
Abstract
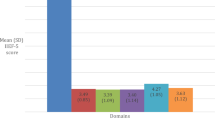
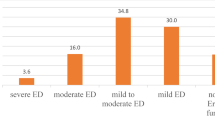
The prevalence and correlates of erectile dysfunction (ED) in developing countries are largely unknown. Our objectives were to determine the prevalence and associated factors of ED in three countries (Pakistan, Egypt, Nigeria) that represent very different cultures. Men 35–70y of age seeking primary medical care answered a structured questionnaire adapted to reflect local cultures. Degree of ED was categorized as ‘none,’ ‘mild,’ ‘moderate,’ or ‘complete.’ The age-adjusted prevalence rates of ED among men attending primary care clinics was 57.4% in Nigeria, 63.6% in Egypt, and 80.8% in Pakistan. Older age, diabetes, peptic ulcers, prostate disease, depression-related symptoms, and caffeine consumption were independently associated with increased prevalence of ED, whereas being moderately active to very active at work (hard physical labor) and during leisure time (strenuous exercise) was associated with half the prevalence of moderate-to-complete ED. Our multicultural study demonstrates that in every country studied, high proportions of men older than age 35 have some degree of ED (57–81%). Both severity and prevalence increase consistently with age. Factors associated with ED are similar, but their distribution differs across countries.

Similar content being viewed by others

References
National Institutes of Health Consensus Development Panel on Impotence. Proceedings of a conference held December 7–9, 1992, Bethesda, MD. JAMA 1993; 270: 83–90.
Feldman HA et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol 1994; 151: 54–61.
Melman A, Gingell JC . The epidemiology and pathophysiology of erectile dysfunction. J Urol 1999; 161: 5–11.
Laumann EO, Paik AMA, Rosen RC . Sexual dysfunction in the United States: prevalence and predictors. JAMA 1999; 281: 537–544.
Bosch R et al. Erectile dysfunction in a community-based sample of men aged 50–75 years: prevalence and risk factors. J Urol 1999; 161(4 Suppl): 178 [Abstract 687].
Ansong KS, Lewis C, Jenkins P, Bell J . Epidemiology of erectile dysfunction: a community-based study in rural New York State. Ann Epidemiol 2000; 10: 293–296.
Chew KK et al. Erectile dysfunction in general medicine practice: prevalence and clinical correlates. Int J Impot Res 2000; 12: 41–45.
Pinnock CB, Stapleton AMF, Marshall VR . Erectile dysfunction in the community: a prevalence study. Med J Aust 1999; 171: 353–357.
Read S, King M, Watson J . Sexual dysfunction in primary medical care: prevalence, characteristics, and detection by the general practitioner. J Public Health Med 1997; 19: 387–391.
Macfarlane GJ et al. The relationship between sexual life and urinary condition in the French community. J Clin Epidemiol 1996; 49: 1171–1176.
Koskimaki J, Hakama M, Huhtala H, Tammela TLJ . Effect of erectile dysfunction on frequency of intercourse: a population based prevalence study in Finland. J Urol 2000; 164: 367–370.
Kongkanand A, the Thai Erectile Dysfunction Study Group. Prevalence of erectile dysfunction in Thailand. Int J Androl 2000; 23(Suppl 2): 77–80.
Braun M et al. Epidemiology of erectile dysfunction: results of the ‘Cologne Male Survey.’ Int J Impot Res 2000; 12: 305–311.
Glasser DB et al. The prevalence of erectile dysfunction in four countries: Italy, Brazil, Malaysia, Japan. Presented at: 8th World Meeting on Impotence Research, Amsterdam, the Netherlands, August 25–28, 1998.
Diokno AC, Brown MB, Herzog AR . Sexual function in the elderly. Arch Intern Med 1990; 150: 197–200.
Sullivan ME, Keoghane SR, Miller MAW . Vascular risk factors and erectile dysfunction. BJU Int 2001; 87: 838–845.
Sullivan ME et al. Does severity of ischaemic coronary disease correlate with erectile function? Int J Impot Res 1998; 10: 75 [Letter].
