
Abstract
Objective
To assess the ability of echocardiographic data to predict important functional status outcomes in patients with chest pain.
Design
Prospective cohort study.
Setting
A large, urban teaching hospital.
Patients
Three hundred thirty-three patients admitted from the Emergency Department for evaluation of chest pain.
Measurements and Main Results
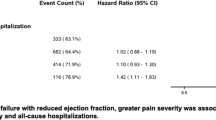
Patients underwent two-dimensional and Doppler echocardiography as well as a face-to-face interview during their initial hospitalization and a telephone interview 1 year thereafter. The interview included the Medical Outcomes Study 36-Item Short Form (SF-36) health inventory, a generic health status instrument with a physical function subscale. The relation between clinical and echocardiographic factors and functional status was explored by univariable and multivariable linear regression and logistic regression analyses. Multiple clinical and echocardiographic factors correlated significantly with functional status measures at 1 year. For the SF-36 score at 1 year, age, male gender, white race, the presence of rales, and a comorbidity score were independently predictors in multivariate analysis; echocardiographic findings of severe left ventricular dysfunction (parameter estimate [PE] −27.6; 95% confidence interval [CI] −43.1, −12.2) and aortic insufficiency (PE −16.7; 95% CI −26.4, −7.0) added independent predictive information. Explanatory power (r 2) for models using clinical and demographic variables was .27 and increased after inclusion of echocardiographic data to an r 2 of .35. Results in the subset of patients (n=148) with acute coronary syndromes such as unstable angina or myocardial infarction were qualitatively similar. Selected factors (rales on examination, electrocardiographic changes suggestive of ischemia, and moderate to severe mitral regurgitation) also predicted which patients would die or have a decline in their functional status. In multivariate analysis, only rales remained an independent predictor of poor outcome (odds ratio 2.4; 95% CI 1.2, 4.5).
Conclusions
Echocardiographic data are correlated with measures of functional status in patients with chest pain, but the ability to predict future functional status from clinical or echocardiographic information is limited. Because functional status cannot be predicted adequately from either patients’ characteristics or echocardiographic testing, it must be assessed directly.
Similar content being viewed by others

References
The Multicenter Post Infarction Research Group Risk stratification and survival after myocardial infarction. N Engl J Med. 1983;309:331–6.
Sanz G, Castener A, Betriu A, et al. Determinants of prognosis in survivors of myocardial infarction. N Engl J Med. 1982;306:1065–70.
Tcheng JE, Jackman JD, Nelson CL, et al. Outcome of patients sustaining acute ischemic mitral regurgitation during myocardial infarction. Ann Intern Med. 1992;117:18–24.
Lehman KG, Francis CK, Dodge HT, and the TIMI Study Group. Mitral regurgitation in early myocardial infarction. Ann Intern Med. 1992;117:10–7.
Fleischmann KE, Goldman L, Robiolio PA et al. Echocardiographic correlates of survival in patients with chest pain. J Am Coll Cardiol. 1994;23(6):1390–6.
Lee TH, Shammash JB, Ribiero JP, et al. Estimation of maximum oxygen uptake from clinical data: performance of the Specific Activity Scale. Am Heart J. 1988;115:203–5.
Caine N, Harrison SCW, Sharples LD, Wallwork J. Prospective study of quality of life before and after coronary artery bypass grafting. BMJ. 1991;302:511–6.
Engler R, Ray R, Higgins CB, et al. Clinical assessment and follow-up of functional capacity in patients with chronic congestive cardiomyopathy. Am J Cardiol. 1982;49:1832–7.
Franciosa JA, Park M, Levine TB. Lack of correlation between exercise capacity and indexes of resting left ventricular performance in heart failure. Am J Cardiol. 1981;47:33–9.
Gorkin L, Norvell NK, Rosen RC, et al. Assessment of quality of life as observed from the baseline data of the Studies of Left Ventricular Dysfunction (SOLVD) trial quality-of-life substudy. Am J Cardiol. 1993;71:1069–73.
Smith RF, Johnson G, Žiesche S, Bhat G, Blankenship K, Cohn JN. Functional capacity in heart failure: comparison of methods for assessment and their relation to other indexes of heart failure. Circulation. 1993;87(suppl VI):VI-88–VI-93.
