
Abstract
The pandemic being a health issue at its core is a multifaceted crisis encompassing both economic and epidemic factors in a twisted tale of challenges. In counteraction, we have proposed a combined epidemic–economic model that analyses system dynamics arising in the presence of an infectious disease (SARS-2-COVID-19 in our case). Dynamical analysis of the system has been performed in context to the equilibria along with local and global stability analysis of the system simultaneously visualizing the effect on capital stabilization. The global stability analysis has been performed using graph-theoretic method. Curve-Fit has been performed for the system using optimization algorithm. The relation between all the parameters and variables involved in the model has been explored by calculating sensitivity indices which gives us the proportion that a relative change in a parameter brings to the relative change in a variable. Our findings reveal that (1) Vaccination instigates economic growth (with evidence of data obtained for 24 countries). (2) Complete vaccination leads to a considerable reduction in all infections (reduction up to 90%, as per current CDC study). (3) Excessive exposure to media can facilitate spike in infections. (4) Parameter sensitivity analysis can be of immense help in policy formation.
Similar content being viewed by others


1 Introduction
The economy in any country is an ecosystem in which goods and services, demand and supply, money market, capital stock, production, national income, and savings are all connected and dependent on each other through multifarious channels. Natural calamities, such as famines, droughts, floods, earthquakes, pest invasions, and disease outbreaks, are detrimental to the economy no matter the level at which they occur. The ongoing pandemic has shrunken economies all across the globe including India. In the presence of an infectious disease, such as the current SARS-2-COVID 19 virus, the economy is bound to suffer setbacks. We have plethora of information on how various industries have been hit including but not limited to imports and exports, aviation industry, tourism industry, oil prices, meat processing sector, construction sector, forest sector, public services and overseas employment, etc. The novel coronavirus will make the world pay approximately between 16 trillion and 35 trillion dollars by 2025 [1]. Economic models are rolling out figures pertaining to various domains, assessing the impact of the pandemic financially but with no direct relationship to infection rates or natural recoveries. Killing more than 4 million people globally [2], the virus continues to invades the lives of people, affecting billions of masses. Again, epidemic models [3,4,5,6] can address the spread of infection, mortality, morbidity, recoveries, and role of vaccinations, but cannot contribute directly for analysing economic damage/possible recovery. The pandemic being a health issue at its core is a multifaceted crisis [7] encompassing both economic and epidemic factors in a twisted tale of challenges like capacity constraints in form of reduced labor due to infections, supply-chain disruptions due to partial and complete lock downs, and competition for global influence in form of effective vaccines [1]. Addressing former issues, a combined epidemic–economic model can act as a lodestar to not only analyse economy v/s infections but to make effective forecasts imbibing both financial and health factors in direct relationship with each other. This proposed piece of research in a novel attempt encapsulates this effort wherein we have analysed an ‘epidemic–economic’ model in the presence of novel corona virus infection with the intent of exploring the threads between capital stabilization and the role of vaccine. We have populated the basic SIR model with two vaccinated classes \(V_1\) and \(V_2\) and the resulting SIVR model has been combined with Solow’s model of economic growth pertaining to evolution of capital stock.
1.1 Vaccination and economic growth: an underestimated relationship
Prima facie, the pandemic hits as a serious health crisis. Though months into it, the economic damage arising out of it was enough to drop world’s GDP (gross domestic product) by 4.6% in 2020 as per inputs from Bureau of Economic Analysis. SARS-COVID-2 has affected the world through multifarious channels, and hence, there have been multitude of studies into it. Ranging from in-depth analysis of the latest variant [8] to the recurrent waves of infection [9, 10] and achieving herd immunity [11], there have been humongous efforts all across the globe to curb this pandemic. In the absence of a permanent cure, our hope to sustain this infectious catastrophe lies purely on physical distancing, mask practice, robust monitoring, herd immunity, and vaccination. Vaccination, unabatedly, is a significant part of the multi-factorial public health system and imbibes ardent potential for bringing down the pandemic. Researchers, scientists, and medical fraternity all across the globe are making humongous efforts to develop cost-effective vaccines that can target the virus and its mutations. Presently, more than 200 vaccines are being developed with two dozen of them being authorized for use [12]. As of November 10 2021, 51.1% population has received at least one dose [13]. Worldwide, 7.31 billion doses have been administered as of November 10 2021, with 27.36 million being administered daily [13].
Our work revolves around studying the impact of vaccinated classes, primarily on capital stock and how the various epidemic and economic variables and parameters are related to each other. The alma matter on the relation between vaccination and economic growth has delivered important insights. Researchers in [14] have analyzed the connectivity between HDI (Human Development Index) and GDP (macro-socioeconomic measures) and SARS-COVID-2 vaccine distribution based on data from 25 countries (data as on first week of February 2021). Findings reveal that higher GDP per capita associates with higher number of vaccinations and HDI does not follow the same. Authors in [15] have shed light on vaccine nationalism through statistical data and have portrayed its impact on world’s economy pertaining to four scenarios, i.e., no vaccination at all, only vaccine producing nations have vaccine, all high income and vaccine producing nations have vaccine, and all high and middle income and vaccine producing nations have vaccine. Conclusion arised that spending on vaccine allocation and development by leading economies is relatively trifle in comparison to the economic loss that incurs, while the latter is ignored. Data-driven research [14, 15] maintains the stand on COVID-19 vaccination adding to economic growth, National or Worldwide. However, the findings do not imbibe any model for correlation or improvement. Given the audacity vaccines are being reported to posses to curb, if not extinct, the ongoing pandemic often leads to a stinging question. Will vaccination end the pandemic? Prominent research [16] dares to answer affirmative, though ‘when’ and ‘how’ have been reported to be dependent on vaccine availability, accessibility, and vaccination rates. This work [16] takes a dig at whether vaccination can end the SARS-COVID-2 infection while taking into account accessibility and availability of vaccines and vaccination rates. Taking case example from one developed country (United States) and one developing country (Indonesia), the work propagates that vaccines imbibe ardent potential to annihilate SARS-COVID-2 infection. Establishing positive correlation between COVID-19 vaccination rates and GDP per capita [17], the research uses Spearman’s correlation analysis to examine the strength and direction of association between GDP per capita and SARS-COVID-2 vaccination rates across 46 countries (data as on 12 January 2021). Findings reveal that countries having high vaccination rates had higher GDP per capita. All of the aforementioned works have established prominent results based on statistics alone without any involving mathematical model. Data-driven studies depend heavily on the source and quality of data imported; hence, even minor discrepancies can alter results and claims made through them. Mathematical models add weight and credibility to the research in broadly two ways. First being, that the model can be subjected to various data sets leading to versatile possible outcomes and thus providing better insights and forecasts rather than specific results rolling out from a single data set. Second, modelling complex situations like that of the ongoing pandemic always have a room for improvement in the form of adding/removing parameters and understanding how the increase/decrease in one parameter can affect the outcomes of the model. This cannot be done in the case of data-driven research.
