
Abstract
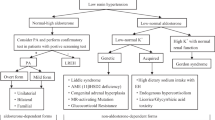
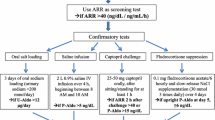
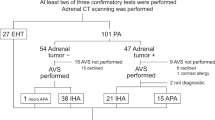
Screening for primary hyperaldosteronism (PHA) is often indicated in individuals with resistant hypertension or hypokalaemia. However, in the far larger subset of the hypertensive population who do not fit into these criteria, the evidence for screening is conflicting and dependent on the disease prevalence. The purpose of this study was to examine the prevalence of PHA in a large population with mild to moderate hypertension and without hypokalaemia using a carefully controlled study protocol including a normotensive control population. Hypertensive subjects underwent medication washout and both hypertensive and normotensive subjects placed on a high-sodium diet prior to biochemical and haemodynamic testing. Study specific cutoff values were based on results from the normotensive population studied under identical conditions. A screening test (serum aldosterone/PRA ratio [ARR]>25 with a serum aldosterone level >8 ng/dl) was followed by a confirmatory test (urine aldosterone excretion rate [AER] >17 μg/24 h) to demonstrate evidence of PHA. An elevated ARR with a concomitant elevated serum aldosterone was present in 26 (7.5%) individuals. Of these, 11 (3.2%) had an elevated AER, consistent with evidence of PHA. Individuals with PHA had higher blood pressure and lower serum potassium levels while on a high-sodium diet. Sodium restriction neutralized these differences between PHA and essential hypertensives. The prevalence of PHA in this mild to moderate hypertensive population without hypokalaemia is at most 3.2%, a rate that might lead to excessive false positives with random screening in comparable populations. Hyperaldosteronism, when present, is responsive to sodium restriction.

Similar content being viewed by others
References
Conn JW . Primary aldosteronism. J Lab Clin Med 1955; 45: 661–664.
Williams JS, Williams GH . 50th anniversary of aldosterone. J Clin Endocrinol Metab 2003; 88: 2364–2372.
McAreavey D, Murray GD, Lever AF, Robertson JI . Similarity of idiopathic aldosteronism and essential hypertension. A statistical comparison. Hypertension 1983; 5: 116–121.
Fraser R, Lever AF, Brown JJ, Robertson JI . Cautions over idiopathic aldosteronism. Lancet 2001; 358: 332.
Kaplan NM . Cautions over the current epidemic of primary aldosteronism. Lancet 2001; 357: 953–954.
Connell JM . Is there an epidemic of primary aldosteronism? J Hum Hypertens 2002; 16: 151–152.
Padfield PL . Primary aldosteronism, a common entity? the myth persists. J Hum Hypertens 2002; 16: 159–162.
Vasan RS, Evans JC, Larson MG, Wilson PW, Meigs JB, Rifai N et al. Serum aldosterone and the incidence of hypertension in nonhypertensive persons. N Engl J Med 2004; 351: 33–41.
Yakovlevitch M, Black HR . Resistant hypertension in a tertiary care clinic. Arch Intern Med 1991; 151: 1786–1792.
Litchfield WR, Dluhy RG . Primary aldosteronism. Endocrinol Metab Clin North Am 1995; 24: 593–612.
Ganguly A . Prevalence of primary aldosteronism in unselected hypertensive populations: screening and definitive diagnosis. J Clin Endocrinol Metab 2001; 86: 4002–4004.
Stowasser M, Gordon RD . Primary aldosteronism – careful investigation is essential and rewarding. Mol Cell Endocrinol 2004; 217: 33–39.
Young Jr WF . Minireview: primary aldosteronism – changing concepts in diagnosis and treatment. Endocrinology 2003; 144: 2208–2213.
Gordon RD, Stowasser M, Tunny TJ, Klemm SA, Rutherford JC . High incidence of primary aldosteronism in 199 patients referred with hypertension. Clin Exp Pharmacol Physiol 1994; 21: 315–318.
