
Abstract
The concurrent additional tasking impacts the walking performance, and such impact is even greater in individuals with mild cognitive impairment (MCI) than in healthy elders. However, effective training program to improve dual task walking ability for the people with MCI is not immediately provided. Therefore, this study aimed to determine the effects of cognitive and motor dual task walking training on dual task walking performance and the responding brain changes in older people with MCI. Thirty older adults with MCI were randomly allocated to receive 24 sessions of 45-min cognitive dual task training (CDTT, n = 9), motor dual task training (MDTT, n = 11), or conventional physical therapy (CPT, n = 10). Gait performance and brain activation during single and dual task walking, and cognitive function assessed by trail-making test (TMT-A, B) and digit span test were measured at pre-, post-test, and 1-month follow-up. Both CDTT and MDTT improved dual task walking with responding activation changes in specific brain areas. The improvements in motor dual task walking performance after both dual task trainings were significantly better than after CPT in the older adults with MCI. Both cognitive and motor dual task training were feasible and beneficial to improve dual task walking ability in older adults with MCI.
Trial Registration: The trial was registered to Thai Clinical Trial Registry and the registration number is TCTR20180510002 (first registration date: 10/05/2018).
Similar content being viewed by others

Introduction
Dual task walking, such as talking or carrying a bag while walking, is essential in daily life. However, both cognitive and motor dual task impact the walking performance, including decreased speed, increased stride time and stride time variability1,2,3, especially in the older population4. The impaired gait performance may indicate a risk of fall5,6, which is an important issue for the aged populations. As dual task walking may be affected by motor ability7, growing evidence demonstrated that the gait performances highly correlated with general cognitive function in the healthy older population3. Prefrontal cortex (PFC) plays a crucial role in cognitive function, and was evident to be involved in dual tasking8,9. Increased activation in PFC was observed during dual task walking in healthy adults, and older adults tended to activate more compared to younger participants10. Other motor brain areas such as premotor cortex (PMC) and supplemental motor area (SMA) were also found to activate during dual task walking, which were responsible for stabilizing gait and adapting walking speed11,12,13,14.
Cognitive impairment in aging population has drawn growing attention in the recent decade. Mild cognitive impairment (MCI) is a brain function syndrome involving the onset and evolution of cognitive impairments beyond those expected based on the age and education of the individual15. In people with MCI, decreased speed, increased stride time, variability were observed during cognitive dual task walking as compared with single walking, with inconclusive results in PFC activation16,17,18,19,20,21. The influence of additional task on walking was even greater in individuals with MCI than in healthy elders17,19,21, which may further impact their daily activities and increase fall risks. Thus, dual task walking ability should be addressed especially in cognitive impaired population. However, the effective training program to improve dual task walking ability is not immediately provided.
Dual task training is designed in accordance with the principles of motor learning and task specificity, to improve the dual task performance22. The beneficial effects of dual task training have been demonstrated in several populations with different clinical conditions23. Specifically, cognitive dual task training has been reported to exert beneficial effects on cognitive and physical functions in older adults with and without cognitive impairment24,25. The overview of systematic reviews has further suggested that such training program is preferred over single task training as targeting motor performance under dual task situation in healthy older adults24. However, the effect of dual task training on dual task walking performance in older adults with MCI is not known. Furthermore, whether different dual task training would exert different effects in the MCI population needs further elucidation for possible clinical applications. Therefore, this study aimed to determine the effects of cognitive and motor dual task walking training on dual task walking performance and responding brain changes in older adults with MCI. We hypothesized that cognitive and motor dual task walking training would provide task-specific effects on dual task walking performance in older adults with MCI, and the brain changes would correlate to the improvement of walking performance after training.
Results
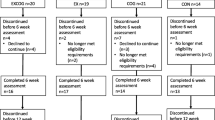
Forty-five older adults with MCI who met the eligibility criteria were recruited, and 14 of them declined to participate due to personal reasons. Thirty-one participants were randomly assigned to the conventional physical therapy group (CPT, n = 10), cognitive dual task training group (CDTT, n = 10), or motor dual task training group (MDTT, n = 11). One in the CDTT group dropped out before the pre-test assessment. Therefore, total of 30 participants completed the training sessions and post-test measurements. One in the CPT group and one in the CDTT group missed the follow-up assessment because of transportation issue. The study flow chart was shown in Fig. 1.

Study flow chart. CPT conventional physical therapy, CDTT cognitive dual task training, MDTT motor dual task training.