Model-based research in this arena is sparse and there are very few works to quote. Authors [18] talk about macroeconomic gains as a result of increased vaccination rates using DTP vaccine as a proxy for the study. Their results talk about reduced public health improvements and economic benefits as the investment in vaccinations is reduced. This research covers general vaccination approach in a pre-pandemic world and does not include the ongoing pandemic and its effects in any manner. In another prominent work [19], an augmented epidemic–economic with two time delays is investigated for hopf bifurcation in presence of an infectious disease. Stability of disease free and endemic equilibrium points has been explored. Their results propagate that local stability corresponding to the endemic equilibrium point relies on \(R_0\) and on latent period (time delay \(\tau _2\)), whereas the first delay (Kalecki’s time delay \(\tau _1\)) does not make a significant difference to model behaviour. However, the model does not include vaccinated class in any capacity nor does it discusses the role of vaccination in uplifting the economy.
1.1.1 Novelty and goal of the paper
There is a paucity of macroeconomic assessment of vaccines that extensively investigates how population saved can affect government expenditure on education, health, and future tax receipts, contribute to capital stabilization, and aid in growing GDP [20]. Our proposed model captures this gap at heart and places the macroeconomic valuation of vaccines at an exposition where public health benefit can translate into remarkable economic activity. In layman terms, the major intent in this research is to study the impact of vaccination on capital stock, i.e., the impact of \(V_{1}\) and \(V_{2}\) on K. To the best of our knowledge, the proposed epidemic–economic model involving two vaccinated classes is a first of its kind. So far, only data [14,15,16] have been available to check an increasing/decreasing economic activity with an increasing/decreasing vaccination rate or roll out. A model-based approach and analysis to evaluate the impact of vaccination on the economy (capital stock) has not been attempted so far. Our work has made an attempt in this direction, and clearly, it is in a position to demonstrate how an increment/decrement in infections, transmission rate, recovery rate, death rate, media, and rate of vaccination can modulate economic growth (capital stock). Mentioned below are the goals of this research work and these aspects have not been explored before in the context of the proposed \(K, S, I, V_{1}, V_{2}, R\) model:
-
Exploring the calibre of vaccination in promoting economic growth globally. Can vaccination act as a lodestar for improved economic figures (can capital stock ‘K’ be instigated as the vaccinated class ‘\(V_{1}\)’ increases)?
-
How does the infected class respond to complete vaccination (relation between infected class I and vaccinated class \(V_{2}\))?
-
The global consociation of media and the pandemic. How is the media affecting infected and susceptible classes (how parameter ‘m’ affects infected class I and susceptible class S?
-
The association of epidemic–economic parameters, i.e., \(N,\sigma , A, \alpha , \delta , \mu , p, p_{1}, p_{2}, b_{1}, \gamma , \psi \) and m with capital stock, susceptible class, infected class, vaccinated classes (both), and the recovered class. What is the degree of relationship, if there exist any, between them?
The analysis has been performed with data sourced from www.mygov.in/covid-19 (rates of vaccination, recovery, and infections, data as on June 19 2021) and thus provide room for realistic dynamics around the pandemic. We have compared the results obtained from our model with original data on GDP and vaccination percentage facilitating evidence for proposed work. Also, a curve fit using optimization algorithm has been performed to fit our system with the help of the initial conditions and the parametric values.
The stratification of the paper is as follows. Section 2 comprises of mathematical model formulation and the questions addressed by this piece of research. Model dynamics is covered in Sect. 3. Numerical simulation and discussion find place in Sect. 4 followed by parameter sensitivity analysis performed in Sect. 4.1 and curve-fit using optimization algorithm performed in Sect. 4.2. Conclusion has been laid out in Sect. 5.
2 Mathematical model: evolution
The epidemic–economic model under investigation inspired from [19], is an amalgamation of Solow’s economic growth model [21, 22] and an \(SIV_1V_2R\) epidemic model. The \(SIV_1V_2R\) model has been derived from the original SIR (Susceptible, Infected, Recovered) epidemiological model presented by Kermack and McKendrick [23]. The model divides the population into three different classes, i.e., S, I, R assuming constant birth and death. SIR model has been the epicentre of disease modelling since its introduction. The differential equations pertaining to the SIR model take the following form:
The susceptible class represents the section of the population that is prone to the disease but have not acquired it. Infected class represents the section that is infected from the disease and Removed class encompasses population that is no longer infected. Either the population has recovered from the infection or died from it. For our research intentions, we have populated the basic SIR model with two vaccinated classes \(V_1\) and \(V_2\) inspired from [24]. Vaccinated class \(V_1\) represents the section of the population that have been vaccinated once. \(V_2\) class involves population that have been vaccinated with both the doses. The \(SIV_1V_2R\) model so obtained is refashioned with the following assumptions:
-
All of the susceptible population do not get vaccinated. Only a fraction of them get vaccinated due to the apprehensions surrounding vaccines.
-
The interaction between susceptible and infected classes is mapped by Holling type-II functional response.
-
Even after getting vaccinated with both the doses, the population can still join the susceptible class and be prone to getting infected. These kind of infections are termed as ‘Breakthrough’ infections [25, 26] and exist for all types of vaccines prescribed against SARS-COVID-2. Breakthrough infections can be attributed to occurrence of severe variants (such as the delta variant), low immune response to vaccination and traveling to places that are seeing significant surge in cases.
-
Breakthrough infections may even occur after first dose. Owing to the facts presented by various studies [26,27,28], it is evident that the percentage of breakthrough infections is less and that the severity of infection reduces manifold. Hence, given the trifle quantity of breakthrough infections [28, 29], we choose to associate it with only one class of vaccination and have assumed it to be associated after second dose, i.e., \(V_{2}\) class. This assumption also finds backing from the idea that general masses unless fully vaccinated take more care and precautions and are less prone to falling prey to breakthrough infections.
