x
Grunberg K, Timmers MC, Smits HH, de Klerk EP, Dick EC, Spaan WJ, Hiemstra PS, Sterk PJ: Effect of experimental rhinovirus 16 colds on airway hyperresponsiveness to histamine and interleukin-8 in nasal lavage in asthmatic subjects in vivo. Clin Exp Allergy 1997, 27: 36-45. 10.1111/j.1365-2222.1997.tb00670.x
Bartlett NW, Walton RP, Edwards MR, Aniscenko J, Caramori G, Zhu J, Glanville N, Choy KJ, Jourdan P, Burnet J, Tuthill TJ, Pedrick MS, Hurle MJ, Plumpton C, Sharp NA, Bussell JN, Swallow DM, Schwarze J, Guy B, Almond JW, Jeffery PK, Lloyd CM, Papi A, Killington RA, Rowlands DJ, Blair ED, Clarke NJ, Johnston SL: Mouse models of rhinovirus-induced disease and exacerbation of allergic airway inflammation. Nat Med 2008, 14: 199-204. 10.1038/nm1713
Newcomb DC, Sajjan US, Nagarkar DR, Wang Q, Nanua S, Zhou Y, McHenry CL, Hennrick KT, Tsai WC, Bentley JK, Lukacs NW, Johnston SL, Hershenson MB: Human rhinovirus 1B exposure induces phosphatidylinositol 3-kinase-dependent airway inflammation in mice. Am J Respir Crit Care Med 2008, 177: 1111-1121. 10.1164/rccm.200708-1243OC
Palmenberg AC, Osorio JE: Cardioviral poly(C) tracts and viral pathogenesis. Arch Virol Suppl 1994, 9: 67-77.
Duke GM, Osorio JE, Palmenberg AC: Attenuation of Mengo virus through genetic engineering of the 5' noncoding poly(C) tract. Nature 1990, 343: 474-476. 10.1038/343474a0
Martin LR, Duke GM, Osorio JE, Hall DJ, Palmenberg AC: Mutational analysis of the mengovirus poly(C) tract and surrounding heteropolymeric sequences. J Virol 1996, 70: 2027-2031.
Osorio JE, Grossberg SE, Palmenberg AC: Characterization of genetically engineered mengoviruses in mice. Viral Immunol 2000, 13: 27-35. 10.1089/vim.2000.13.27
Osorio JE, Martin LR, Palmenberg AC: The immunogenic and pathogenic potential of short poly(C) tract Mengo viruses. Virology 1996, 223: 344-350. 10.1006/viro.1996.0485
Martin LR, Neal ZC, McBride MS, Palmenberg AC: Mengovirus and encephalomyocarditis virus poly(C) tract lengths can affect virus growth in murine cell culture. J Virol 2000, 74: 3074-3081. 10.1128/JVI.74.7.3074-3081.2000
Sorkness RL, Castleman WL, Kumar A, Kaplan MR, Lemanske RF Jr: Prevention of chronic post-bronchiolitis airway sequelae with interferon-γ treatment in rats. Am J Respir Crit Care Med 1999, 160: 705-710.
Shibata F, Konishi K, Kato H, Komorita N, Al-Mokdad M, Fujioka M, Nakagawa H: Recombinant production and biological properties of rat cytokine-induced neutrophil chemoattractants, GRO/CINC-2 alpha, CINC-2 beta and CINC-3. Eur J Biochem 1995, 231: 306-311. 10.1111/j.1432-1033.1995.tb20701.x
Hall DJ, Bates ME, Guar L, Cronan M, Korpi N, Bertics PJ: The role of p38 MAPK in rhinovirus-induced monocyte chemoattractant protein-1 production by monocytic-lineage cells. J Immunol 2005, 174: 8056-8063.