The median age for all participants was 79.5 (interquartile range, IQR = 74.3–85.3) years old. The median mini-mental state examination (MMSE) scores were 28 (IQR = 27–29) and the median Montreal cognitive assessment (MoCA) scores were 22 (IQR = 20–23.8). No significant differences among groups were found in basic data and measures at pre-test (Table 1).
Cognitive dual task walking
Table 2 shows the results of cognitive dual task walking performance after different interventions. The CDTT resulted in significant within-group improvements in speed, cadence, stride length, and stride time. The improvement in stride length correlated with the increase in PFC (rho = 0.850, p = 0.007), bilateral PMC (left PMC: rho = 0.778, p = 0.023; right PMC: rho = 0.838, p = 0.009) and SMA (rho = 0.910, p = 0.002) after CDTT. Significant within-group training effects of MDTT were observed on all the gait parameters, except for temporal variability. However, the improvement in gait performance after MDTT did not correlate significantly with the change in brain activation. There was no significant difference across time in the CPT group. The training effects on speed, stride length, and spatial variability were significantly better after MDTT than CPT at follow-up.
Motor dual task walking
The motor dual task gait performance in three groups are presented in Table 3. The significant improvements in speed, cadence, stride length, stride time, spatial variability, and dual task cost (DTC) of gait speed were found in the MDTT group. Only the change in spatial variability correlated with PFC after MDTT (rho = 0.857, p = 0.007). On the other hand, CDTT also provided beneficial effects on cadence and stride time during motor dual task walking. The improvement in cadence correlated with PFC (rho = 0.810, p = 0.015) and right PMC (rho = 0.714, p = 0.047), and the improvement in stride time correlated with PFC (rho = − 0.874, p = 0.005) and right PMC (rho = − 0.934, p = 0.001) after CDTT. No significant improvement was shown in the CPT group. The between-group differences among three groups were found significant at both post-test and follow-up assessment. Both MDTT and CDTT provided greater improvements on cadence and stride time than CPT at the end of the training programs. The improvement in cadence remained for 4 weeks after CDTT, while the changes in speed, stride length and spatial variability in the MDTT group were significantly greater than that in the CPT group at follow-up.
Single walking
The speed, cadence, stride length, and stride time during single walking were improved after CDTT. Significant within-group improvements in speed, cadence, stride length, spatial variability, and stride time were found in the MDTT group. No significant change was found after CPT. Furthermore, the training effects on cadence and stride time after CDTT was significantly better than CPT at follow-up (Table 4). However, the improvements in gait performance did not significantly correlate with the change in brain activation after the cognitive or motor dual task training.
Cognitive function
There were no significant changes in cognitive function after CDTT, MDTT or CPT, except for the trail-making test part B (TMT-B). The time needed to complete TMT-B was significantly less after 24 sessions of MDTT, and such effect remained at the 4-week follow-up (Table 5).
Discussion
Although many studies have examined the interventions on cognitive function in individuals with MCI26,27,28, few have explored the effect of different training on gait performance29. This study demonstrated both cognitive and motor dual task trainings improved dual task walking and single walking performance. Furthermore, the effects of both dual task trainings on the motor dual task walking performance were superior to CPT in the older adults with MCI. Nevertheless, only MDTT resulted in significantly superior effect at 1-month on both dual task walking performances as compared with CPT. In addition, improvements in dual task gait performance correlated with the activations in the specific brain areas.
As dual task walking ability is essential for daily activities, previous studies have shown that simultaneous cognitive and aerobic training improved cognitive dual task walking ability more than physical training in people with MCI30. However, the virtual reality-based dual task balance training did not benefit the Timed Up-and-Go test under dual task condition in the institutionalized older persons with MCI31. In present study, both cognitive and motor dual task trainings improved walking performance under dual task conditions, but the CPT, as practicing single tasks consecutively, did not. Present results were consistent with results of other studies in different populations32,33, suggesting the specific dual task training effect over single task training. Moreover, the improvements in gait speed (median: 18.1 and 17.3 cm/s for cognitive and motor dual task walking, respectively) were higher than the minimum detectable change value (16 cm/s) during dual task walking34, which may indicate the clinical importance of the favorable results.