-
After recovering naturally from the infection, the population can still join the susceptible class and be prone to getting infected. Such infections are termed as ‘Reinfections’. A reinfection as defined by Indian Council Of Medical Research (ICMR) is the occurrence of two positive tests at a gap of at least 102 days with one interim negative test.
-
The susceptible, vaccinated and the recovered class contribute to the economy. How ? Highlighting the importance of vaccination, majority of countries have made it mandatory for their citizens to get the jab for working offline both in government and private spaces. Following this rule will result in increased employment opportunities for the masses and fuel the slow paced economy, thus aiding in increased capital stock for the country.
-
The infected population cannot contribute as they are sick, need physical and mental rest, and are not in a position to work.
The equation of evolution of capital stock from Solow’s economic growth model [21] is given by
The epidemic model \(SIV_1V_2R\) in the current scenario when the vaccination drive is in progress is given by
The system is bounded in the region \(\{S,I,V_1,V_2,R;S+I+V_1+V_2+R=N \}\).
Combining Eqs. (2) and (3), we obtain the amalgamated epidemic–economic model in question as follows:
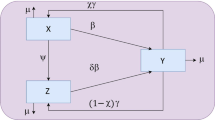
Figure 1 demonstrates the flow diagram of the proposed model.

Flow diagram of the \(KSIV_1V_2R\) model. Susceptible individuals S can either move to the infected class I or the vaccinated class \(V_1\). The susceptibles who get vaccinated with the first dose join vaccinated class \(V_1\) at the rate of p. Individuals who recover naturally after getting infected, join the recovered class R at the rate of \(\gamma \). Individuals who receive the second dose of vaccination after getting the first dose move towards the vaccinated class \(V_2\) at the rate of \(p_1\). After receiving both the doses, individuals move towards the recovered class R at the rate of \(p_2\). Even after recovering from the infection naturally or getting vaccinated with both the doses, individuals from the recovered class R join back to the class of susceptibles S at the rate of \(\psi \) owing to breakthrough infections/reinfections. Only the classes \(S,V_1,V_2\) and R can join the labour force to contribute to the class of capital stock K
The variables and parameters used in the model are defined in Table 1.
3 Model dynamics
3.1 Existence of equilibrium points
The system (4) possesses a disease free or boundary equilibrium point \(E^0(K^0,S^0,0,V_1^0,V_2^0,R^0)\) given by
Endemic or interior equilibrium point \(E^*(K^*,S^*,I^*,V_1^*,V_2^*,R^*)\) for the system (4) is given by
It follows that \(I^{*}>0\) and \(R^{*}>0\), if \((1-p)Nb_{1}>(\mu +\gamma ) \) and \((\mu + \gamma )(\mu +\psi )(m \mu + b_{1})> \psi b_{1}\gamma .\) We will now be analysing the stability of boundary and interior equilibrium points for the system (4).

Relation between vaccinated class \(V_1\) and Recovered class R
3.2 Mathematical analysis
The \(KSIV_{1}V_{2}R\) model used in this paper is locally and globally stable. For better understanding of the mathematical analysis of the \(KSIV_{1}V_{2}R\) model, relevant matter has been stated in Appendix 1.
3.2.1 Basic reproduction number
Basic reproduction number \(R_0\) is a crucial element of the dynamic analysis of any epidemic model. It signifies the number of secondary infections stemming from a single infection. If \(R_0\le 1\), then the disease will die out; if \(R_0>1\), then the disease will continue in the system. Since, we want to explore the impact of vaccination when the infection is present, we will be dealing with \(R_0>1\) primarily. \(R_{0}\) can be written as

Relation between \(V_1\),R and K when rate of first dose of vaccine ‘p’ is modulated
4 Numerical simulation and discussion
The analysis has been performed for \(R_{0}>1\) which implies that the disease is prevalent in the system and does not die out. The system of equations (4) for parametric values mentioned in Table 2 has a unique positive equilibrium \((K^*,S^*,I^*, V_{1}^*, V_{2}^*, R^*)\) resting at (237.0320, 0.5716, 11.8177, 0.4446, 0.0366, 105.0860).
We see that the system (4) demonstrates (Fig. 2) a positive relation of the capital stock and recovered class with the vaccinated class \(V_1\) which falls in line with the intent behind the model discovering how the vaccinated classes contribute towards the economy. The vaccinated class \(V_1\) adds to the capital stock and recoveries. This is also evident from Table 4 for sensitivity indices, wherein the rate of first dose of vaccine ‘p’ is positively correlated to both the vaccinated classes \(V_1\), \(V_2\) and the capital stock.

Association of vaccination and GDP per capita across countries

Relation between vaccinated class \(V_2\) and infection I, when rate of second dose of vaccination ‘\(p_1\)’ is modulated

Effect of media on infected class I and susceptible class S
Modulating the rate of first dose of vaccine p, we observe that (Fig. 3) as the rate is dipped to \(p=0.4545\) rate/day, it results in lower values of capital stock and recoveries. Furthermore, on increasing the rate to \(p=0.0000004545\) rate/day, we observe that capital stock and recovered class show a significant boost.
Remark 1
Our results vouch an exact replication of situation around the ongoing pandemic. In the absence of an exact cure to the disease, vaccination stands to be our biggest weapon in fighting the disease and controlling the damage done by the infection. If the population is not adequately vaccinated, it may fall prey to the deadly infection resulting into severe health issues and increased fatalities. On the contrary, if the masses are vaccinated timely and with an increased rate, it will not only result into increased recoveries but also boost the capital stock of the nation. Results obtained from the model demonstrate an increased capital stock corresponding to an increased rate of vaccination and vice versa. An increasing capital stock is the lodestar for increased GDP. How? An increased value of capital stock brings specialisation and large-scale production along [30]. Both of these entities bring down the cost of production per unit in addition to offering increased output and productivity. In fact, the economy suffers when the rate at which capital stock moves in fails to match with the rate of growing population leading to humongous under-employment and unemployment [22, 30]. Hence, a capital stock that is expanding, by all means, contributes to a blooming GDP. Findings from our model align perfectly with outcomes of prominent literature [14, 16, 17] which maintains a firm stand on higher GDP values being associated with higher vaccination rates across the globe.