Gonzalo JA, Lloyd CM, Wen D, Albar JP, Wells TN, Proudfoot A, Martinez A, Dorf M, Bjerke T, Coyle AJ, Gutierrez-Ramos JC: The coordinated action of CC chemokines in the lung orchestrates allergic inflammation and airway hyperresponsiveness. J Exp Med 1998, 188: 157-167. 10.1084/jem.188.1.157
Maus U, von GK, Kuziel WA, Mack M, Miller EJ, Cihak J, Stangassinger M, Maus R, Schlondorff D, Seeger W, Lohmeyer J: The role of CC chemokine receptor 2 in alveolar monocyte and neutrophil immigration in intactmice. Am J Respir Crit Care Med 2002, 166: 268-273. 10.1164/rccm.2112012
Maus UA, Waelsch K, Kuziel WA, Delbeck T, Mack M, Blackwell TS, Christman JW, Schlondorff D, Seeger W, Lohmeyer J: Monocytes are potent facilitators of alveolar neutrophil emigration during lung inflammation: role of the CCL2-CCR2 axis. J Immunol 2003, 170: 3273-3278.
Vozzelli MA, Mason SN, Whorton MH, Auten RL Jr: Antimacrophage chemokine treatment prevents neutrophil and macrophage influx in hyperoxia-exposed newborn rat lung. Am J Physiol Lung Cell Mol Physiol 2004, 286: L488-L493. 10.1152/ajplung.00414.2002
Yin FH, Lomax NB: Establishment of a mouse model for human rhinovirus infection. J Gen Virol 1986, 67: 2335-2340. 10.1099/0022-1317-67-11-2335
Zhu Z, Tang W, Gwaltney JM Jr, Wu Y, Elias JA: Rhinovirus stimulation of interleukin-8 in vivo and in vitro: role of NF-kappaB. Am J Physiol 1997, 273: L814-L824.
Subauste MC, Jacoby DB, Richards S, Proud D: Infection of a human respiratory epithelial cell line with rhinovirus. Induction of cytokine release and modulation of susceptibility to infection by cytokineexposure. J Clin Invest 1995, 96: 549-557. 10.1172/JCI118067
Donninger H, Glashoff R, Haitchi HM, Syce JA, Ghildyal R, van RE, Bardin PG: Rhinovirus induction of the CXC chemokine epithelial-neutrophil activating peptide-78 in bronchial epithelium. J Infect Dis 2003, 187: 1809-1817. 10.1086/375246
Arruda E, Boyle TR, Winther B, Pevear DC, Gwaltney JM Jr, Hayden FG: Localization of human rhinovirus replication in the upper respiratory tract by in situ hybridization. J Infect Dis 1995, 171: 1329-1333.
Pitkaranta A, Puhakka T, Makela MJ, Ruuskanen O, Carpen O, Vaheri A: Detection of rhinovirus RNA in middle turbinate of patients with common colds by in situ hybridization. J Med Virol 2003, 70: 319-323. 10.1002/jmv.10397
Winther B, Gwaltney JM Jr, Mygind N, Turner RB, Hendley JO: Sites of rhinovirus recovery after point inoculation of the upper airway. JAMA 1986, 256: 1763-1767. 10.1001/jama.256.13.1763
Skoner DP, Doyle WJ, Seroky J, Vandeusen MA, Fireman P: Lower airway responses to rhinovirus 39 in healthy allergic and nonallergicsubjects. Eur Respir J 1996, 9: 1402-1406. 10.1183/09031936.96.09071402
Zambrano JC, Carper HT, Rakes GP, Patrie J, Murphy DD, Platts-Mills TA, Hayden FG, Gwaltney JM Jr, Hatley TK, Owens AM, Heymann PW: Experimental rhinovirus challenges in adults with mild asthma: Response to infection in relation to IgE. J Allergy Clin Immunol 2003, 111: 1008-1016. 10.1067/mai.2003.1396
de Kluiver J, Grunberg K, Sont JK, Hoogeveen M, van Schadewijk WA, de Klerk EP, Dick CR, van Krieken JH, Sterk PJ: Rhinovirus infection in nonasthmatic subjects: effects on intrapulmonary airways. Eur Respir J 2002, 20: 274-279. 10.1183/09031936.02.00247202
Angelini B, Van Deusen MA, Doyle WJ, Seroky J, Cohen S, Skoner DP: Lower airway responses to rhinovirus-Hanks in healthy subjects with and without allergy. J Allergy Clin Immunol 1997, 99: 618-619. 10.1016/S0091-6749(97)70022-8
Gern JE, Calhoun W, Swenson C, Shen G, Busse WW: Rhinovirus infection preferentially increases lower airway responsiveness in allergicsubjects. Am J Respir Crit Care Med 1997, 155: 1872-1876.