It draws our attention that motor and cognitive dual task training did not result in distinct effects in accordance with the dual task types in the MCI population. Previously we found that CDTT improved cognitive dual task gait performance and MDTT improved motor dual task gait performance in people with chronic stroke35. The reasons for inconsistent results between participants with MCI and stroke are not known. We further noted the lasting effects (at 1-month follow-up) on dual task walking performance seemed to be evident after MDTT, while the lasting effects on single walking performance was significant after CDTT. The concept of task priority may lend some explanations for such results after motor and cognitive dual task training. Previous studies proposed the prioritization of dual task performance depended on the complexity of the posture-related task as well as the additional tasks36,37,38. In present study, the additional cognitive tasks may be too challenging for our participants to maintain the posture control and gait stability, thus they needed to allocate attentional resources on posture and gait control during CDTT. As a result, we observed the significant improvement in single walking performance after CDTT with little changes in cognitive function tested by TMT and digit span test. The insignificant improvements in cognitive function as demonstrated by executive and memory function were also noted in the meta-analysis study after combined cognitive-physical intervention39.
On the other hand, the additional motor tasks did not seem very complex or difficult, so the participants may not need to prioritize the additional task over the walking during MDTT. In other words, MDTT might benefit from minimizing the crosstalk, which reduced the requirement for attention on the additional motor tasks during training40. Therefore, the participants could have ample opportunity to practice the integration of two simultaneous tasks, which resulted in superior beneficial effects on dual task walking performance even after 1-month post training. In addition, it should be mentioned the implications of changes in gait variability after MDTT. Studies showed that the gait variability was able to predict fall risk, and was related to executive function in the aging populations with and without cognitive impairment41. In line with the improvement in dual task walking performance, we noticed the beneficial effects on TMT-B after MDTT. As mentioned earlier, cognitive flexibility plays an important role in dual tasking in the aged population42, and TMT-B is used to assess executive function, specifically as the ability of cognitive flexibility43. Taking together, our MDTT program improved dual task walking ability by the adaptation of dual tasking and possibly decreased fall risks in older adults with MCI.
It is worth mentioning that our two dual task training programs were also able to exert clinically important improvements in single walking speed, as the median change values (15.1 and 16.8 cm/s at follow-up in CDTT and MDTT group, respectively) were in the range of minimal clinical important differences (10–20 cm/s)44. By contrast, CPT did not improve any walking performance measured in present study. A meta-analysis demonstrated multi-modal training, similar to CPT in present study, could improve single walking performance with a relatively long period of training, e.g. 90 min per session for 40 sessions in older adults with MCI or mild dementia45. Our CPT programs were 45 min per session, including 15 min of gait training, for a total of 24 sessions. On the other hand, our dual task training combined either cognitive or motor task concurrently with gait training throughout the 45-min session, and resulted in single walking improvement. Therefore, to improve single walking performance may need relatively long duration of walking activity.
Although both cognitive and motor dual task training exerted beneficial effects on dual task walking ability, the underlying brain changes in response to different types of dual task training seemed different, which may indicate different strategies for the improvements46. According to our results, positive correlations between the changes in gait performance and brain activation after CDTT, suggesting that CDTT enhanced the brain activations in prefrontal and motor-associated brain areas extensively to provide positive effects. In line with our findings, previous study proposed that older adults increased the activation in SMA and frontal cortex as a compensatory strategy to ensure a better task performance47. PMC and SMA played important roles in gait control, and prioritizing the walking tasks during CDTT might specifically induce activations of these brain areas. Regarding the PFC activation, although it may reach the resource ceiling for cognitive tasks in the aged population, Logan et al. demonstrated that providing external instructions potentially helped to reverse the deactivation of frontal cortex48. Thus, we speculate that CDTT may increase the recruitment of PFC resource by verbal cues from the therapist, which may partially contribute to the improvements in walking performance. As for the MDTT, the reduction in spatial variability correlated with the decreased activation in PFC during motor dual task walking after training, which may be explained by the cortical adaptation for the processing of dual-tasking49. Previous studies demonstrated decreased PFC activation at late stage of motor learning, accompanied by the shifting of neural networks50,51 to promote neural efficiency even after the learning process46. We thus think the beneficial effects on dual task walking of MDTT may be related to the enhancement of neural efficiency, and that of CDTT may be related to the recruitment of neural resources.
There were several limitations in this study should be noted. First, the sample size was relatively small in each training group, and there were drop-outs at the 1-month follow-up. To address this issue, we applied the non-parametric statistical methods with Bonferroni adjustment and intention-to-treat in order to draw unbiased conclusion. The significances in the between-group comparisons were with large effect size, which may help to validate the training effects. Second, the task priority was not specifically emphasized during our dual task training programs, and the instructions were given according to the performance for each participant during training. Further studies are needed to investigate the influences of task prioritization and task complexity on training effects to establish a comprehensive guideline for the application of dual task training.