Gordon RD, Ziesak MD, Tunny TJ, Stowasser M, Klemm SA . Evidence that primary aldosteronism may not be uncommon: 12% incidence among antihypertensive drug trial volunteers. Clin Exp Pharmacol Physiol 1993; 20: 296–298.
Hiramatsu K, Yamada T, Yukimura Y, Komiya I, Ichikawa K, Ishihara M et al. A screening test to identify aldosterone-producing adenoma by measuring plasma renin activity. Results in hypertensive patients. Arch Intern Med 1981; 141: 1589–1593.
Streeten DH, Tomycz N, Anderson GH . Reliability of screening methods for the diagnosis of primary aldosteronism. Am J Med 1979; 67: 403–413.
Mulatero P, Stowasser M, Loh KC, Fardella CE, Gordon RD, Mosso L et al. Increased diagnosis of primary aldosteronism, including surgically correctable forms, in centers from five continents. J Clin Endocrinol Metab 2004; 89: 1045–1050.
Mulatero P, Rabbia F, Milan A, Paglieri C, Morello F, Chiandussi L et al. Drug effects on aldosterone/plasma renin activity ratio in primary aldosteronism. Hypertension 2002; 40: 897–902.
Schwartz GL, Turner ST . Screening for primary aldosteronism in essential hypertension: diagnostic accuracy of the ratio of plasma aldosterone concentration to plasma renin activity. Clin Chem 2005; 51: 386–394.
Fardella CE, Mosso L, Gomez-Sanchez C, Cortes P, Soto J, Gomez L et al. Primary hyperaldosteronism in essential hypertensives: prevalence, biochemical profile, and molecular biology. J Clin Endocrinol Metab 2000; 85: 1863–1867.
Loh KC, Koay ES, Khaw MC, Emmanuel SC, Young Jr WF . Prevalence of primary aldosteronism among Asian hypertensive patients in Singapore. J Clin Endocrinol Metab 2000; 85: 2854–2859.
Stowasser M . Primary aldosteronism: revival of a syndrome. J Hypertens 2001; 19: 363–366.
Hambling C, Jung RT, Browning MC, Gunn A, Anderson JM . Primary hyperaldosteronism – evaluation of procedures for diagnosis and localization. Q J Med 1993; 86: 383–392.
Naomi S, Iwaska T, Umeda T, Inoue J, Hamasaki S, Miura F et al. Clinical evaluation of the captopril screening test for primary aldosteronism. Jpn Heart J 1985; 26: 549–556.
Hollenberg NK, Moore T, Shoback D, Redgrave J, Rabinowe S, Williams GH . Abnormal renal sodium handling in essential hypertension. Relation to failure of renal and adrenal modulation of responses to angiotensin II. Am J Med 1986; 81: 412–418.
Gordon RD . Primary aldosteronism. J Endocrinol Invest 1995; 18: 495–511.
Raji A, Williams GH, Jeunemaitre X, Hopkins PN, Hunt SC, Hollenberg NK et al. Insulin resistance in hypertensives: effect of salt sensitivity, renin status and sodium intake. J Hypertens 2001; 19: 99–105.
Hopkins PN, Lifton RP, Hollenberg NK, Jeunemaitre X, Hallouin MC, Skuppin J et al. Blunted renal vascular response to angiotensin II is associated with a common variant of the angiotensinogen gene and obesity. J Hypertens 1996; 14: 199–207.
Emanuel RL, Cain JP, Williams GH . Double antibody radioimmunoassay of renin activity and angiotensin II in human peripheral plasma. J Lab Clin Med 1973; 81: 632–640.
Underwood RH, Williams GH . The simultaneous measurement of aldosterone, cortisol, and corticosterone in human peripheral plasma by displacement analysis. J Lab Clin Med 1972; 79: 848–862.
Calhoun DA, Nishizaka MK, Zaman MA, Thakkar RB, Weissmann P . Hyperaldosteronism among black and white subjects with resistant hypertension. Hypertension 2002; 40: 892–896.