Another milestone towards our model and its consequent work is the data from 24 countries [13]. Table 3 illustrates GDP per capita (Current U.S dollar) of 2019 [31] and its comparison with GDP per capita (Current U.S dollar) of 2020 [32] and the second quarterly estimate of GDP per capita (U.S dollars, Current Price) in the form of ‘World Outlook Economic Database—October 2021’ [33] published by International Monetary Fund. Percentage of people those who have received first dose (\(V_1\)) and percentage of people those who have received both the doses (\(V_2\)) add in to form total vaccinated percentage [13] in a country, i.e., (\(V_1 +V_2\)) in Table 3. The table covers comparative analysis of the GDP per capita of 24 countries in 2019 and 2020 to that of October 2021 while demonstrating the vaccinated population percentage. Countries have been arranged in descending order of vaccinated population percentage as on November 10, 2021. Prima facie, it is observed that economies with prominent vaccinated percentage show greater boost in GDP figures falling in line with the concept and results of our model. Obviously, the increase in GDP is uneven across countries owing to the degree of positive correlation that exist between the vaccinated population percentage and GDP per capita of that respective country [17]. This degree of correlation depends on a multitude of factors including geographical distribution, population density,cvaccine hesitancy, and vaccine Nationalism [15]. However, narrowing down to countries with vaccinated percentage less than 60%, i.e., Mexico, India, Indonesia, Russia, Bangladesh, and South Africa, it is to be noted that their increase in GDP per capita is not as prominent as compared to countries with vaccinated percentage more than 60%. Looking at the values of GDP per capita (2019) and the estimates of GDP per capita October 2021, it can be deduced that vaccination instigates enhanced economic growth, further strengthening the results propagated by the model. For better understanding of the results, a pictorial representation (Fig. 4) of GDP per capita October 2021 and its association with vaccinated population percentage as on November 10, 2021 is shown on World map.
Understanding the relation between infected class and the vaccinated class \(V_2\) (second dose) (Fig. 5), it is interesting to observe that the number of infections starts to come down as the vaccinated class \(V_2\) increases. The rate \(p_1=0.001\) rate/day for second dose is less than that of \(p=0.004545\) rate/day for the first dose. A period of gap is necessarily required between the doses for the effective working of the vaccines. Due to irregular periods between which the two doses are taken, availability/non-availability of the second dose, and the callous nature of the masses after taking first shot of the vaccine, all contribute towards a lower rate of \(p_1\) as compared to its counter part p and has been taken in accordance with the above-mentioned factors.
Remark 2
We observe in Fig. 5 that an increase in rate (\(p_1=0.00005\) rate/day) of second dose of vaccine curbs the infection to a greater degree, bringing it down as evident from the graph. Though, while the rate (\(p_1=0.9\) rate/day) of second dose of vaccine is decreased, the infections start rising in a prominent manner. This behaviour of the system backs the idea propagated by scientist and medical board regarding the second dose of vaccination. Taking both the doses at appropriate intervals guarantees maximum protection from the infection and curb fresh infections from spewing up. In an indirect relationship, less infections would definitely aid in stabilizing the economy if not remarkably increase it. A concrete evidence supporting our result is the study [34] conducted by ‘Centers for Disease Control and Prevention’ (CDC). Data [35] were extracted from 4000 individuals with versatile professions viz health care workers, delivery workers, teachers, and first responders who were inoculated with Moderna/Pfizer vaccine between the period of December 2020 and March 2021. The study concludes that vaccines caused a 90% reduction in all infections.

Parameter sensitivity analysis K, R, S
Also, the two rates \(p_1=0.001\) and \(p_1=0.00005\) show close statistics. Even if we increase the rate sufficiently high, it continues to curb infections at an intensity similar to that of \(p_1=0.001\).
Analysing the effect of media on susceptible class S and infected class I against time, our results (Fig. 6) show slight variation from the perceived notions of how media affect us. With subsequent lock downs and restricted movements happening during the course of pandemic, we are hooked on to our television sets and mobile phones more than ever, hence experiencing and absorbing larger quantities of information fed to us. As we increase the rate with which the media affects us from \(m=0.5\) to \(m=0.9\), we see prominent rise in the number of both susceptible and infected classes (also evident from the values pinned on the graph Fig. 6, X-represents susceptibles in the figure and Y-represents infected in the figure). The effect on infected class is more. Reducing the effect of media to \(m=0.0005\), we see that it brings down susceptible and infected individuals to some extent. Further reduction in the rate to \(m=0.000005\), the system maintains status quo.

Parameter sensitivity analysis \(I,V_1,V_2\)
Remark 3
There is no doubt that the media do affect us. Increasing the rate with which it affects us implies that our exposure to it increases. As evident from the results obtained, \(m=0.9\) has a negative impact on the system. With a new piece of information emerging everyday, contrasting data on how the infection may spread and how to avert it, the recurring waves of infection and the dynamics of the disease make media a tricky partner. Dwelling too much into it may make the general population uneasy as if the infection is in-evitable given the new variants and when the numbers spike. This may lead to panic movements across cities, regions, and even countries spreading infection to places that have successfully got control of it. Also, on seeing infections go down general masses adopt callous attitude towards COVID-19 appropriate behaviour. As a result people visit flea markets, and attend and organize large-scale ceremonies and head for popular tourist destinations thereby adding to infections and susceptibility. The case of Russia serves as a classic example in this context. During the month of March, 2021, Russia declared its region almost infection free with its indigenous vaccine ‘Sputnik-V’ encapsulating an efficacy of 98%. The cases had gone down considerably, falling to less than 8000 in the month of May, 2021. and the country was boosting of its fight against the infection. The media reported accordingly and general masses started taking it lightly without feeling the need to get vaccinated and adopting callous behaviour against COVID-19 appropriate culture. As a result, within a month, the cases in Russia doubled up asking the administration to intervene and advise people to follow norms. It later came out that only 13% of the population had been vaccinated as on May,2021 which led to the spike in the infections once the masses were devoid of the fear of contracting the virus. Cases continue to increase in Russia [36] (22,000 as of 1-08-2021), though people have started taking an account of the situation.