Our study provides the first evidence about different dual task trainings on dual task walking performance and related brain changes in individuals with MCI using three parallel groups with randomized controlled design. Both cognitive and motor dual task training for 24 sessions improved walking performance under single and dual task condition, while the CPT did not exert significant change in gait performance. Furthermore, the changes in responding brain activation during walking were related to dual task walking improvement after CDTT and MDTT. The possible mechanisms for the different dual task training should be investigated and validated in future studies.
Methods
Study design
This study was a three-arm parallel single blinded (assessor blinded), randomized controlled trial. The Block of 6 randomization was used, and the random allocation sequence was generated via sealed envelope drawn by a person who was not involved in the study. Participants were enrolled and randomly assigned by the researchers to one of the three groups: cognitive dual-task training (CDTT), motor dual-task training (MDTT) or conventional physical therapy group (CPT). A sample of 30 participants was suggested to be sufficient with effect size of 0.4 (medium effect size), power of 0.80 and a two-tailed alpha level of 0.05 using G*Power version 3.1. The basic data including age, gender, educational level, mini-mental state examination (MMSE) scores and Montreal cognitive assessment (MoCA) scores were obtained and assessed before the interventions. All participants received 45 min of training according to their group assignment, 3 sessions per week for a total of 24 sessions instructed by a physical therapist. All outcomes were measured before (pre) and after completing 24 sessions of interventions (post), and at 1-month follow-up assessment (follow-up). The study protocol was approved by the Institutional Review Board of National Yang-Ming University (approval number: YM107032F). The trial was prospectively registered to Thai Clinical Trial Registry (TCTR20180510002) on 10/05/2018 and conformed to the CONSORT checklist. All experiments were performed in accordance with relevant guidelines and regulations.
Participants
Older adults with MCI were recruited from community centers, nursing homes and long-term care facilities in Taiwan. The inclusion criteria were (1) age ≥ 65 years old, (2) MCI was determined by MMSE ≥ 24 and MoCA < 2652,53,54, and (3) the ability to walk for 60 s independently without any assistive device. The exclusion criteria included (1) unstable medical condition and (2) any neurological disease, psychological disorder, or learning disability known to interfere with participation in the study. Informed consent was obtained from all participants.
Outcome measures
The primary outcome was gait performance under dual task conditions, and the secondary outcomes included single walking performance, brain activation during walking, and cognitive function. Data for gait performance and brain activation were obtained simultaneously during 3 walking conditions described below. Participants were asked to sit on a chair for 60 s, and then to stand still for at least 15 s to stabilize the hemodynamic response before each walking trial. The participants were asked to walk back and forth on the hallway for 60 s in each walking trial. Each condition repeated twice with a total of 6 walking trials in a random order.
-
Single walking (SW): Participants were asked to walk at their self-selected speed.
-
Walking while performing a cognitive task: Participants were asked to walk at their self-selected speed while subtracting three from a random three-digit number serially.
-
Walking while performing a motor task: Participants were asked to walk at their self-selected speed while carrying a tray, with a cup of water on it, with both hands.
Gait performance
The gait performance was assessed by two wearable Physilog sensors (GaitUp system, Lausanne, Switzerland) attached to the lateral side of each shoe. The sensor was validated and had fair reliabilities (0.71–0.87) for measuring single and dual task walking performance34,55. The kinematic data was recorded and synchronized wirelessly for two sensors, and transferred to a tablet computer. Gait parameters included speed, cadence, stride length, stride time, and gait variability. The spatial and temporal gait variability were calculated as the coefficient of variation (= standard deviation/mean × 100%) of the stride length and stride time, respectively. To increase the measurement reliability, the gait parameters recorded in two trials of each walking condition were averaged for statistical analysis. In addition, to quantify the interference of additional task on walking, the dual task cost of gait speed (DTC) was calculated according to the following formula. The higher DTC value indicates the more interference caused by the additional task to walking speed.
DTC: dual task cost, SST: walking speed during single walking, SDT: walking speed during cognitive (motor) dual task walking.
