
Abstract
OBJECTIVE: To determine health utility scores for specific debilitated health states and to identify whether race or other demographic differences predict significant variation in these utility scores.
DESIGN: Utility analysis.
SETTING: A community hospital general internal medicine clinic, a private internal medicine practice, and a private pulmonary medicine practice.
PARTICIPANTS: Sixty-four consecutive patients aged 50 to 75 years awaiting appointments. In order to participate, patients at the pulmonary clinic had to meet prespecified criteria of breathing impairment.
MEASUREMENTS: Individuals’ strength of preference concerning specific states of limited physical function as measured by the standard gamble technique.
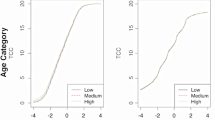
MAIN RESULTS: Mean utility scores used to quantitate limitations in physical function were extremely low. Using a scale for which 0 represented death and 1.0 represented normal health, limitation in activities of daily living was rated 0.19 (95% confidence interval [CI] 0.13, 0.25), tolerance of only bed-to-chair ambulation 0.17 (95% CI 0.11, 0.23), and permanent nursing home placement 0.16 (95% CI 0.10, 0.22). Bivariate analysis identified female gender and African-American race as predictors of higher utility scores (p ≦ .05). In multiple regression analysis, only race remained statistically significant (p ≦ .02 for all three outcome variables).
CONCLUSION: Comparisons of African-American values with those of whites concerning defined states of debility demonstrate greater than threefold increases in utility scores. This finding suggests that racial differences need to be taken into account when studying the effects of medical interventions on quality of life.
Similar content being viewed by others

References
Fryback DG, Dasbach EJ, Klein R, et al. The Beaver Dam health outcomes study: initial catalogue of health-state quality factors. Med Decis Making. 1993;13:89–102.
Torrance G, Thomas W, Sackett D. A utility maximization model for the evaluation of health care programs. Health Serv Res. 1972;7(2):118–33.
O’Meara J, McNutt R, Evans A, Moore S, Downs S. A decision analysis of streptokinase plus heparin as compared with heparin alone for deep-vein thrombosis. N Engl J Med. 1994;330:1864–9.
Disch D, Greenberg M, Holzberger P, Malenka D, Birkmeyer J. Managing chronic atrial fibrillation: a Markov decision analysis comparing warfarin, quinidine, and low-dose amiodarone. Ann Intern Med. 1994;120:449–57.
Gage B, Cardinalli A, Albers G, Owens D. Cost-effectiveness of warfarin and aspirin for prophylaxis of stroke in patients with non-valvular atrial fibrillation. JAMA. 1995;274:1839–45.
Ebell M, Warbasse L, Brenner C. Evaluation of the dyspeptic patient: a cost utility study. J Fam Pract. 1997;44:545–55.
Engle V, Graney M. Black and white female nursing home residents: does health status differ? J Gerontology. 1995;50A(4):M190–5.
McKinley E, Garrett J, Evans A, Danis M. Differences in end-of-life decision making among black and white ambulatory cancer patients. J Gen Intern Med. 1996;11:651–6.
Gold M, Franks P, Erickson P. Assessing the health of the nation: the predictive validity of a preference-based measure and selfrated health. Med Care. 1996;34:163–77.
Johnson R, Wolinsky F. Gender, race, and health: the structure of health status among older adults. Gerontologist. 1994;34(1):24–35.
Tell G, Shumaker S, Mittlemark M, Russell G, Hylander B, Burkart J. Social support and health-related quality of life in black and white dialysis patients. ANNA J. 1995;22(3):301–10.
Bechard D, Wetstein L. Assessment of exercise oxygen consumption as preoperative criterion for lung resection. Ann Thorac Surg. 1987;44:344–9.
Smith T, Kinasewitz G, Tucker W, Spillers W, George R. Exercise capacity as a predictor of post-thoracotomy morbidity. Am Rev Respir Dis. 1984;129:730–4.
Morice R, Peters E, Ryan M, Putnam J, Ali M, Roth J. Exercise testing in the evaluation of patients at high risk for complications from lung resection. Chest. 1992;101:356–61.
Bolliger C, Wyser C, Roser H, Soler M, Perruchoud A. Lung scanning and exercise testing for the prediction of postoperative performance in lung resection candidates at increased risk for complications. Chest. 1995;108:341–8.
Kearney D, Lee T, Reilly J, Decamp M, Sugarbaker D. Assessment of operative risk in patients undergoing lung resection: importance of predicted pulmonary function. Chest. 1994;105:753–9.
Busch E, Verazin G, Antkowiak J, Driscoll D, Takita H. Pulmonary complications in patients undergoing thoracotomy for lung carcinoma. Chest. 1994;105:760–6.
Ferguson M, Reeder L, Mick R. Optimizing selection of patients for major lung resection. J Thorac Cardiovasc Surg. 1995;109:275–83.
Ferguson M, Little L, Rizzo L, et al. Diffusing capacity predicts morbidity and mortality after pulmonary resection. J Thorac Cardiovasc Surg. 1988;96:894–900.
Nord E. Methods for quality adjustment of life years. Soc Sci Med. 1992;34(5):559–69.
Simon J, Bruce P. Resampling: a tool for everyday statistical work. Chance: New Directions for Statistics and Computing. 1991;4(1):22–32.
Nease RF Jr, Kneeland T, O’Connor GT, et al. Variation in patient utilities for outcomes of the management of chronic stable angina. JAMA. 1995;273:1185–90.
Markides K. Aging, religiosity, and adjustment: a longitudinal analysis. J Gerontol. 1983;38(5):621–5.
Levin J, Taylor R, Chatters L. Race and gender differences in religiosity among older adults: findings from four national surveys. J Gerontol. 1994;49(3):S137–45.
Thompson M. Willingness to pay and accept risks to cure chronic disease. Am J Public Health. 1986;76(4):392–6.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Cykert, S., Joines, J.D., Kissling, G. et al. Racial differences in patients’ perceptions of debilitated health states. J GEN INTERN MED 14, 217–222 (1999). https://doi.org/10.1046/j.1525-1497.1999.00320.x
Issue Date:
DOI: https://doi.org/10.1046/j.1525-1497.1999.00320.x