Reducing the effect of media, i.e., to \(m=0.0005\), we see positive impact on the system which is obvious in context to the aforementioned explanation. Limited exposure also limits the chances of misinformation and fake news/partial information from making rounds which in turn makes the audience alert but not assertive. The figures of death and helplessness can more often than not, and disturb individuals mentally and emotionally making their immune system vulnerable. Selective consumption of data contributes to a better state of physical and mental health aiding in stabilization of infections. Further diminishing the rate with which the media affect us to \(m=0.000005\), we see that the state of the system remains unchanged, indicating that there needs to be sufficient exposure for any visible change to occur. With such trifle value, system retains its last state and has no considerable effect to show. Hence, it can be said that media though indirectly have a considerable impact on the economy of a country.

Curve fit
4.1 Parameter sensitivity analysis
We have performed sensitivity analysis of the endemic equilibrium point \(E^* (K^*,S^*,I^*,V_1^*,V_2^*,R^*)\) with respect to all the epidemic–economic parameters present in the model pertaining to the methodology in [37]. Through this process of parameter sensitivity analysis, we investigate the degree to which a parameter can affect the concerned variable through an affirmative relationship or a negative relationship. The sensitivity index (Table 4) obtained gives us the proportion that a relative change in a parameter brings to the relative change in a variable.
Definition
[37]. For the variable x that depends differentiably on a parameter p, we define the normalised forward sensitivity index \(\beta \) of a variable as
In layman terms, for a parameter p and \(\beta ^{x}_{p}=1\) as we increase or decrease p by certain percentage, let us say k percent, then x also increases or decreases by the same k percentage. For instance, \(\beta ^{V^{*}_1}_{p}=1.1240\) depicts the relation of vaccinated class \(V_1\) with the rate of first dose of vaccine, i.e., p. As we increase p, vaccinated class \(V_1\) increases as well as evident from Fig. 3. Also
It is understood that p the rate of first dose of vaccine, i.e., vaccination will bring down the infections and susceptibles by offering subsequent protection, and thus, it has a negative relationship with infected class and susceptible class. Rate of first dose of vaccine facilitates for the second dose and hence in an affirmative association with vaccinated class \(V_2\).
The parameter \(\psi \) is in a positive relationship with the infected and susceptible class and in an negative association with the recovered class, i.e., \(\beta ^{S^{*}}_{\psi }=0.1591,\quad \beta ^{I^{*}}_{\psi }=0.1867,\quad \beta ^{R^{*}}_{\psi }= 0.0219\). The parameter \(\psi \) denotes the rate at which the individuals after a breakthrough infection/reinfection join the susceptible class. Hence, as the rate of \(\psi \) increases, it increases the vulnerability of the population to get infected and hence increases susceptibles and infections accordingly. Also, increased susceptibles and infections would hamper recoveries, and hence, \(\psi \) is negatively related to the recovered class. The value \(\beta ^{V^{*}_2}_{p_1}=0.7498\) propagates that the rate of second dose of vaccine, i.e., \(p_1\) is in positive relation with vaccinated class \(V_2\) which implies that as we increase the rate of second dose, the individuals in class \(V_2\) will increase accordingly which is obvious. Natural recovery rate \(\gamma \) shares an affirmative mapping with the capital stock, susceptible class, recovered class, and a negative association with the infected class
An increase in natural recoveries would definitely boost the capital as recovered class is contributing to the capital stock (Eq. 4). Since a portion from the recovered class goes into susceptible class again, hence increasing \(\gamma \) increases susceptibles too. Again, an increase in natural recoveries would lead to less infections and hence the relationship between them. Table 4 explains how the various epidemic–economic parameters are associated with the epidemic–economic variables when the system is in a state of equilibrium. A graphical representation (Figs. 7, 8) of Table 4 explains the relationship in a visually rich and enhanced manner.
This analysis can be of great help in policy formation and predicting future trends of recoveries and infections. For instance, looking at the relationship between rate of vaccination of first dose p and the vaccinated class \(V_2\) and infected class I, increasing the rate of vaccination would certainly aid in bringing down the infection and facilitate for the second dose of vaccination. Hence, majority of offices and institutions both private and government have put a policy of “Compulsory vaccination to work”. In another scenario, predicting trends of the pandemic like, to what extent can a rise in the rate of infection \(b_1\) increase the additions to infected class? or how many people can recover each day, if the recovery rate \(\psi \) increases by a specific percentage. Such forecasts can be made.
4.2 Curve-fit using optimization algorithm
Following numerical approximation, we have fitted our system with the help of the initial conditions and the parametric values. The method’s role is to minimize the square of errors of all the parametric values of our data [38]. We have used Levenberg–Marrquadt algorithm which helps in minimizing the residual by comparing the current residual vector with previous residual vector [39]. Furthermore, since we did not get the desired results, we optimized the curve fit again by Nedlar–Mean algorithm [40] which uses initial guess for parameter estimation [41] (Fig. 9) and the result propagates that this methodology assisted with producing a perfect match for our model as we get a single regression line and all the cluster points are nearest to regression line which indicates that residual error is minimum [42].
5 Conclusion
We have braced an epidemic–economic model which is the amalgamation of an \(SIV_1V_2R\) model and Solow’s model of economic growth. The \(SIV_1V_2R\) model has been obtained by populating the basic SIR model with vaccinated classes \(V_1\) (recipients of the first dose) and \(V_2\) (recipients of the second dose). Model dynamics have been investigated for the existence and local stability of boundary and interior equilibrium points and global stability of interior(endemic) equilibrium point. Parameter sensitivity analysis for system (4) has been performed. Also, we have performed curve fit for the system (4) using Nedlar–Mean algorithm. Our analysis reveals the following:
-
1
Will vaccination instigate economic growth ? A simple answer to this tricky question is ‘Yes’. Results obtained from the model as shown in Fig. 3 clearly indicate an improved capital stock with improved vaccination rates and a decreased capital stock with low vaccination rates. Providing firm testimony to our results are the recent studies (discussed in Sect. 1.1) vouching in all forms for higher GDP rates belonging to countries with high vaccination rates. A hands-on-evidence to further strengthen the bond between vaccination and economic growth is the data from 24 countries (Table 3) on the positive relationship of GDP per capita and vaccinated population percentage which clearly propagates the results obtained from our model.