Brain activation
A multichannel wearable functional near-infrared spectroscopy (fNIRS) imaging system (NIRSport, NIRx Medical Technologies LLC, Glen Head, NY, USA) was used to detect the cortical hemodynamic response to indicate the brain activation during walking. A total of 14 source-detector channels were arranged over the bilateral prefrontal cortex (PFC), premotor cortex (PMC), and supplementary motor cortex (SMA). The procedure of signal processing referred to our previous study1. The data was band-filtered (low-cutoff frequency 0.005 Hz, high-cutoff frequency 0.03 Hz), and wavelet filtering was used for the motion artifact correction in each channel. The preprocessed signals were converted to concentration in oxygenated (HbO) and deoxygenated hemoglobin (HbR) using the modified Beer–Lambert law56,57,58. The relative changes in HbO and HbR concentrations for each walking condition were obtained using a 5-s baseline collected before each session. The HbO and HbR changes were averaged over two repetitions for each walking condition (5–40 s after the onset) to improve signal-to-noise ratio. The index of hemoglobin differential was calculated by (Hbdiff = HbO − HbR) for further analysis. The Hbdiff values in multiple channels corresponding to each brain area were averaged to provide a better indication of hemodynamic response in the specific area (Supplementary Fig. 1). The fNIRS signals were processed using the HOMER2 package, and the calculation of the noise ratio and the Hbdiff values were performed using customized scripts developed on MATLAB (Mathworks, Natick, MA, USA).
Cognitive function
The cognitive function was assessed by the modified trail making test (TMT) and digit span test.
The TMT are widely used to evaluate executive function in different populations59. The modified version of TMT-A and B for the Chinese speakers were used in this study60. The time needed to complete each task was recorded for statistical analysis.
Digit span test was used to assess sustained attention and working memory61. Participants were asked to repeat series of numbers forward and backward instructed by the assessor. The total scores ranged from 0 to 28, and the higher scores indicated the better performance.
Interventions
Participants received 24 sessions of 45-min one-on-one training program according to their group assignment.
Participants in CDTT group practiced cognitive tasks during walking on level surface. The cognitive tasks included repeating phrases, counting number forward or backward, playing phonemic word chain games, reciting a poem, having conversations, and reciting a sentence backward.
Participants in MDTT group practiced motor tasks during walking on level surface. The motor tasks consisted of holding balls, raising an umbrella by both hands, waving a rattle, beating a castanet, bouncing a basketball, and holding one ball and concurrently kicking a basketball.
The complexity of walking for both dual-task training groups was modified by walking forward, backward and on an S-shaped route. The difficulty in tasks and walking complexity was progressively adjusted to challenge participants. The 8-week programs for the cognitive and motor dual-task training groups are shown in Supplementary Table 1.
Participants in CPT group received a multicomponent exercise program consisting of muscle strengthening, balance, and gait training for 15 min each. The strengthening exercise focused on the lower extremity muscles, including gluteal muscles, quadriceps, hamstrings, calf muscles and ankle dorsiflexors. The balance training included weight shifting to different directions while standing, tandem standing, standing on a foam, and one-leg standing. Participants were asked to walk forward, backward and on an S-shaped route during the gait training. The resistance for muscle strengthening, and the difficulty of the balance and gait training were adjusted accordingly as the participants progressed.
Statistical analysis
Non-parametric test was used for comparisons due to heterogeneity of the study sample tested by Shapiro–Wilk test. Intention-to-treat analysis was used for the missing data at follow-up assessment. Descriptive statistics were generated and presented in median (interquartile, IQR) for all variables. The between-group differences in basic data and outcome measures at pre-test were examined using Kruskal–Wallis test and Chi-square test. The within-group training effect on gait performance and cognitive function was evaluated by Friedman test in each group. The between-group differences were analyzed by Kruskal–Wallis test using change values, and post hoc analysis with Dunn–Bonferroni test. Epsilon-square estimate (ε2) of effect size was calculated for the between-group comparisons (ε2 = 0.02 as small, 0.13 as medium and 0.26 as large effect size)62. Change values were calculated by subtracting the pre-test data from the post-test or follow-up data. Spearman’s rank correlation coefficient was used to determine the correlation between the post-intervention changes in gait and brain activation during walking. All the data was analyzed by SPSS 24.0. The statistically significant level was set at 0.05.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
References
Lu, C. F., Liu, Y. C., Yang, Y. R., Wu, Y. T. & Wang, R. Y. Maintaining gait performance by cortical activation during dual-task interference: A functional near-infrared spectroscopy study. PLoS One 10, e0129390 (2015).
Liu, Y. C., Yang, Y. R., Tsai, Y. A., Wang, R. Y. & Lu, C. F. Brain activation and gait alteration during cognitive and motor dual task walking in stroke—A functional near-infrared spectroscopy study. IEEE Trans. Neural Syst. Rehabil. Eng. 26, 2416–2423 (2018).
Al-Yahya, E. et al. Cognitive motor interference while walking: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 35, 715–728 (2011).