Goldman L, Weinberg M, Weisberg M, et al. A computer derived protocol to aid in the diagnosis of emergency room patients with acute chest pain. N Engl J Med. 1982;307:588–96.
Goldman L, Cook EF, Brand DA, et al. A computer protocol to predict myocardial infarction in emergency department patients with chest pain. N Engl J Med. 1988;318:797–803.
Lee TH, Rouan G, Weisberg M, et al. Senstivity of routine clinical criteria for diagnosing myocardial infarction within 24 hours of hospitalization. Ann Intern Med. 1987;106:181–6.
Lee TH, Juarez G, Cook EF, et al. Ruling out acute myocardial infarction: a prospective multicenter validation of a 12 hour strategy for patients at low risk. N Engl J Med. 1991;324:1239–46.
Lee TH, Rouan GW, Weisberg MC, et al. Clinical characteristics and natural history of patients with acute myocardial infarction sent home from the emergency room. Am J Cardiol. 1987;60:219–24.
Lee TH, Cook EF, Weisberg MC, Brand DA, Rouan GW, Goldman L. Candidates for thrombolysis among emergency department patients with acute chest pain: the Multicenter Chest Pain Study experience. Ann Intern Med. 1989;110:957–62.
Rouan GW, Lee TH, Cook EF, Brand DA, Weisberg MC, Goldman L. Clinical characteristics and outcome of acute myocardial infarction in patients with initially normal or nonspecific electrocardiograms. Am J Cardiol. 1989;64:1087–92.
White LD, Lee TH, Cook EF, et al. Comparison of the natural history of new onset and exacerbated chronic ischemic heart disease. J Am Coll Cardiol. 1990;16:304–10.
Lee TH, Ting HH, Shammash JB, Soukup JR, Goldman L. Longterm survival of emergency department patients with chest pain. Am J Cardiol. 1992;69:145–51.
Ware JE Jr, Sherbourne CD. The MOS 36-Item Short-Form health survey (SF-36). Med Care. 1992;30:473–82.
Helmeke F, Nanda NC, Hsuing MC, et al. Color Doppler assessment of mitral regurgitation with orthogonal planes. Circulation. 1987;75:175–83.
Nishimura RA, Reeder GS, Miller FA, et al. Prognostic value of predischarge 2-dimensional echocardiogram after acute myocardial infarction. Am J Cardiol. 1984;53:429–32.
Nishimura RA, Tajik AJ, Shub C, Miller FA, Illstrup DM, Harrison CE. Role of two-dimensional echocardiography in the prediction of in-hospital complications after acute myocardial infarction. J Am Coll Cardiol. 1984;4:1080–7.
Edwards WD, Tajik AJ, Seward JB. Standardized nomenclature and anatomic basis for regional tomographic analysis of the heart. Mayo Clinic Proc. 1981;56:479–97.
Fleischmann KE, Lee TH, Come PC, et al. Echocardiographic prediction of complications in patients with chest pain. Am J Cardiol. 1997;79:292–8.
Fletcher AE, Hunt BM, Bulpitt CJ. Evaluation of quality of life in clinical trials of cardiovascular disease. J Chron Dis. 1987;40:557–69.
Ware JE, Bayliss MS, Rogers WH, Kosinski M, Tarlov AR. Differences in 4-year health outcomes for elderly and poor. chronically ill patients treated in HMO and fee-for-service systems: results from the Medical Outcomes Study. JAMA. 1996;276:1039–47.
Nelson CL, Herdon JE, Mark DB, Pryor DB, Califf RM, Hlatky M. Relation of clinical and angiographic factors to functional status as measured by the Duke Activity Status Index. Am J Cardiol. 1991;68:973–5.
Author information
Authors and Affiliations
Additional information
Dr. Fleischmann is the recipient of a Clinical Investigator Development Award (IK08HL02964-01) from the National Heart, Lung and Blood Institute.
Rights and permissions
About this article
Cite this article
Fleischmann, K.E., Lee, R.T., Come, P.C. et al. Clinical and echocardiographic correlates of health status in patients with acute chest pain. J GEN INTERN MED 12, 751–756 (1997). https://doi.org/10.1046/j.1525-1497.1997.07160.x
Issue Date:
DOI: https://doi.org/10.1046/j.1525-1497.1997.07160.x