-
2
Findings from the model (Fig. 5) reveal that complete vaccination brings down the infection considerably. Earlier vaccinations were just associated with preventing hospitalizations and reducing the degree of severity of infections but as the results have it, they are also cutting on circulation of silent infections. The conclusion of a study done by CDC in 2021 (discussed in Sect. 4) is in synchronisation with the outcomes of our model in this context.
-
3
Media, in all of its form, print, and electronic, are playing a crucial role in the face of the catastrophe that the novel SARS-COVID-2 has bestowed globally. As the model points out (Fig. 6) increased exposure to media instigates infections and susceptibles, whereas for vice versa, we see a decline in infections. In either of the case, the economy gets affected.
-
4
Through performing parameter sensitivity analysis (Table 4) for the proposed epidemic–economic model, we have gained insight on the intensity with which the rate of vaccination of first dose p facilitates vaccinated classes \(V_1\) and \(V_2\) and brings down the addition to infected class I. The performance of the rate of natural recoveries in hitting the infected class has also been demonstrated (Table 4). Hence, quantifying the association of parameters with variables in the epidemic–economic model through the exercise of parameter sensitivity analysis can greatly aid in curating policies both economical and health wise that fulfill the major goal behind them.
Apart from indigenous growth, vaccines are facilitating global economy as well. How? The aftermath of global cost of vaccination reveals that high-income countries can expect a worthwhile return of 4.80 dollars for every dollar spent on facilitating low-income countries with vaccines. As in the event of low-income countries not being able to access vaccines, the world should be ready for sustaining loses between 60 and 340 billion dollars a year in GDP. As an extension to this work, parameters denoting different entities such as ‘vaccine hesitancy’, ‘effect of pandemic on population growth rate and its economic consequences’, ‘rise in mental health issues’ and impact of ‘work from home’ condition, etc., can be added to the model and their effect be analysed.
References
McKinsey Company. Covid-19: Implications for business. http://www-personal.umich.edu/~mejn/netdata/ . Accessed 10 August 2021 (2021)
Covid-19 map, johns hopkins coronavirus resource center. https://coronavirus.jhu.edu/map.html. Accessed 1 August 2021 (2021)
F. Baldassi, F. D’Amico, A. Malizia, P. Gaudio, Evaluation of the spatiotemporal epidemiological modeler (stem) during the recent covid-19 pandemic. Eur. Phys. J. Plus 136(10), 1072 (2021)
R. Fitriani, W.D. Revildy, E. Marhamah, T. Toharudin, B.N. Ruchjana, The autoregressive integrated vector model approach for covid-19 data in Indonesia and Singapore. J. Phys: Conf. Ser. 1722, 012057 (2021)
U. Tirnakli, C. Tsallis, Epidemiological model with anomalous kinetics: early stages of the covid-19 pandemic. Front. Phys. 8, 613168 (2020)
A.I. Shnip, Epidemic dynamics kinetic model and its testing on the covid-19 epidemic spread datas. J. Eng. Phys. Thermophys. 94, 6–17 (2021)
T. Kapitaniak, S. Jafari, Nonlinear effects in life sciences. Eur. Phys. J. Spec. Top. 227(7–9), 693–696 (2018)
A. Gowrisankar, T.M.C. Priyanka, S. Banerjee, Omicron: a mysterious variant of concern. Eur. Phys. J. Plus 137(1), 1–8 (2022)
C. Kavitha, A. Gowrisankar, S. Banerjee, The second and third waves in India: when will the pandemic be culminated? Eur. Phys. J. Plus 136(5), 1–12 (2021)
D. Easwaramoorthy, A. Gowrisankar, A. Manimaran, S. Nandhini, L. Rondoni, S. Banerjee, An exploration of fractal-based prognostic model and comparative analysis for second wave of covid-19 diffusion. Nonlinear Dyn. 106(2), 1375–1395 (2021)
A. Gowrisankar, L. Rondoni, S. Banerjee, Can India develop herd immunity against covid-19? Eur. Phys. J. Plus 135(6), 1–9 (2020)
Covid-19 vaccine tracker, regulatory affairs professionals society (raps). https://www.raps.org/news-and-articles/news-articles/2020/3/covid-19-vaccine-tracker. Accessed 1 August 2021 (2021)
H. Ritchie, E. Mathieu, L. Rodés-Guirao, C. Appel, C. Giattino, E. Ortiz-Ospina, J. Hasell, B. Macdonald, D. Beltekian, and M. Roser. Coronavirus pandemic (covid-19). Our World in Data. https://ourworldindata.org/coronavirus. Accessed 10 November, 2021 (2020)
A. Roghani and S. Panahi. The Global Distribution of Covid-19 Vaccine: The Role of Macro-Socioeconomics Measures. Medrxiv, 2021
M. Hafner, E. Yerushalmi, C. Fays, E. Dufresne, and C. V. Stolk. The global economic cost of covid-19 vaccine nationalism. https://doi.org/10.7249/RBA769-1 (2020)
G. Owens, J. Khusanov. Will vaccination end the pandemic? Available at SSRN 3839234 (2021)
D. Dongarwar, B.Y. Garcia, S.O. Maiyegun, K.K. Yusuf, H.M. Salihu, Covid-19 early vaccination rates and gross domestic product per capita. Int. J. Transl. Med. Res. Public Health 5(1), 37–40 (2021)
N.A. Masia, J. Smerling, T. Kapfidze, R. Manning, M. Showalter, Vaccination and GDP growth rates: exploring the links in a conditional convergence framework. World Dev. 103, 88–99 (2018)