Hollman, J., Kovash, F., Kubik, J. & Linbo, R. Age-related differences in spatiotemporal markers of gait stability during dual task walking. J. Geriatr. Phys. Ther. 29, 126–127 (2006).
Menant, J. C., Schoene, D., Sarofim, M. & Lord, S. R. Single and dual task tests of gait speed are equivalent in the prediction of falls in older people: A systematic review and meta-analysis. Ageing Res. Rev. 16, 83–104 (2014).
Hausdorff, J. M., Rios, D. A. & Edelberg, H. K. Gait variability and fall risk in community-living older adults: A 1-year prospective study. Arch. Phys. Med. Rehabil. 82, 1050–1056 (2001).
Cheng, S. J. et al. Gait performance and brain activities during cognitive and motor dual task in Prefrail elderly. Int J Gerontol 15, 53–57 (2021).
Leone, C. et al. Cognitive-motor dual-task interference: A systematic review of neural correlates. Neurosci. Biobehav. Rev. 75, 348–360 (2017).
Frith, C. & Dolan, R. The role of the prefrontal cortex in higher cognitive functions. Brain Res. Cogn. Brain Res. 5, 175–181 (1996).
Udina, C. et al. Functional near-infrared spectroscopy to study cerebral hemodynamics in older adults during cognitive and motor tasks: A review. Front. Aging Neurosci. 11, 367 (2020).
Bruijn, S. M., Van Dieën, J. H. & Daffertshofer, A. Beta activity in the premotor cortex is increased during stabilized as compared to normal walking. Front. Hum. Neusci. 9, 593 (2015).
Harada, T., Miyai, I., Suzuki, M. & Kubota, K. Gait capacity affects cortical activation patterns related to speed control in the elderly. Exp. Brain Res. 193, 445–454 (2009).
Suzuki, M. et al. Prefrontal and premotor cortices are involved in adapting walking and running speed on the treadmill: An optical imaging study. Neuroimage 23, 1020–1026 (2004).
Stuart, S., Alcock, L., Rochester, L., Vitorio, R. & Pantall, A. Monitoring multiple cortical regions during walking in young and older adults: Dual-task response and comparison challenges. Int. J. Psychophysiol. 135, 63–72 (2019).
Petersen, R. C. et al. Mild cognitive impairment: A concept in evolution. J. Intern. Med. 275, 214–228 (2014).
Muir, S. W. et al. Gait assessment in mild cognitive impairment and Alzheimer’s disease: The effect of dual-task challenges across the cognitive spectrum. Gait Posture 35, 96–100 (2012).
Montero-Odasso, M. et al. Quantitative gait analysis under dual-task in older people with mild cognitive impairment: A reliability study. J. Neuroeng. Rehabil. 6, 35 (2009).
Montero-Odasso, M. et al. Dual-tasking and gait in people with mild cognitive impairment. The effect of working memory. BMC Geriatr. 9, 1–8 (2009).
Doi, T. et al. Brain activation during dual-task walking and executive function among older adults with mild cognitive impairment: A fNIRS study. Aging Clin. Exp. Res. 25, 539–544 (2013).
Holtzer, R. & Izzetoglu, M. Mild cognitive impairments attenuate prefrontal cortex activations during walking in older adults. Brain Sci. 10, 415 (2020).
Bishnoi, A. & Hernandez, M. E. Dual task walking costs in older adults with mild cognitive impairment: A systematic review and meta-analysis. Aging Ment. Health 25, 1618–1629 (2021).
Shumway-Cook, A. & Woollacott, M. H. Motor Control: Translating Research into Clinical Practice (Lippincott, Williams & Wilkins, 2007).
Parvin, E., Mohammadian, F., Amani-Shalamzari, S., Bayati, M. & Tazesh, B. Dual-task training affect cognitive and physical performances and brain oscillation ratio of patients with Alzheimer’s disease: A randomized controlled trial. Front. Aging Neurosci. 12, 605317 (2020).
Gallou-Guyot, M., Mandigout, S., Bherer, L. & Perrochon, A. Effects of exergames and cognitive-motor dual-task training on cognitive, physical and dual-task functions in cognitively healthy older adults: An overview. Ageing Res. Rev. 63, 101135 (2020).
Gallou-Guyot, M., Mandigout, S., Combourieu-Donnezan, L., Bherer, L. & Perrochon, A. Cognitive and physical impact of cognitive-motor dual-task training in cognitively impaired older adults: An overview. Neurophysiol. Clin. 50, 441–453 (2020).
