
Abstract
OBJECTIVE: To determine, in a representative sample of patients drawn from a variety of hospitals, the degree of adherence to consensus recommendations for anticoagulation among patients with deep vein thrombosis or pulmonary embolism.
DESIGN: Cross-sectional review of a population-based random sample.
SETTING: Twenty-one randomly selected Pennsylvania hospitals.
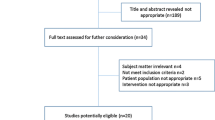
PATIENTS: Of 357 randomly selected Medicare beneficiaries discharged from study hospitals with a diagnosis of deep venous thrombosis or pulmonary embolism during 1992, 43 charts were not reviewed for administrative reasons, 31 were miscoded or not treated with intravenous administration of heparin, and 13 were excluded for other reasons, leaving 270 in the final sample.
MEASUREMENTS AND MAIN RESULTS: Overall, 179 patients (66%, 95% confidence interval [CI] 59%, 72%) received therapeutic anticoagulation (two consecutive partial thromboplastin times more than 1.5 times control) within 24 hours of starting heparin. Platelet counts were checked at least once during the first week of heparin therapy in 66% (95% CI 58%, 74%). At least 5 days of heparin therapy was given to 84% (95% CI 79%, 87%). Among 266 (99%) of the patients receiving warfarin, 193 (72%; 95% CI 63%, 80%) received heparin until the prothrombin time ratio or International Normalized Ratio was therapeutic. Patients who were started on warfarin therapy within 2 days of heparin had decreased length of stay (geometric mean 8.2 vs 9.7 days, p=.003). Compliance varied among hospitals.
CONCLUSIONS: In a wide variety of hospitals, we found fair, but variable, compliance with consensus recommendations for anticoagulation of patients with venous thromboembolic disease. Simple interventions to improve compliance with these recommendations might improve quality of care and reduce costs.
Similar content being viewed by others


References
Anderson FA, Wheeler HB. Physician practices in the management of venous thromboembolism: a community-wide survey. J Vasc Surg. 1992;16:707–14.
Goldhaber SZ, Morpurgo M. Diagnosis, treatment and prevention of pulmonary embolism. JAMA. 1992;268:1727–33.
Hyers TM, Hull RD, Weg JG. Antithrombotic therapy for venous thromboembolic disease. Chest. 1995;108(suppl):S335–51.
Hyers TM, Hull RD, Weg JG. Antithrombotic therapy for venous thromboembolic disease. Chest. 1986;89(suppl):S26–35.
Hyers TM, Hull RD, Weg JG. Antithrombotic therapy for venous thromboembolic disease. Chest. 1989;95(suppl):S37–51.
Hyers TM, Hull RD, Weg JG. Antithrombotic therapy for venous thromboembolic disease. Chest. 1992;102(suppl):S408–25.
Cook DJ, Guyatt GH, Laupacis A, Sackett DL, Goldberg RJ. Clinical recommendations using levels of evidence for antithrombotic agents. Chest. 1995;108(suppl):S227–30.
Gunnarsson PS, Sawyer WT, Montague D, Williams ML, Dupuis RE, Caiola SM. Appropriate use of heparin: empiric vs nomogram-based dosing. Arch Intern Med. 1995;155:526–32.
Cruickshank MK, Levine MN, Hirsh J, Roberts R, Siguenza M. A standard heparin nomogram for the management of heparin therapy. Arch Intern Med. 1991;151:333–7.
Eliott GC, Hiltunen SJ, Suchyta M, et al. Physician-guided treatment compared to a heparin protocol for deep vein thrombosis. Arch Intern Med. 1994;154:999–1004.
Fennerty AG, Thomas P, Backhouse G, Bentley P, Campbell IA. Audit control of heparin treatment. BMJ. 1985;290:27–8.
Wheeler AP, Jaquiss RDB, Newman JH. Physician practices in the treatment of pulmonary embolism and deep venous thrombosis. Arch Intern Med. 1988;148:1321–5.
Raschke RA, Reilly BM, Guidry JR, Fontana JR, Srinivas S. The weight-based heparin dosing nomogram compared with a "standard care" nomogram: a randomized controlled trial. Ann Intern Med. 1993;119:874–81.
Hull RD, Raskob GE, Rosenbloom D, et al. Optimal therapeutic level of heparin therapy in patients with venous thrombosis. Arch Intern Med. 1992;152:1589–95.
Hollingsworth JA, Rowe BH, Brisebois FJ, Thompson PR, Fabris LM. The successful application of a heparin nomogram in a community hospital. Arch Intern Med. 1995;155:2095–2100.
Raschke RA, Gollihare B, Peirce JC. The effectiveness of implementing the weight-based heparin nomogram as a practice guideline. Arch Intern Med. 1996;156:1645–9.
Dalen JE, Hirsh J. Introduction to the Fourth ACCP Consensus Conference on Antithrombotic Therapy. Chest. 1995;108(suppl):S225–6.
Hirsh J, Raschke R, Warkentin TE, Dalen JE, Deykin D, Poller L. Heparin: mechanism of action, pharmacokinetics, dosing considerations, monitoring, efficacy and safety. Chest. 1995;108(suppl):S258–75.
Hirsh J, Dalen JE, Deykin D, Poller L, Bussey H. Oral anticoagulants: mechanism of action, clinical effectiveness, and optimal therapeutic range. Chest. 1995;108(suppl):S231–46.
Diggle PJ, Liang KY, Zeger SL. Analysis of Longitudinal Data. Oxford, UK: Clarendon Press; 1994:146–68.
Gallus A, Tillett J, Jackaman J, Mills W, Wycherley A. Safety and efficacy of warfarin started early after submassive venous thrombosis or pulmonary embolism. Lancet. 1986;2:1293–6.
Hull RD, Raskob GE, Hirsh J, et al. Continuous intravenous heparin compared with intermittent subcutaneous heparin in the initial treatment of proximal-vein thrombosis. N Engl J Med. 1986;315:1109–14.
Anand S, Ginsberg JS, Kearon C, Gent M, Hirsh J. The relation between the activated partial thromboplastin time response and recurrence in patients with venous thrombosis treated with continuous intravenous heparin. Arch Intern Med. 1996;156:1677–81.
Author information
Authors and Affiliations
Additional information
The analyses on which this publication is based were performed Under contract 500-96-P708, entitled “Utilization and Quality Peer Review Organization for the Commonwealth of Pennsylvania,” sponsored by the Health Care Financing Administration, Department of Health and Human Services. The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government. The authors assume full responsibility for the accuracy and completeness of the ideas presented. This article is a direct result of the Health Care Quality Improvement Program initiated by the Health Care Financing Administration, which has encouraged identification of quality improvement projects derived from analysis of patterns of care, and therefore required no special funding on the part of this contractor. Ideas and contributions to the authors concerning experience in engaging with issues presented are welcomed.
Rights and permissions
About this article
Cite this article
Whittle, J., Johnson, P. & Russell Locailo, A. Anticoagulation therapy in patients with venous thromboembolic disease. J GEN INTERN MED 13, 373–378 (1998). https://doi.org/10.1046/j.1525-1497.1998.00117.x
Issue Date:
DOI: https://doi.org/10.1046/j.1525-1497.1998.00117.x