S. Sahbani, H.T. Alaoui, A. Kaddar, Fluctuations of solow economic growth model in the presence of an infectious disease. Appl. Math. Sci. 13(13), 627–636 (2019)
S. Quilici, R. Smith, C. Signorelli, Role of vaccination in economic growth. J. Market Access Health Policy 3(1), 27044 (2015)
R.M. Solow, A contribution to the theory of economic growth. Q. J. Econ. 70(1), 65–94 (1956)
F. Karim, S. Chauhan, J. Dhar, On the comparative analysis of linear and nonlinear business cycle model: effect on system dynamics, economy and policy making in general. Quant. Fin. Econ. 4(1), 172–203 (2020)
W. O. Kermack, A. G. McKendrick. A contribution to the mathematical theory of epidemics. in Proceedings of the Royal Society of London. Series A, Containing Papers of a Mathematical and Physical Character, vol. 115(772), pp. 700–721 (1927)
F. Rizvi. Mathematical modeling of two-dose vaccines. PhD thesis, The Ohio State University (2016)
What you should know about the possibility of covid-19 illness after vaccination, centers for disease control and prevention. https://www.cdc.gov/coronavirus/2019- ncov/vaccines/effectiveness/why-measure-effectiveness/breakthrough-cases.html. Accessed 1 August 2021 (2021)
M. Klompas, Understanding breakthrough infections following mRNA SARS-CoV-2 vaccination. JAMA 326, 2018–2020 (2021)
Covid-19 - can i get infected after vaccination? https://www.who.int/emergencies/diseases/novel-coronavirus-2019/media-resources/science-in-5/episode-49-can-i-get-infected-after-vaccination?gclid=EAIaIQobChMI0avK4oiT9AIVSQ8rCh3qqAiKEAAYASAAEgJowfDBwEASAAEgJowfDBwE [Accessed 12, November,2021], 2021
Washington State Department of Health. Sars-cov-2 vaccine breakthrough surveillance and case information resource. https://www.doh.wa.gov/Portals/1/Documents/1600/coronavirus/data-tables/420-339-VaccineBreakthroughReport.pdf. Accessed 12 November 2021 (2021)
J. Kates, L. Dawson, E. Anderson, A. Rouw, J. Michaud, N. Singer. Covid-19 vaccine breakthrough cases: Data from the states. https://www.kff.org/policy-watch/covid-19-vaccine-breakthrough-cases-data-from-the-states/. Accessed 12 November 2021 (2021)
F. Karim, S. Chauhan, S.K. Bhatia, J. Dhar, Hopf bifurcation in an augmented is-lm linear business cycle model with two time delays. Int. J. Math. Eng. Manage. Sci. 5(3), 518–528 (2020)
Gdp per capita (current u.s dollars) - 2019, data. https://data.worldbank.org/indicator/NY.GDP.PCAP.CD?end=2019&start=1960. Accessed 10 November 2021 (2019)
Gdp per capita (current u.s dollars) - 2020, data. https://data.worldbank.org/indicator/NY.GDP.PCAP.CD?end=2020&start=1960. Accessed 10 November 2021 (2020)
Gdp per capita (current prices, u.s. dollars)-international monetary fund. https://www.imf.org/en/Publications/WEO/weo-database/2021/October. Accessed 10 November 2021 (2021)
Gdp per capita (current prices, u.s. dollars)-international monetary fund. https://www.imf.org/en/Publications/WEO/weo-database/2021/October. Accessed 10 November 2021 (2021)
F. Flam, T. Gupta, S. Zompa. Don’t believe doomsayers. Vaccines will end the pandemic, the print. https://theprint.in/health/dont-believe-doomsayers-vaccines-will-endthe-pandemic/631444/. Accessed 1 August 2021 (2021)
H. Ritchie, E. Mathieu, L. Rodés-Guirao, C. Appel, C. Giattino, E. Ortiz-Ospina, J. Hasell, B. Macdonald, D. Beltekian, M. Roser. Coronavirus pandemic (covid-19)-the data-statistics and research, our world in data. https://ourworldindata.org/coronavirus-data. Accessed 1 August 2021 (2020)
N. Chitnis, J.M. Hyman, J.M. Cushing, Determining important parameters in the spread of malaria through the sensitivity analysis of a mathematical model. Bull. Math. Biol. 70(5), 1272–1296 (2008)
J.O. Ramsay, G. Hooker, D. Campbell, J. Cao, Parameter estimation for differential equations: a generalized smoothing approach. J. Roy. Sta. Soc. Ser. B Stat. Methodol. 69(5), 741–796 (2007)
F. Hamilton, Parameter estimation in differential equations: a numerical study of shooting methods. SIAM Undergraduate Res. Online 4(16–31), 1 (2011)
R. Barati, Parameter estimation of nonlinear muskingum models using nelder-mead simplex algorithm. J. Hydrol. Eng. 16(11), 946–954 (2011)
Parameter estimation for differential equations. https://tavoglc.medium.com/parameter-estimation-for-differential-equations-bd5e44bf2fd7. Accessed 1 June 2021 (2019)
A.N. More, P.S. Kohli, K.H. Kulkarni, Simple linear regression with least square estimation: An overview. International Journal of Computer Science and Information Technologies 7(6), 2394–2396 (2016)
Z. Shuai, V.D.P. van den Driessche, Global stability of infectious disease models using lyapunov functions. SIAM J. Appl. Math. 73(4), 1513–1532 (2013)
H. Guo, M. Li, Z. Shuai, A graph-theoretic approach to the method of global lyapunov functions. Proc. Am. Math. Soc. 136(8), 2793–2802 (2008)
K. Bessey, M. Mavis, J. Rebaza, J. Zhang, Global stability analysis of a general model of zika virus. Nonautonomous Dynamical Systems 6(1), 18–34 (2019)
P. Gulati, S. Chauhan, A. Mubayi, T. Singh, P. Rana, Dynamical analysis, optimum control and pattern formation in the biological pest (efsb) control model. Chaos Solit. Fract. 147, 110920 (2021)
Author information
Authors and Affiliations
Ethics declarations
Conflict of interest
All authors declare no conflicts of interest in this paper.