Law, L. L., Barnett, F., Yau, M. K. & Gray, M. A. Effects of combined cognitive and exercise interventions on cognition in older adults with and without cognitive impairment: A systematic review. Ageing Res. Rev. 15, 61–75 (2014).
Zhang, L. et al. Meta-analysis: Resistance training improves cognition in mild cognitive impairment. Int. J. Sports Med. 41, 815–823 (2020).
Reynolds, G. O., Willment, K. & Gale, S. A. Mindfulness and cognitive training interventions in mild cognitive impairment: Impact on cognition and mood. Am. J. Med. 134, 444–455 (2021).
Plummer, P., Zukowski, L. A., Giuliani, C., Hall, A. M. & Zurakowski, D. Effects of physical exercise interventions on gait-related dual-task interference in older adults: A systematic review and meta-analysis. Gerontology 62, 94–117 (2016).
Donnezan, L. C., Perrot, A., Belleville, S., Bloch, F. & Kemoun, G. Effects of simultaneous aerobic and cognitive training on executive functions, cardiovascular fitness and functional abilities in older adults with mild cognitive impairment. Ment. Health Phys. Act. 15, 78–87 (2018).
Delbroek, T., Vermeylen, W. & Spildooren, J. The effect of cognitive-motor dual task training with the biorescue force platform on cognition, balance and dual task performance in institutionalized older adults: A randomized controlled trial. J. Phys. Ther. Sci. 29, 1137–1143 (2017).
Horata, E. T., Cetin, S. Y. & Erel, S. Effects of individual progressive single-and dual-task training on gait and cognition among older healthy adults: A randomized-controlled comparison study. Eur. Geriatr. Med. 12, 363–370 (2020).
Fritz, N. E., Cheek, F. M. & Nichols-Larsen, D. S. Motor-cognitive dual-task training in persons with neurologic disorders: A systematic review. J. Neurol. Phys. Ther. 39, 142–153 (2015).
Soulard, J., Vaillant, J., Balaguier, R. & Vuillerme, N. Spatio-temporal gait parameters obtained from foot-worn inertial sensors are reliable in healthy adults in single- and dual-task conditions. Sci. Rep. 11, 10229 (2021).
Liu, Y. C., Yang, Y. R., Tsai, Y. A. & Wang, R. Y. Cognitive and motor dual task gait training improve dual task gait performance after stroke—A randomized controlled pilot trial. Sci. Rep. 7, 4070 (2017).
Hiyamizu, M., Morioka, S., Shomoto, K. & Shimada, T. Effects of dual task balance training on dual task performance in elderly people: A randomized controlled trial. Clin. Rehabil. 26, 58–67 (2012).
Doumas, M., Smolders, C. & Krampe, R. T. Task prioritization in aging: Effects of sensory information on concurrent posture and memory performance. Exp. Brain Res. 187, 275 (2008).
Rapp, M. A., Krampe, R. T. & Baltes, P. B. Adaptive task prioritization in aging: Selective resource allocation to postural control is preserved in Alzheimer disease. Am. J. Geriatr. Psychiatry 14, 52–61 (2006).
Karssemeijer, E. E., Aaronson, J. J., Bossers, W. W., Smits, T. T. & Kessels, R. R. Positive effects of combined cognitive and physical exercise training on cognitive function in older adults with mild cognitive impairment or dementia: A meta-analysis. Ageing Res. Rev. 40, 75–83 (2017).
Göthe, K., Oberauer, K. & Kliegl, R. Eliminating dual-task costs by minimizing crosstalk between tasks: The role of modality and feature pairings. Cognition 150, 92–108 (2016).
Pieruccini-Faria, F., Montero-Odasso, M. & Hausdorff, J. M. Gait variability and fall risk in older adults: The role of cognitive function. in Falls and Cognition in Older Persons: Fundamentals, Assessment and Therapeutic Options (eds. Montero-Odasso, M. & Camicioli, R.) 107–138 (Springer International Publishing, 2020).
Hobert, M. A. et al. Gait is associated with cognitive flexibility: A dual-tasking study in healthy older people. Front. Aging Neurosci. 9, 154–154 (2017).
Kortte, K. B., Horner, M. D. & Windham, W. K. The trail making test, part B: Cognitive flexibility or ability to maintain set?. Appl. Neuropsychol. 9, 106–109 (2002).
Bohannon, R. W. & Glenney, S. S. Minimal clinically important difference for change in comfortable gait speed of adults with pathology: A systematic review. J. Eval. Clin. Pract. 20, 295–300 (2014).