Fleming HE, Little FF, Schnurr D, Avila PC, Wong H, Liu J, Yagi S, Boushey HA: Rhinovirus-16 colds in healthy and in asthmatic subjects: similar changes in upper and lower airways. Am J Respir Crit Care Med 1999, 160: 100-108.
Lemanske RF Jr, Dick EC, Swenson CA, Vrtis RF, Busse WW: Rhinovirus upper respiratory infection increases airway hyperreactivity and late asthmatic reactions. J Clin Invest 1989, 83: 1-10. 10.1172/JCI113843
de Gouw HW, Grunberg K, Schot R, Kroes AC, Dick EC, Sterk PJ: Relationship between exhaled nitric oxide and airway hyperresponsiveness following experimental rhinovirus infection in asthmatic subjects. Eur Respir J 1998, 11: 126-132. 10.1183/09031936.98.11010126
Avila PC, Abisheganaden J, Wong H, Liu J, Yagi S, Schnurr D, Kishiyama JL, Boushey HA: Effects of allergic inflammation of the nasal mucosa on the severity of rhinovirus 16 cold. J Allergy Clin Immunol 2000, 105: 923-932. 10.1067/mai.2000.106214
Sorkness RL, Herricks KM, Szakaly RJ, Lemanske RF Jr, Rosenthal LA: Altered allergen-induced eosinophil trafficking and physiological dysfunction in airways with preexisting virus-induced injury. Am J Physiol Lung Cell Mol Physiol 2007, 292: L85-L91. 10.1152/ajplung.00234.2006
Roth I, Hebert C: CXCR1 and CXCR2. In Cytokine Reference: a Compendium of Cytokines and Other Mediators of Host Defense. Edited by: Oppenheim JJ, Feldman M. San Diego: Academic Press; 2001:1982-2002.
Amineva SP, Mosser AG, Binder JJ, Aminev AG, Palmenberg AC, Gern JE: Synthesis of the allergen ovomucoid by a replicating Mengo virus. Arch Virol 2006, 151: 1933-1946. 10.1007/s00705-006-0778-z
Acknowledgements
The authors thank Dr. Ann Palmenberg (The Institute for Molecular Virology, University of Wisconsin-Madison) for generously providing the plasmid containing the attenuated mengovirus, vMC0, and for helpful discussions. We also thank Maria Bulat and LaCinda Burchell for technical assistance with the virology and histology studies, respectively. This work was funded by National Institutes of Health grants AI070503 to LAR and JEG and AI50500 to RFL.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
LAR co-conceived the study, designed and coordinated the experiments, participated in the animal and immunological studies, performed the data and statistical analysis, analyzed and interpreted the data, and drafted the manuscript. SPA carried out the virology studies and participated in the experimental design and interpretation of the data. RJS carried out the animal, immunological, and histological studies and participated in the interpretation of the data. RFL participated in the interpretation of the data and revision of the manuscript. JEG co-conceived the study and participated in the interpretation of the data and revision of the manuscript. RLS co-conceived the study and participated in the experimental design, the animal and immunological studies, the interpretation of the data, and the revision of the manuscript. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Rosenthal, L.A., Amineva, S.P., Szakaly, R.J. et al. A rat model of picornavirus-induced airway infection and inflammation. Virol J 6, 122 (2009). https://doi.org/10.1186/1743-422X-6-122
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1743-422X-6-122