A Mathematical analysis
A Mathematical analysis
1.1 A.1 Local stability analysis
General Jacobian matrix for system (4) is given by
where \(Z = \sigma K^\alpha (1-\alpha )(S+V_1+V_2+R)^{-\alpha }\)
General characteristic equation pertaining to the Jacobian matrix above is given by
Characteristic equation pertaining to the boundary equilibrium point \(E^0\) is given by
Eigen values corresponding to boundary equilibrium point \(E^0\) are \( \lambda _1= \frac{\alpha Z^0(S^0+V_1^0+ V_2^0+R^0)}{K^0(1-\alpha )}-\delta < 0\), if \( K^0 > \frac{\alpha Z^0(S^0+V_1^0+ V_2^0+R^0)}{\delta (1-\alpha )}, \lambda _2=-\mu , \lambda _3= b_1S^0-(\mu +\gamma )<0 \) if \( b_1S^0<(\mu +\gamma )\) or \(R_0<\frac{N}{S^0} , \lambda _4= -(\mu +p_1), \lambda _5= -(\mu +p_2), \lambda _6= -(\mu +\psi ) \). Consequently, \(E^0\) is stable if, \( K^0 > \frac{\alpha Z^0(S^0+V_1^0+ V_2^0+R^0)}{\delta (1-\alpha )}\) and \(R_0<\frac{N}{S^0}\). Next, the characteristic equation pertaining to interior equilibrium point \(E^*(K^*, S^*, I^*, V_1^*, V_2^*, R^*)\) is given as follows:
Expanding the above expression, we obtain
where
Following Routh–Hurwitz criterion, we obtain that the endemic equilibrium point \(E^*(K^*, S^*, I^*, V_1^*, V_2^*, R^*)\) is stable, provided the following conditions are met:
1.2 A.2 Global stability
To establish global stability, we count on the graph-theoretic method [43,44,45,46]. We have constructed a Lyapunov function through a directed graph using the terminologies from [43]. A directed graph possesses a set of ordered pair say (i, j) and vertices. Here, (i, j) is known as arc to terminal vertex j from initial vertex i. For the terminal vertex j, \(d^{-}(j)\) is the in-degree of j which denotes the number of arcs in the digraph. For initial vertex i, \(d^{+}(i)\) is the out-degree of vertex i which denotes the number of arcs in the digraph. Let us consider a weighted directed graph say \(\chi (P)\) over a \(q\times q\) weighted matrix P where the weights(\(a_{ij}\)) of each arc, if they exist, are \(a_{ij}>0\), and if otherwise, then \(a_{ij}=0\).
We consider \(c_{i}\) as the co-factor of \(l_{ij}\) of the Laplacian of \(\chi (P)\) which is given by
If there is a strongly connected path, i.e., directed to and fro path for the arcs in \(\chi (P)\) then \(c_i>0 \quad \forall \quad i=1,2,\ldots ,q\). We rope in Theorem 3.3 and Theorem 3.4 from [43, 45], which will help us in the construction of lyapunov function. The theorem is as follows:
-
Theorem 3.3 of [43]: if \(a_{ij}>0\) and \(d^{-}(i)=1\), for some i, j, then
$$\begin{aligned} c_{i}a_{ij}=\sum _{k=1}^{q}c_{j}a_{jk} \end{aligned}$$ -
Theorem 3.4 of [43]: if \(a_{ij}>0\) and \(d^{+}(j)=1\), for some i, j, then
$$\begin{aligned} c_{i}a_{ij}=\sum _{k=1}^{q}c_{k}a_{ki}. \end{aligned}$$
Also, we use Theorem 3.5 of [43] which is stated as Theorem 1.
Theorem 1
Let us consider an open set \( L\subset R^{m}\) and a function \(f: L\rightarrow R^{m}\) for a system
and assuming:
(a) \(\exists \) \(B_{i}:L\rightarrow R\) , \(G_{ij}:L\rightarrow R\) and \(a_{ij}\ge 0\), such that
\(B'_{i}=B'_{i}\vert _{6} \le \sum ^{q}_{j=1}a_{ij}G_{ij}(z)\), with \(z\in L\), \(i=1,\dots ,q\)
(b) For \(P=[a_{ij}]\), of (G, P) each directed cycle \(D_{c}\) satisfies \(\sum _{(i,j)\in \epsilon (D_{c})}G_{ij}(z)\le 0\) , \(z\in L\),
where \(\epsilon (D_{c})\) is set of arcs in \(D_{c}\).
Then, for \(c_{i}\ge 0 , i=1,\dots ,q\), the function is
satisfies \(B'\vert _{6} \le 0\), that is, B(z) is a Lyapunov function for 6.
1.2.1 A.2.1 Constructing the Lyapunov function
Let
Now, by differentiation, we have
where, \( a_{21}=(1-p)\mu N + \mu S^{*}, a_{23}=b_{1}S^{*}, a_{26}=\psi .\)
For \(B_1\) differentiating, we have, \( B'_{1}=(K-K^{*})K'\le \sigma K^{\alpha +1}(S +V_1+V_2+ R)^{1-\alpha } - \delta KK^{*}\). Adhering to the complexity of the model, we have considered two cases.

Directed graph for \(\alpha =0\)

Directed graph for \(\alpha =1\)
Case I: \(\alpha = 0\)
The lyapunov function constructed makes
where \(\quad a_{12}=\sigma =a_{14}=a_{15}=a_{16}\) and \( a_{51}=\delta K^{*}.\)
We get an associated weighted directed graph, as shown in Fig. 10. Then, by Theorem 3.5, [43] \(\exists c_{i}'s ,1\le i \le 6\), such that \(B=\sum ^{q}_{i=1}c_{i}B_{i}\) is a lyapunov function. Using Theorem 3.3 and 3.4, we get the relation between \(c_{i}\).
For \(a_{14}>0\) and \(d^{+}(4)=1\), we get \(c_{1}a_{14}=c_{4}(a_{45}+a_{42})\), and for \(a_{63}>0\) and \(d^{-}(6)=1\), we get \(c_{6}a_{63}=c_{5}a_{56}+c_{3}a_{36}\). Hence
Thus,
the lyapunov function is as follows:
And, for \(B'\)
Case II: \(\alpha = 1\)
We get an associated weighted directed graph as shown in Fig. 11. Similarly as above, for \(a_{45}>0\) and \(d^{+}(5)=1\), we get \(c_{4}a_{45}=c_{5}(a_{52}+a_{56})\). Hence,
Thus, the lyapunov function is as follows:
And, for \(B'\)
If we consider the set \(U=\{ x\in R_+^6 : B'=0 \}\), then we see that \(K=K^*\), \(S=S^*\), \(V_{1}=V_{1}^*\), \(V_{2}=V_{2}^*\), \(I=I^*\) and \(R=R^*\). Hence, we get the unique equilibrium point \((K^*,S^*,I^*, V_{1}^*, V_{2}^*, R^*)\). Therefore, following ’LaSalle’s Invariance’ principle, it can be said that the endemic equilibrium point is globally stable.
Rights and permissions
About this article

Cite this article
Karim, F., Chauhan, S. & Dhar, J. Analysing an epidemic–economic model in the presence of novel corona virus infection: capital stabilization, media effect, and the role of vaccine. Eur. Phys. J. Spec. Top. 231, 3545–3562 (2022). https://doi.org/10.1140/epjs/s11734-022-00539-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1140/epjs/s11734-022-00539-0