Lam, F. M. H. et al. Physical exercise improves strength, balance, mobility, and endurance in people with cognitive impairment and dementia: A systematic review. J. Physiother. 64, 4–15 (2018).
VanSwearingen, J. M. & Studenski, S. A. Aging, motor skill, and the energy cost of walking: Implications for the prevention and treatment of mobility decline in older persons. J. Gerontol. A Biol. Sci. Med. Sci. 69, 1429–1436 (2014).
Allali, G. et al. The neural basis of age-related changes in motor imagery of gait: An fMRI study. J. Gerontol. A Biol. Sci. Med. Sci. 69, 1389–1398 (2013).
Logan, J. M., Sanders, A. L., Snyder, A. Z., Morris, J. C. & Buckner, R. L. Under-recruitment and nonselective recruitment: Dissociable neural mechanisms associated with aging. Neuron 33, 827–840 (2002).
Erickson, K. I. et al. Training-induced functional activation changes in dual-task processing: An FMRI study. Cereb. Cortex 17, 192–204 (2007).
Sakai, K., Hikosaka, O. & Nakamura, K. Emergence of rhythm during motor learning. Trends Cogn. Sci. 8, 547–553 (2004).
Shadmehr, R. & Holcomb, H. H. Neural correlates of motor memory consolidation. Science 277, 821–825 (1997).
Nasreddine, Z. S. et al. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 53, 695–699 (2005).
Creavin, S. T. et al. Mini‐Mental State Examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. Cochrane Database Syst. Rev. (2016).
Liu-Ambrose, T. Y., Ashe, M. C., Graf, P., Beattie, B. L. & Khan, K. M. Increased risk of falling in older community-dwelling women with mild cognitive impairment. Phys. Ther. 88, 1482–1491 (2008).
Schwameder, H., Andress, M., Graf, E. & Strutzenberger, G. Validation of an IMU-System (Gait-Up) to identify gait parameters in normal and induced limping walking conditions. in 33rd ISBS-conference (ed. Floren Colloud, M. D. T. M.) (2015).
Kocsis, L., Herman, P. & Eke, A. The modified Beer–Lambert law revisited. Phys. Med. Biol. 51, N91-98 (2006).
Cope, M. & Delpy, D. T. System for long-term measurement of cerebral blood and tissue oxygenation on newborn infants by near infra-red transillumination. Med. Biol. Eng. Comput. 26, 289–294 (1988).
Boas, D. A. et al. The accuracy of near infrared spectroscopy and imaging during focal changes in cerebral hemodynamics. Neuroimage 13, 76–90 (2001).
Sánchez-Cubillo, I. et al. Construct validity of the Trail Making Test: Role of task-switching, working memory, inhibition/interference control, and visuomotor abilities. J. Int. Neuropsychol. Soc. 15, 438 (2009).
Lu, L. & Bigler, E. D. Normative data on trail making test for neurologically normal, Chinese-speaking adults. Appl. Neuropsychol. 9, 219–225 (2002).
Ruchinskas, R. Wechsler adult intelligence scale-digit span performance in subjective cognitive complaints, amnestic mild cognitive impairment, and probable dementia of the Alzheimer type. Clin. Neuropsychol. 33, 1436–1444 (2019).
Tomczak, M. & Tomczak, E. (2014) The need to report effect size estimates revisited An overview of some recommended measures of effect size. Trends Sport Sci. 1, 19–25.
Acknowledgements
This work was supported by grant from the Ministry of Science and Technology (MOST 106-2314-B-010-040-MY3) and National Health Research Institutes (NHRI-EX109-10913PI). We would like to thank all participants in this study.
Author information
Authors and Affiliations
Contributions
H.T.K., W.C.H., Y.R.Y. and R.Y.W. designed the study. H.T.K. and W.C.H. performed the experiments. Y.Y.L. helped recruiting participants. H.T.K. and N.C.Y. analyzed the data. H.T.K., N.C.Y. and R.Y.W. interpreted the data and prepared the manuscript. All authors reviewed the manuscript and approved the submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kuo, HT., Yeh, NC., Yang, YR. et al. Effects of different dual task training on dual task walking and responding brain activation in older adults with mild cognitive impairment. Sci Rep 12, 8490 (2022). https://doi.org/10.1038/s41598-022-11489-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-11489-x
- Springer Nature Limited
This article is cited by
-
Can transcranial direct current stimulation combined with interactive computerized cognitive training boost cognition and gait performance in older adults with mild cognitive impairment? a randomized controlled trial
Journal of NeuroEngineering and Rehabilitation (2024)