
Abstract
Aim
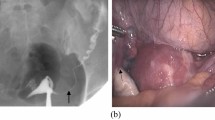
Hysterosalpingography (HSG) is one of the most commonly used methods in order to evaluate the condition of fallopian tubes in infertility clinics. In the present paper, we retrospectively compared the findings of HSG and laparoscopy to elucidate the relationship between tubal dysfunction and background factors, such asChlamydia trachomatis infection, endometriosis and previous surgery.
Methods
We retrospectively reviewed clinical records of 314 patients who were examined by both HSG and laparoscopy between 1996 and 2001 in the Department of Obstetrics and Gynecology, University of Tokyo.
Results
When HSG findings were evaluated in reference to those of laparoscopy, sensitivity and specificity for tubal patency were 0.63 and 0.79, respectively, whereas those for peritubal adhesion were 0.65 and 0.61, respectively. We compared the percentage of existence of background factors between the patients who were diagnosed as normal by both HSG and laparoscopy (Group L[+]) and those whose fallopian tubes were observed as patent by HSG, but were not patent by chromopertubation under laparoscopy (Group L[-]). The percentage of patients with positive chlamydial antibodies in Group L(-) (42.9%, 15/35) was significantly higher than that of patients with positive chlamydial antibodies in Group L(+) (22.8%, 44/193, P< 0.05).
Conclusions
These finding suggested that even if HSG showed normally patent tubes in a patient with positiveChlamydia trachomatis antibodies, the possibility of tubal occulusion still remains high and further examination by laparoscopy is recommended.
Similar content being viewed by others

References
Kodaman PH, Arid A, Seli E. Evidence-based diagnosis and management of tubal factor infertility.Curr Opin Obst Gynecol 2004;16: 221–229.
Land JA, Evers JLH. Chlamydia infection and subfertility.Best Prac Res Clin Obstetrics Gynecol 2002;16: 901–912.
Mol BWJ, Swart P, Mossuyt PMM, Veen F. Is hysterosalpingography an important tool in predicting fertility outcome?Fertil Steril 1997;67: 663–669.
Halis G, Arici A. Endometriosis and Inflammation in Infertility.Ann N Y Acad Sci 2004;1034: 300–315.
Kissler S, Hamscho N, Zangos Set al. Diminished pregnancy rates in endometriosis due to impaired uterotubal transport assessed by hysterosalpingoscintigraphy.Br J Obstetrics Gynaecol 2005;112: 1391–1396.
Bulletti C, Ziegler D, Polli V, Ferro E, Palini S, Flamigni C. Characteristics of uterine contractility during menses in women with mild to moderate endometriosis.Fertil Steril 2002;77: 1156–1161.
Bahamondes L, Bueno JG, Hardy E, Vera S, Pimentel E, Ramos M. Identification of main risk factors for tubal infertility.Fertil Steril 1994;61: 478–482.
Watrelot A, Hamilton J, Grudzinskas JG. Advances in the assessment of the uterus and fallopian tube function.Best Prac Res Clin Obstetrics Gynecol 2003;17: 187–209.
Holz K, Becker R, Schurmann R. Ultrasound in the investigation of tubal patency. A meta-analysis of three comparative studies of Echovist-200 including 1007 women.Zentrabl Gynacol 1997;119: 213–215.
Feanty P, Besnard S, Arnold A, Turner C, Cram P. Air-contrast sonohysterography as a first step assessment of tubal patency.J Ultrasound Med 2000;19: 519–527.
Mol BWJ, Lijmer J, Dijman B, Veen F, Wertheim P, Bossuyt PMM. The accuracy of serum chlamydial antibodies in the diagnosis of tubal pathology: a meta-analysis.Fertil Steril 1997;67: 1031–1037.
Akande VA, Hunt LP, Cahil DJ, Caul EO, Ford WCL, Jenkins JM. Tubal damage in infertile women: prediction using chlamydia serology.Hum Reprod 2003;18: 1841–1847.
Siegler AM. Hysterosalpingography.Fertil Steril 1983;40: 139–158.
Nugent D, Watson AJ, Killick SR, Balen AH, Rutherford AJ. A randomized controlled trial of tubal flushing with lipoidal for unexplained infertility.Fertil Steril 2002;77: 173–175.
Watson A, Vandekerckhove P, Lilford R, Vail A, Brosens I, Hughes E. A meta-analysis of the therapeutic role of oil soluble contrast media at hysterosalpingography: a surprising result?Fertil Steril 1994;61: 470–477.
Swart P, Beurden M, Mol BWJ, Redekop WK, Veen F, Bossuyt PMM. The accuracy of hysterosalpingography in the diagnosis of tubal pathology: a meta-analysis.Fertil Steril 1995;64: 486–491.
Jansen FW, Kapiteyn K, Trimbos-Kemper T, Hermans J, Trimbos JB. Complication of laparoscopy: a prospective, multicentre, observational study.Br J Obstetrics Gynaecol 1997;104: 595–600.
Fatum M, Laufer N, Simon A. Investigation of the infertile couple: Should diagnostic laparoscopy be performed after normal hyterosalpingography in treating infertility suspected to be of unknown origin?Hum Reprod 2002;17: 1–3.
Mol BWJ, Collins JA, Burrows EA, Veen F, Bossuyt PMM. Comparison of hysterosalpingography and laparoscopy in predicting fertility outcome.Hum Reprod 1999;14: 1237–1242.
Glatstein IZ, Adoni A, Sleeper LAet al. Observer variability in the diagnosis and management of the hysterosalpingogram.Fertil Steril 1997;67: 233–237.
Land JA, Evers JLH, Goossen VJ. How to use Chlamydia antibody testing in subfertility patients.Hum Reprod 1998;13: 1094–1098.
Dabekausen YAKM, Evers JLH, Land JA, Stale FS. Chlamydia trachomatis andibody testing is more accurate than hysterosalpingography in predicting tubal factor infertility.Fertil Steril 1994;61: 833–837.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Hiroi, H., Fujiwara, T., Nakazawa, M. et al. High incidence of tubal dysfunction is determined by laparoscopy in cases with positiveChlamydia trachomatis antibody despite negative finding in prior hysterosalpingography. Reprod Med Biol 6, 39–43 (2007). https://doi.org/10.1111/j.1447-0578.2007.00163.x
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1111/j.1447-0578.2007.00163.x