Magill SB, Raff H, Shaker JL, Brickner RC, Knechtges TE, Kehoe ME et al. Comparison of adrenal vein sampling and computed tomography in the differentiation of primary aldosteronism. J Clin Endocrinol Metab 2001; 86: 1066–1071.
Ganguly A . Primary aldosteronism. N Engl J Med 1998; 339: 1828–1834.
Bravo EL, Tarazi RC, Dustan HP, Fouad FM, Textor SC, Gifford RW et al. The changing clinical spectrum of primary aldosteronism. Am J Med 1983; 74: 641–651.
Kunzelmann K, Mall M . Electrolyte transport in the mammalian colon: mechanisms and implications for disease. Physiol Rev 2002; 82: 245–289.
Mosso L, Carvajal C, Gonzalez A, Barraza A, Avila F, Montero J et al. Primary aldosteronism and hypertensive disease. Hypertension 2003; 42: 161–165.
Rossi E, Regolisti G, Negro A, Sani C, Davoli S, Perazzoli F . High prevalence of primary aldosteronism using postcaptopril plasma aldosterone to renin ratio as a screening test among Italian hypertensives. Am J Hypertens 2002; 15: 896–902.
Gordon MS, Williams GH, Hollenberg NK . Renal and adrenal responsiveness to angiotensin II: influence of beta adrenergic blockade. Endocr Res 1992; 18: 115–131.
Manhem P, Hokfelt B . Prolonged clonidine treatment: catecholamines, renin activity and aldosterone following exercise in hypertensives. Acta Med Scand 1981; 209: 253–260.
Brown MJ, Hopper RV . Calcium-channel blockade can mask the diagnosis of Conn's syndrome. Postgrad Med J 1999; 75: 235–236.
Zhou BF, Stamler J, Dennis B, Moag-Stahlberg A, Okuda N, Robertson C et al. Nutrient intakes of middle-aged men and women in China, Japan, United Kingdom, and United States in the late 1990s: the INTERMAP study. J Hum Hypertens 2003; 17: 623–630.
Adler GK, Moore TJ, Hollenberg NK, Williams GH . Changes in adrenal responsiveness and potassium balance with shifts in sodium intake. Endocr Res 1987; 13: 419–445.
Acknowledgements
This work was supported by the National Institutes of Health grants HL47651, HL59424, HL77234, DK63214, Specialized Center of Research in Hypertension (HL55000), National Center for Research Resources (General Clinical Research Centers) in Boston (M01 RR 02635) and Salt Lake City (M01 RR 00064) and the Department of Veterans Affairs- Health Services Research and Development (TEL-02-100). Dr J Williams was in part supported by a Brigham and Women's Hospital Research Council Dual-mentorship grant. We gratefully acknowledge the assistance of the dietary, nursing, administrative and laboratory staffs of the clinical research centers.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Williams, J., Williams, G., Raji, A. et al. Prevalence of primary hyperaldosteronism in mild to moderate hypertension without hypokalaemia. J Hum Hypertens 20, 129–136 (2006). https://doi.org/10.1038/sj.jhh.1001948
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jhh.1001948
- Springer Nature Limited
Keywords
This article is cited by
-
Diagnosis and management of primary hyperaldosteronism in patients with hypertension: a practical approach endorsed by the British and Irish Hypertension Society
Journal of Human Hypertension (2023)
-
Primary Aldosteronism: a Continuum from Normotension to Hypertension
Current Cardiology Reports (2021)
-
Therapeutic Outcomes with Surgical and Medical Management of Primary Aldosteronism
Current Cardiology Reports (2021)
-
Salt intake in mineralocorticoid receptor antagonist-treated primary aldosteronism: foe or ally?
Hormones (2020)
-
Primary aldosteronism in patients with acute stroke: prevalence and diagnosis during initial hospitalization
BMC Neurology (2016)