Mulligan T, Retchin SM, Chinchilli VM, Bettinger CB . The role of aging and chronic disease in sexual dysfunction. J Am Geriatr Soc 1988; 36: 520–524.
Bansal S . Sexual dysfunction in hypertensive men. A critical review of the literature. Hypertension 1988; 12: 1–10.
Wabrek AJ, Burchell RC . Male sexual dysfunction associated with coronary heart disease. Arch Sex Behav 1980; 9: 59.
Kayigil O, Atahan O, Metin A . Multifactorial evaluation of diabetic erectile dysfunction. Int Urol Nephrol 1996; 28: 717.
Shabsigh R et al. Increased incidence of depressive symptoms in men with erectile dysfunction. Urology 1998; 52: 848–852.
Mannino DM, Klevens RM, Flanders WD . Cigarette smoking: an independent risk factor for impotence? Am J Epidemiol 1994; 140: 1003–1008.
Rimm EB, Bacon C, Giovannucci EL, Kawachi I . Body weight, physical activity, and alcohol consumption in relation to erectile dysfunction among US male health professionals free of major chronic diseases. J Urol 2000; 163(Suppl 4): 241 [Abstract 1073].
Bacon C, Mittelman MA, Glasser DB, Rimm EB . Can lifestyle factors help prevent erectile dysfunction? Eur Urol 2001; 29(Suppl 5): 17.
Bacon C, Mittelman MA, Glasser DB, Rimm EB . A large prospective study of risk factors for change in erectile function among men over age 50. J Urol 2001; 165(Suppl): 219 [Abstract 903].
Dunn KM, Croft PR, Hackett GI . Association of sexual problems with social, psychological, and physical problems in men and women: a cross sectional population survey. J Epidemiol Commun Health 1999; 53: 144–148.
Parazzini F et al. Frequency and determinants of erectile dysfunction in Italy. Eur Urol 2000; 37: 43–49.
Fedele D et al. Incidence of erectile dysfunction in Italian men with diabetes. J Urol 2001; 166: 1368–1371.
Klein R et al. Prevalence of self-reported erectile dys-function in people with long-term IDDM. Diabetes Care 1996; 19: 135–141.
Araujo AB et al. The relationship between depressive symptoms and male erectile dysfunction: cross-sectional results from the Massachusetts Male Aging Study. Psychosom Med 1998; 60: 458–465.
Weissman MM . Assessing depressive symptoms in five psychiatric populations: a validation study. Am J Epidemiol 1977; 106: 203–214.
SAS/STAT User's Guide, Version 6, 4th ed. SAS Institute, Inc: Cary, NC, 1989.
U.S. Census Bureau, Census, 2000. http://factfinder.census.gov/bf.
Feldman HA et al. Construction of a surrogate variable for impotence in the Massachusetts Male Aging Study. J Clin Epidemiol 1994; 47: 457–467.
Acknowledgements
This study was supported by a research grant from Pfizer Inc.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shaeer, K., Osegbe, D., Siddiqui, S. et al. Prevalence of erectile dysfunction and its correlates among men attending primary care clinics in three countries: Pakistan, Egypt, and Nigeria. Int J Impot Res 15 (Suppl 1), S8–S14 (2003). https://doi.org/10.1038/sj.ijir.3900971
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ijir.3900971
- Springer Nature Limited
Keywords
This article is cited by
-
Association between maternal decision-making and mental health and the nutritional status of children under 6 years of age in sub-urban Nigeria
BMC Public Health (2023)
-
Early childhood caries: Are maternal psychosocial factors, decision-making ability, and caries status risk indicators for children in a sub-urban Nigerian population?
BMC Oral Health (2021)
-
Psychosocial, education, economic factors, decision-making ability, and caries status of mothers of children younger than 6 years in suburban Nigeria
BMC Oral Health (2020)
-
Prevalence of erectile dysfunction and associated factors among diabetic men attending the diabetic clinic at Felege Hiwot Referral Hospital, Bahir Dar, North West Ethiopia, 2016
BMC Research Notes (2018)
-
Physical inactivity, gender and culture in Arab countries: a systematic assessment of the literature
BMC Public Health (2018)